Andreasen JO, Andreasen FM, Skeie A, Hjørting-Hansen E, Schwartz O. Effect of treatment delay upon pulp and periodontal healing of traumatic dental injuries – a review article. Dent Traumatol. 2002; 18:116-128
Day P, Duggal M. A multicentre investigation into the role of structured histories for patients with tooth avulsion at their initial visit to a dental hospital. Dent Traumatol. 2003; 19:243-247
Von Arx T, Filippi A, Buser D. Splinting of traumatized teeth with a new device: TTS (Titanium Trauma Splint). Dent Traumatol. 2001; 17:180-184
DiAngelis AJ, Andreasen JO International Association of Dental Traumatology guidelines for the management of traumatic dental injuries: 1. Fractures and luxation of permanent teeth. Dent Traumatol. 2012; 28:2-12
Albadri S, Zaitoun H, Kinirons M. UK National Clinical Guidelines in Paediatric Dentistry. Treatment of traumatically intruded permanent incisor teeth in children. Int J Paediatr Dent. 1998; 8:289-293
Andreasen JO, Bakland LK, Matras R, Andreasen FM. Traumatic intrusion of permanent teeth. Part 3. A clinical study of the effect of treatment variables such as treatment delay, method of repositioning, type of splint, length of splinting and antibiotics on 140 teeth. Dent Traumatol. 2006; 22:99-111
Management of acute dental trauma. Pediatr Dent. 2004; 26:120-127
Albadri S, Kinirons M, Cole B, Welbury R. Factors affecting resorption in traumatically intruded permanent incisors in children. Dent Traumatol. 2002; 18:73-76
Humphrey JM, Kenny DJ, Barrett EJ. Clinical outcomes for permanent incisor luxations in a pediatric population I. Dent Traumatol. 2003; 19:266-273
Albadri S, Zaitoun H, Kinirons M. Treatment of traumatically intruded permanent incisor teeth in children.
Kenny DJ, Barrett EJ, Casas MJ. Avulsions and intrusions: the controversial displacement injuries. J Can Dent Assoc. 2003; 69:308-313
Andersson L, Andreasen JO, Day P International Association of Dental Traumatology guidelines for the management of traumatic dental injuries: 2. Avulsion of permanent teeth. Dent Traumatol. 2012; 28:88-96
Gregg TA, Boyd D. Treatment of avulsed permanent incisor teeth in children – British Society of Paediatric Dentistry. Int J Paediatr Dent. 1998; 8:75-81
Day P, Duggal M. Interventions for treating traumatised permanent front teeth: avulsed (knocked out) and replanted (Review). The Cochrane Library. 2010; 1:1-28
Andreasen JO, Andreasen FM, Mèjare I, Cvek M. Healing of 400 intra-alveolar root fractures. 2. Effect of treatment factors such as treatment delay, repositioning, splinting type and period antibiotics. Dent Traumatol. 2004; 20:203-211
Cvek M, Mèjare I, Andreasen JO. Conservative endodontic treatment of teeth fractured in the middle or apical part of the root. Dent Traumatol. 2004; 20:261-269
Taking the trauma out of trauma: an easy to follow guide for the management of trauma to the permanent dentition Ian White Gareth Spiers Dental Update 2024 40:8, 707-709.
Authors
IanWhite
BChD MFDS, GDP
Oakdene Dental Practice, 9 Long Lane, Holbury, Hants SO45 2LF, UK
Treatment of dental trauma can be an infrequent, unpredictable and stressful experience for a dental practitioner. Correct diagnosis and management of such cases is of primary importance in the prognosis of the affected dentition. We have therefore constructed a number of easy to follow algorithms in management, both short and long term, for the range of traumatic injuries that can affect the permanent dentition.
Clinical Relevance: Immediate as well as longer term management of dental trauma cases can be difficult, therefore a clear treatment plan is of great importance in successful results.
Article
Treatment of dental trauma can be an infrequent, unpredictable and stressful experience for the general dental practitioner. The presenting patient is often distressed, in pain and can arrive at any point during the day, making management of such cases particularly challenging.
Correct diagnosis and treatment of dental trauma injuries is of primary importance in the prognosis of the affected dentition.1 The purpose of this article is to condense neatly the short- and longer-term treatment options and needs for varying types of trauma to the permanent dentition. It does this by creating easy to follow algorithms that can be used as an aid when constructing a treatment plan, thus appropriate management can be taken, improving the prognosis of the affected teeth. However, each case should be assessed individually. Treatment plans should be constructed taking into account the patient's wishes after discussing the pros and cons of the different treatment options.
Where appropriate, always refer or seek advice from a specialist at the earliest opportunity. This is particularly important if you are in any doubt about the correct management, or you feel that the treatment needed is outside of your ability, as correct timings of treatment can affect outcomes. If there is a combination of injuries it may be appropriate to ask advice as the management of these cases can sometimes cause confusion. Behavioural or medical issues can complicate treatment, thus if you feel out of your depth seek advice and/or refer.
History
A comprehensive history and exam should be taken from all patients who have suffered dental trauma. A systematic approach to a traumatized child is essential for correct diagnosis and treatment:2
What is their complaint? – What are they most worried about?
When did the injury occur? – Date and time: particularly important with avulsion.
How did the injury happen? – High or low impact injury? Any chance of non-accidental injury?
Where did the injury happen? – Is there a risk of tetanus? Risk of infection?
Are there any other injuries? – Do they require treatment or investigations by other specialties? Should their management take priority over dental injuries?
Where are lost teeth fragments or avulsed teeth? – Is a chest or soft tissues X-ray needed to locate these?
What was the storage medium of any tooth/fragment?
From the history it is of primary importance to rule out a head injury. Any patient who has had dental trauma may also present with symptoms such as:
Loss of consciousness;
Amnesia;
Severe headaches;
Drowsiness;
Confusion;
Vomiting.
These symptoms should be taken seriously. If a patient presents with one or more of these post-injury they should immediately be sent to A&E with a covering letter so that more serious neurological injuries can be ruled out.
Dental history – How co-operative will the patient be with potentially prolonged treatment?
Relevant medical history – Are there any contra-indications to treatment?
Examination
Extra-oral exam
Check and record the following:
Any tenderness or reduced range of movement of neck – Can neck injury be ruled out?
Examine and feel all facial bones:
Supra- and infra-orbital rim – Any steps felt in the bone may be a fracture.
Nose – Check for deviations or flattening. This could suggest a fracture.
Mastoid – Bruising could indicate skull base fracture (as could CSF fluid from the ear).
Zygoma – Flattening of the facial contour may be due to fracture (excessive swelling can make this difficult to access).
TMJ – Check for tenderness.
Maxilla – Feel for movement with finger and thumb whilst supporting the forehead. Excessive movement may indicate mid face fracture.
Mandible – Check for areas of tenderness.
Mandibular movement – Extent of any trismus (normal opening 35–45 mm), range of movement laterally as well as protrusion (inability to protrude can indicate condylar fracture).
Note any lacerations – Is there any contamination that may require debridement of the wound? – Note the depth of the wound. – Are sutures required?
Note any bruising – This is sometimes suggestive of an underlying fracture.
Eye signs:
– Range of movement – Is there restricted movement anywhere? – This could suggest infra-orbital rim or zygoma fracture, especially if on upward gaze.
– Diplopia – Could indicate infra-orbital rim or zygoma fracture.
– Visual acuity – Check if the patient can read print at a distance of 1 m. Reduced acuity requires further investigations.
– Pupils' reaction to light – If pupils are unresponsive there may be an underlying neurological problem that will require immediate referral.
If possible facial bone fractures are suspected, then referral to a maxillofacial department is necessary. In the event of uncertainty, contact your local unit.
Intra-oral exam
Check and record the following:
Soft tissue damage – Sublingual haematoma is suggestive of mandible fracture.
Lacerations – Note size and position. If tooth fragments are lost, feel the area as they may be embedded within soft tissue. Are sutures required?
Teeth present – Check for damage to all teeth, not just the most severely damaged.
Mobility – f the fulcrum of movement is felt to be coronal to the apex this may indicate root fracture.
Occlusion – Any disruption due to traumatized tooth/teeth? Any steps suggestive of alveolar or mandible fracture?
Oral hygiene/periodontal health.
Type of injury to the affected teeth – Radiographs may aid diagnosis: remember to report on any radiographs taken.
For record keeping, photographs or drawings may be helpful.
Once a diagnosis has been made a treatment plan can be formulated. The algorithms that follow may be helpful in the process. Remember to discuss the options with the patient/guardian and the risks/benefits of treatment to gain informed consent.
Treatment plans must be flexible. A patient's desires or co-operation can change, or new factors can present. Always consider the long-term options and try to keep as many treatment avenues open to the patient. This is particularly important when the likely prognosis of the tooth is poor. Always refer early when orthodontic or surgical treatment may be required, or you feel that diagnosis, treatment or management is outside of your ability.
Guide to splinting
When splinting, ideally use titanium trauma splint3 with composite. However, if this product is not available, then an orthodontic wire with composite would be a reasonable alternative. Flexible fixation should allow physiological tooth movement to reduce the risk of ankylosis or resorption.3
Reposition tooth.
Cut wire/titanium trauma splint to correct length (one tooth either side of affected tooth/teeth).
Clean and dry the area.
Allow good moisture control with cotton wool rolls or rubber dam.
Etch affected teeth and one tooth either side.
Place bonding agent, air dry and light cure.
Apply composite to etched areas.
Place wire/titanium trauma splint into composite and light cure composite.
More composite can be placed over wire/titanium trauma splint to secure in place.
Smooth any sharp edges.
Ensure the splint does not irritate the soft tissues, can be easily cleaned, allows endodontic access and does not interfere with occlusion.
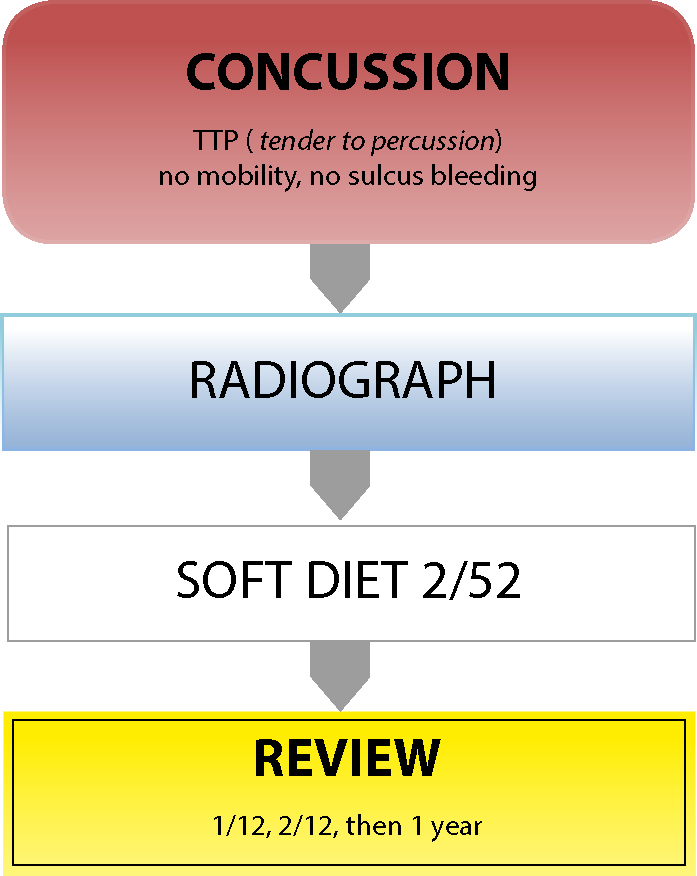
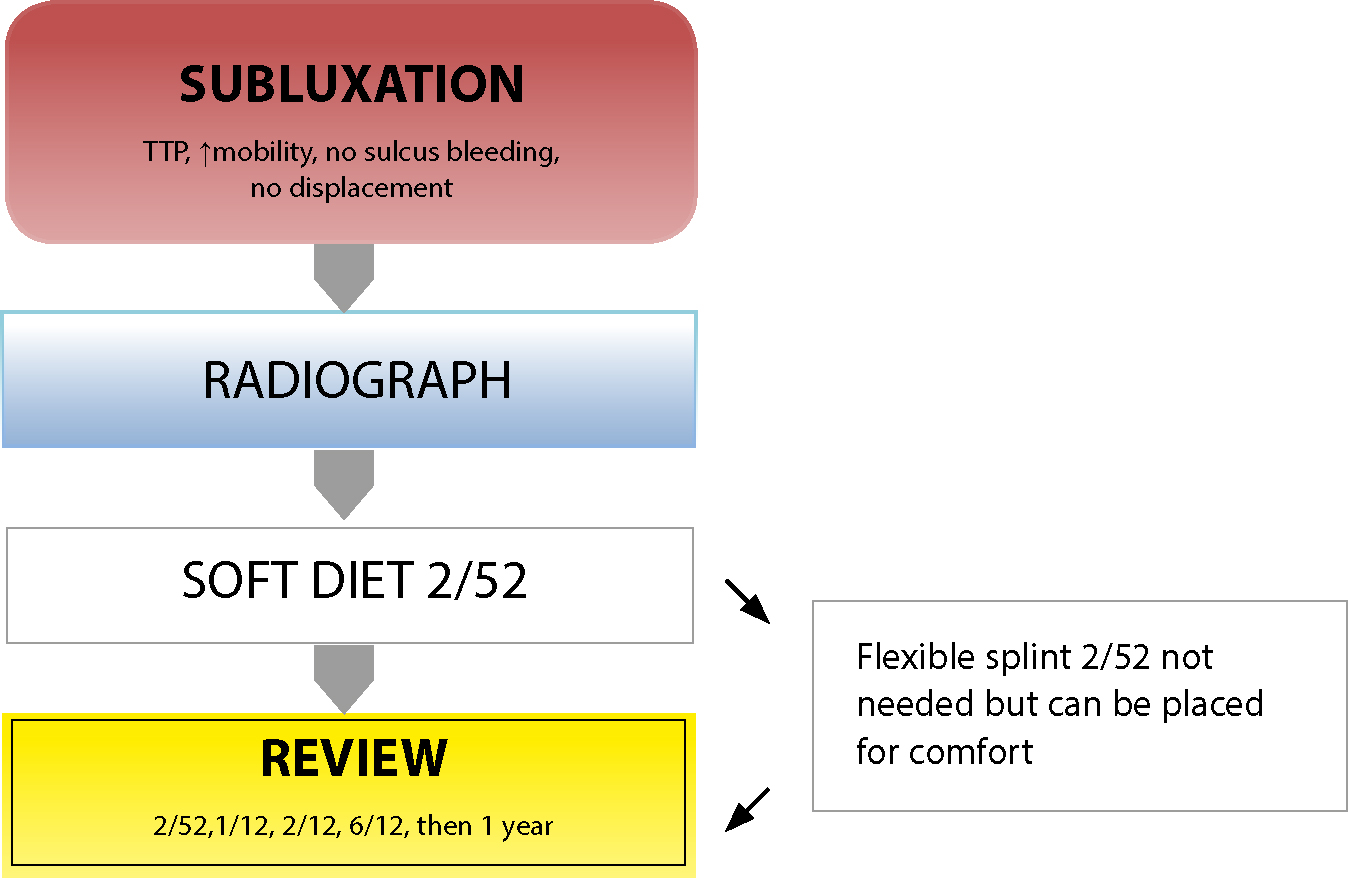
Concussion and subluxation
For both concussion (Figure 1) and subluxation (Figure 2) injuries, a radiograph should be taken to confirm diagnosis and as a reference for future radiographs. Soft diet and good oral hygiene should be advised for two weeks. For subluxation injuries, splinting is not required but can be placed for two weeks to aid comfort. Review the patient as the algorithm indicates.4 At these reviews, look for signs of pulpal necrosis using both visual and radiographic clues, as well as sensibility tests (be advised that false negatives are possible for 3/12). Treat necrosis if required.
Figure 1. Treatment for concussion.Figure 2. Treatment for subluxation.
Luxation
When treating luxation injuries (Figure 3), ensure a radiograph is taken to check position. Is it lateral, labial or palatally displaced, and are other adjacent teeth affected by this? Reposition the tooth using local anaesthetic. Forceps may be required if a bony lock has occurred, particularly if displacement is palatally. If the patient has presented after some time, repositioning may not be possible and orthodontic repositioning may be required, thus an immediate referral is needed. However, owing to possible occlusal interference and likely fracture of alveolar bone, orthodontic repositioning can be time consuming, therefore all attempts should be made to reposition the tooth immediately to give the best chance for successful results.
Figure 3. Treatment for luxation injuries.
If it is possible to reposition immediately, then place a flexible splint for four weeks4 after checking correct position with a radiograph. Advise soft diet for that period as well as good oral hygiene with the use of chlorhexidine. Review at two weeks, then one, two and six months post incident, followed by yearly for five years. At these reviews, check for signs of pulpal necrosis and RCT (root treat) or extract, if indicated, depending upon the patient's wishes.
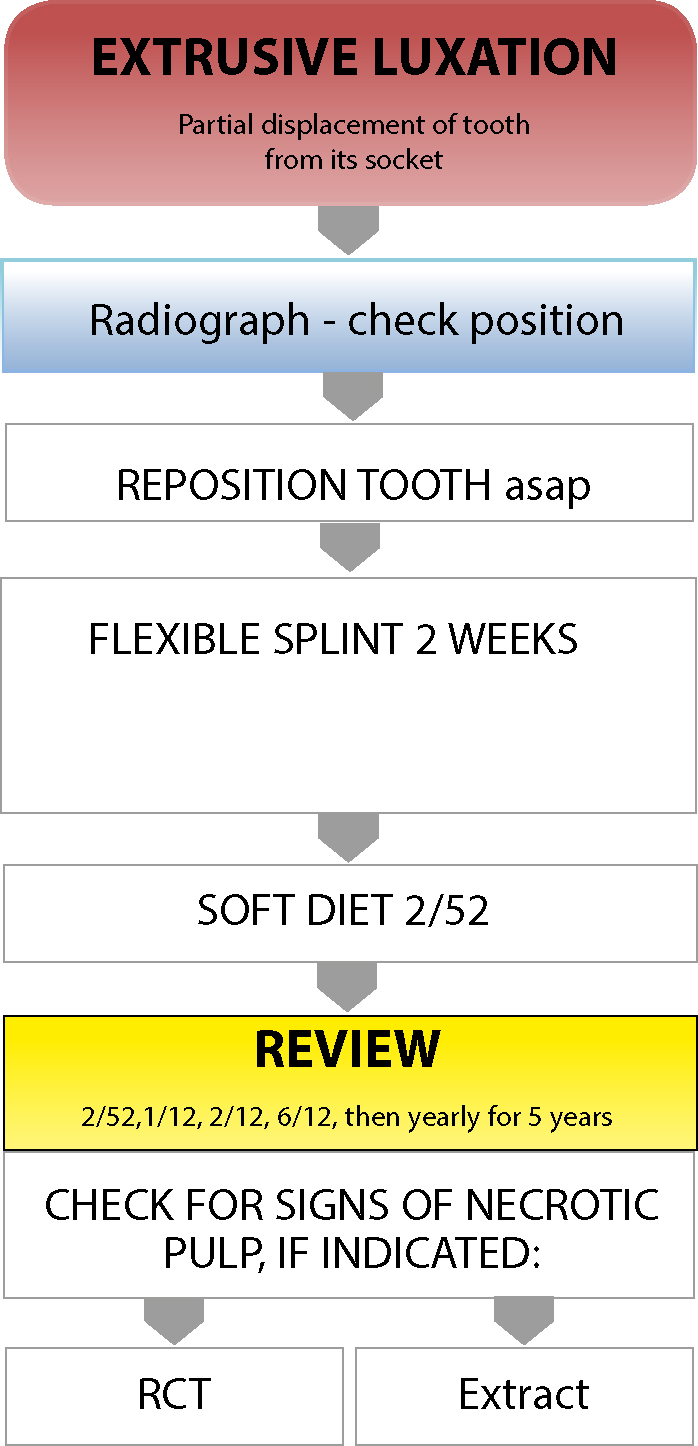
Extrusion
For extrusive luxation (Figure 4), treat as for luxation injuries. However, when splinted, do so with a flexible splint for two weeks.4 Review the patient at the same intervals, again treating any pulpal necrosis as necessary.
Figure 4. Treatment for extrusion injuries.
Intrusion
When treating a patient for intrusion (Figure 5) take a radiograph to confirm diagnosis and for record keeping. From the radiograph, confirm whether the root formation is complete or incomplete. The degree of intrusion in centimetres should also be measured.
Figure 5. Treatment for dental intrusion.
With all intrusion injuries there is the need or the potential need for specialist treatment, either orthodontic or surgical. Therefore, it is advisable to consult with a specialist after the initial assessment of the patient, who may wish to review the case him/herself.
With intrusion injuries there also is a high risk of root resorption with potential tooth loss in the long term.5 Therefore, it would be appropriate to inform the patient of this and discuss potential treatment options for replacement if the tooth were to be lost in the future.
When the root formation is complete, passive re-eruption is unlikely, especially if over the age of 17.6 In these cases, if intrusion is between 3 mm and 7 mm, rapid orthodontic or surgical repositioning is likely to be required to move the tooth back to its functional position.4 Therefore, an immediate referral is needed. However, if intrusion is less than 3 mm, there is still some potential for re-eruption, and it is advised to monitor the situation for up to three weeks to see if this occurs. If adequate re-eruption does not occur, then rapid orthodontic or surgical reposition will be required. It may be advisable to seek advice from a specialist after the initial assessment in these cases, before the monitoring period starts. Specialists may wish to review the patients themselves as there is an increased risk of ankylosis the longer the time since trauma.
Also, when the root formation is complete, intrusion is likely to result in pulp necrosis, therefore pulp extirpation and non-setting calcium hydroxide should be placed 2–3 weeks after the tooth has been repositioned;4 this should reduce the chance of inflammatory-induced root resorption. The root filling can be completed at a later appointment. If intrusion is greater than 7 mm, the prognosis is poor, with root resorption and subsequent loss the most likely outcome.7,8,9 However, there are a number of options available, depending upon the patient's wishes and co-operation. An extraction could be performed, however, the patient needs to understand the impact that this could have on future treatment options. Surgical repositioning may be necessary if the patient is keen to try and retain the tooth/teeth, therefore an immediate referral should be made.4,9,10 Once repositioned, root treatment will be required. The patient should be informed that eventually there is a good chance that the tooth will be lost due to the very high risk of root resorption.5 A further option would be to extract the tooth and re-implant, treating it as an avulsion;10 however, it would be advisable to consult a specialist before embarking on this treatment plan.
When the root formation is incomplete (Figure 5), assess the degree of intrusion. If less than 3 mm, then leave to re-erupt.4,9,10,11 If this has not occurred within three weeks, then orthodontic repositioning will be required. If the intrusion is between 3 mm and 7 mm, the tooth may re-erupt but will likely need orthodontic repositioning.4 If greater than 7 mm intrusion, then surgical or orthodontic repositioning will be required.4 In all these cases, if a referral is required, do so at the earliest opportunity. With undeveloped roots, intrusion does not always result in pulp death; therefore review at two weeks, one, two, and six months, then yearly for five years, checking for signs of pulpal necrosis and treating as necessary.
All teeth, irrespective of their root form, that have been repositioned by orthodontics or surgically, require the placement of a flexible splint for 4–8 weeks post repositioning.4
Avulsion
During history and examination, assess whether treatment is appropriate. In certain situations, replantation is not indicated, such as severe caries, periodontal disease, non-cooperative patient or if the tooth is very immature, ie has just erupted into occlusion.
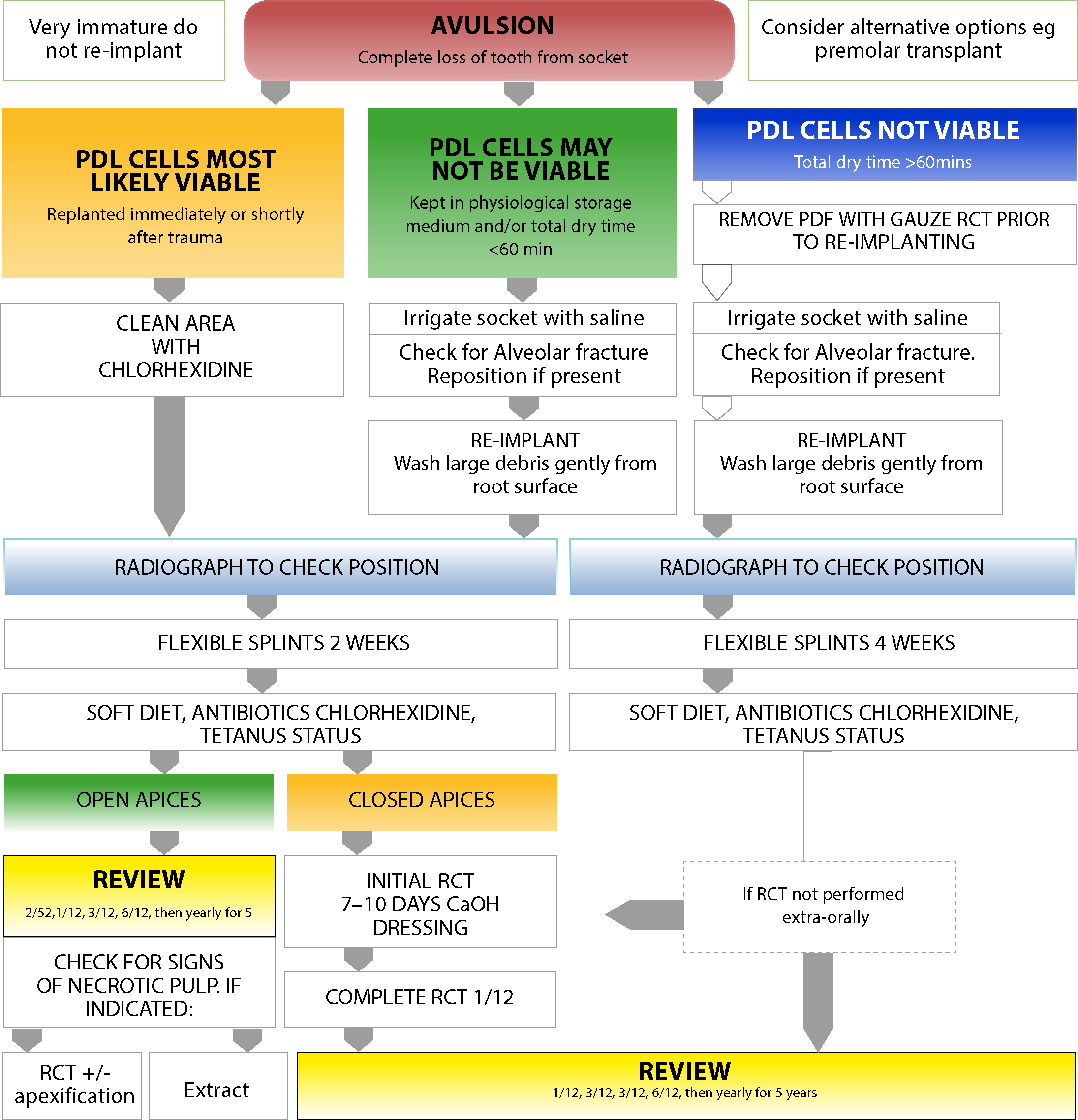
Before treatment for avulsed teeth (Figure 6), the dentist needs to make a decision on what he/she feels the health of the periodontal ligament (PDL) cells are likely to be, as the prognosis and subsequent treatment pathways of avulsed teeth are dependent upon the health of these cells. This in turn is affected by the extra-oral time (especially dry time) and storage medium.12 Therefore, these two pieces of information are essential to obtain during history-taking to ensure that the correct treatment pathways are followed.
Figure 6. Treatment for avulsion.
The scenario that leaves the PDL cells most likely to be viable is if the patient presents having had the avulsed tooth replanted immediately, or soon after, the incident.12 The next most favourable scenario is if there has been a total extra-oral dry time of less than 60 minutes,12 in which case, the PDL cells may be viable but have been compromised. This 60 minutes does not include time when the tooth has been within a physiological or osmolality balanced storage medium (eg tissue culture medium, Hank's Balanced Salt Solution [HBSS], saline, milk or saliva). Time spent within non-physiologic storage medium, eg tap water or chlorhexidine, should be considered the same as extra-oral dry time. The final scenario is that where the tooth has had a total extra-oral dry time (including time spend within non-physiologic storage medium) of greater than 60 minutes. In this case, all the PDL cells are considered to be non-viable.12
Another important factor that influences treatment decisions is the extent of root formation. The most appropriate way to access this is radiographically once the tooth has been replanted, or visually prior to replanting.
In the situation of a patient presenting having had the avulsed tooth replanted immediately or soon after the incident, the area should be cleaned with chlorhexidine, a radiograph taken to check position, and repositioning carried out, if necessary. Once positioned correctly, a flexible splint is placed for two weeks.11,12 During this period, the patient is advised to eat a soft diet, use chlorhexidine mouthwash and perform thorough oral hygiene. A short course of antibiotics may be required12 and a tetanus booster may also be needed if the tooth has come into contact with soil, in which case the patient should be advised to see a physician.
If the apex is closed, then initial root treatment should take place just prior to splint removal, placing non-setting calcium hydroxide.12,13 This root treatment should be completed at the one month review. If the apex is open, then there is a chance of revasculation of the pulp, therefore review as the algorithm indicates, checking for signs of necrosis. If necrosis occurs then decide with the patient whether to root treat with or without apexification or extract. With both open and closed apices, review the patient regularly, checking for signs of resorption or ankylosis, discussing treatment options if this occurs.
If the tooth has been kept in a physiological storage medium and/or stored dry with a total dry time less than 60 minutes, the PDL cells may be viable but compromised.12 The tooth is replanted with local anaesthetic after gently washing any large debris from the root surface. If a clot is present in the socket, irrigate with saline and use suction prior to insertion. Check for any alveolar fractures and reposition if required. Gently replant the tooth and check position with a radiograph. Continue treatment as for immediately replanted teeth, depending on whether there is an open or closed apex.
With a total dry time and time within non-physiologic medium of 60 minutes or more, all the PDL cells should be considered non-viable and periodontal healing is unfavourable.12 As further handling and drying of the root is unlikely to worsen the prognosis, root treatment can be performed outside the mouth prior to re-implanting.12,14 As the PDL cells will be dead, it should be removed using gauze prior to reinsertion.12 In this situation, replacement resorption and ankylosis may be considered an acceptable outcome as the replanted tooth may last for a number of years, maintaining bone. However, in young patients, infra-occlusion may result in gingival irregularity which could result in poor aesthetics. This should be monitored during review visits and, if present, advice could be sought regarding decoronating. Splint using a flexible splint for four weeks,12 advising soft diet, chlorhexidine mouthwash and good oral hygiene for two weeks. A short course of antibiotics may be required. Review the patient at splint removal, then three and six months post-trauma, followed by yearly for five years. Referral for an opinion regarding premolar implants could be considered, if the patient is of the appropriate age.
Fractures
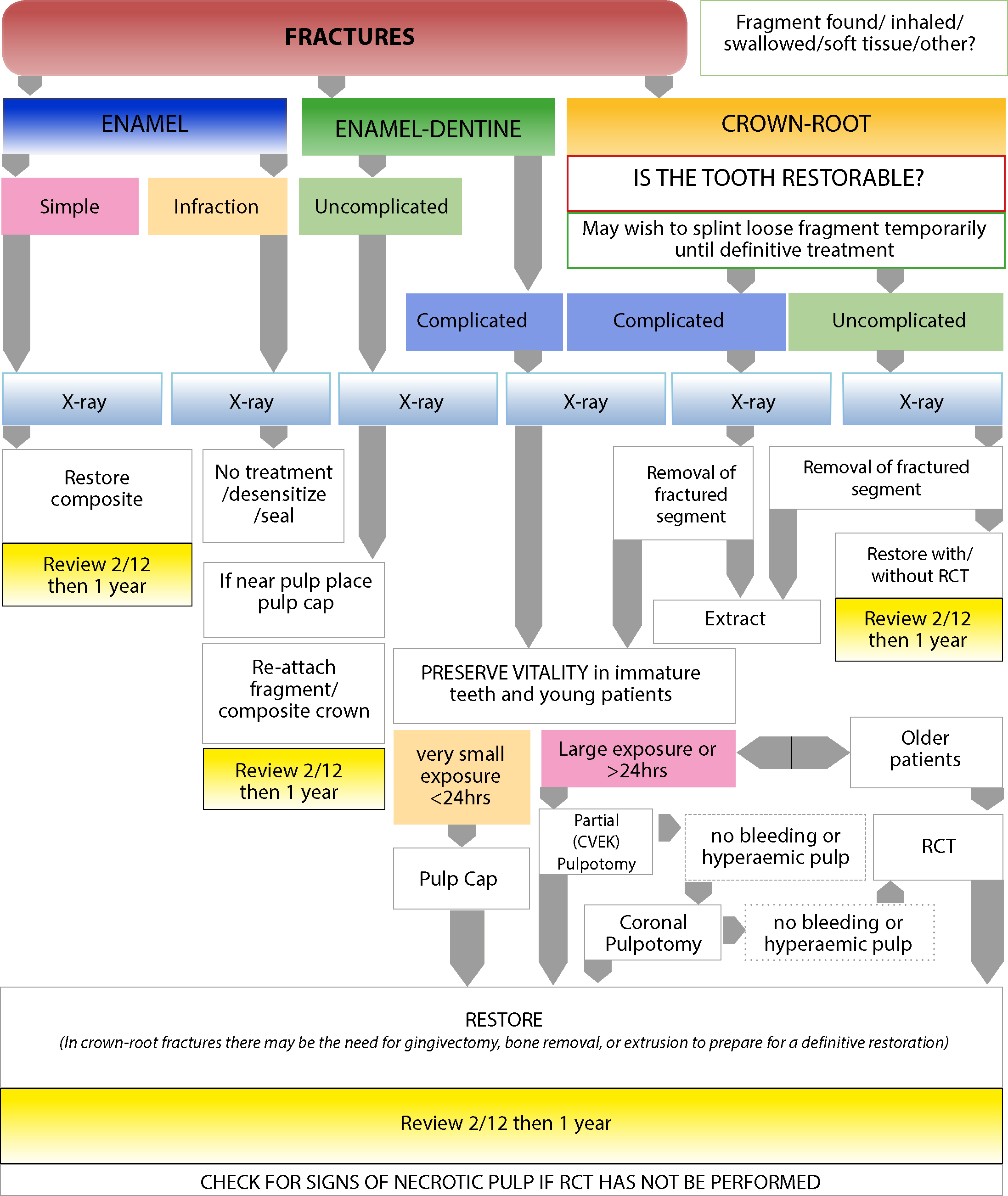
During the history and exam when a dental fracture (Figure 7) has occurred, check that all the fragments have been accounted for, as there is always a risk that they have been inhaled, swallowed or are within soft tissue.
Figure 7. Treatment for fracture injuries.
No treatment is needed unless symptomatic for infractions,4,11 however, for enamel fractures restore with composite.
For enamel-dentine fractures, assess whether pulpal exposure has occurred (complicated). If no exposure has occurred (uncomplicated) then simply place a composite restoration or re-attach fragment using composite.4,11 If the fracture is near the pulp (0.5 mm appearing pink) but without exposure, a dressing of calcium hydroxide or mineral trioxide aggregate (MTA) over the pulp area (pulp cap) may be advisable.
If a pulpal exposure is present, then preserving the vitality is of primary importance. This is especially true if the tooth is not fully matured, to allow continued root development.
For small exposures (less than 2 mm) that happened less than 24 hours previously, place a dressing material such as calcium hydroxide or MTA over the traumatized pulp (pulp cap) and restore with a plastic restoration.7,15 For larger exposures, greater than 2 mm and/or when exposure has been for greater than 24 hours, it is possible to amputate the infected/inflamed portion of the pulp (partial pulpotomy (Cvek)).11,15 If no bleeding at all is seen, or the pulp is hyperaemic during the partial pulpotomy, the healthy portion of the pulp has not been reached. Therefore, there is the need to progress towards a full coronal pulpotomy.
Remove pulp in 1–2 mm increments until only slight bleeding is seen. Once healthy pulp tissue is reached, place a dressing material and restore. If there is still no sign of bleeding or a hyperaemic pulp is still present, then a pulpectomy with root treatment is required.15
These treatment options are best used when treating younger patients. With older patients, full root treatment may be a more appropriate option,4 especially with large or contaminated exposures. Also always consider if the tooth is restorable before embarking on prolonged treatment. This is especially true with crown-root fractures, as, to restore, gingivectomy or extrusion may need to be considered if the fracture goes very subgingival.4 Review teeth with complicated fractures after two months, then one year after pulp treatment, checking for signs of pulpal necrosis or periradicular disease and treating as necessary.
During the initial management of crown-root fractures, it may be appropriate to splint the fractured segment temporarily to provide comfort until definitive treatment can be done.4,11 As with enamel-dentine fractures, assess whether the fracture is complicated or uncomplicated. For uncomplicated fractures, remove the fragment and restore with or without RCT,4 or extract if the tooth is thought to be unrestorable or if the patient requests extraction. For complicated fractures, remove the fragment and either extract the tooth or treat as like a complicated enamel-dentine fracture, with pulp treatment or RCT before restoring.4,11 It should be considered that, to restore crown-root fractures, there may be the need for a gingivectomy, with or without bone removal, or for the tooth to be extruded. Either of these may require a specialist referral.
Root fractures
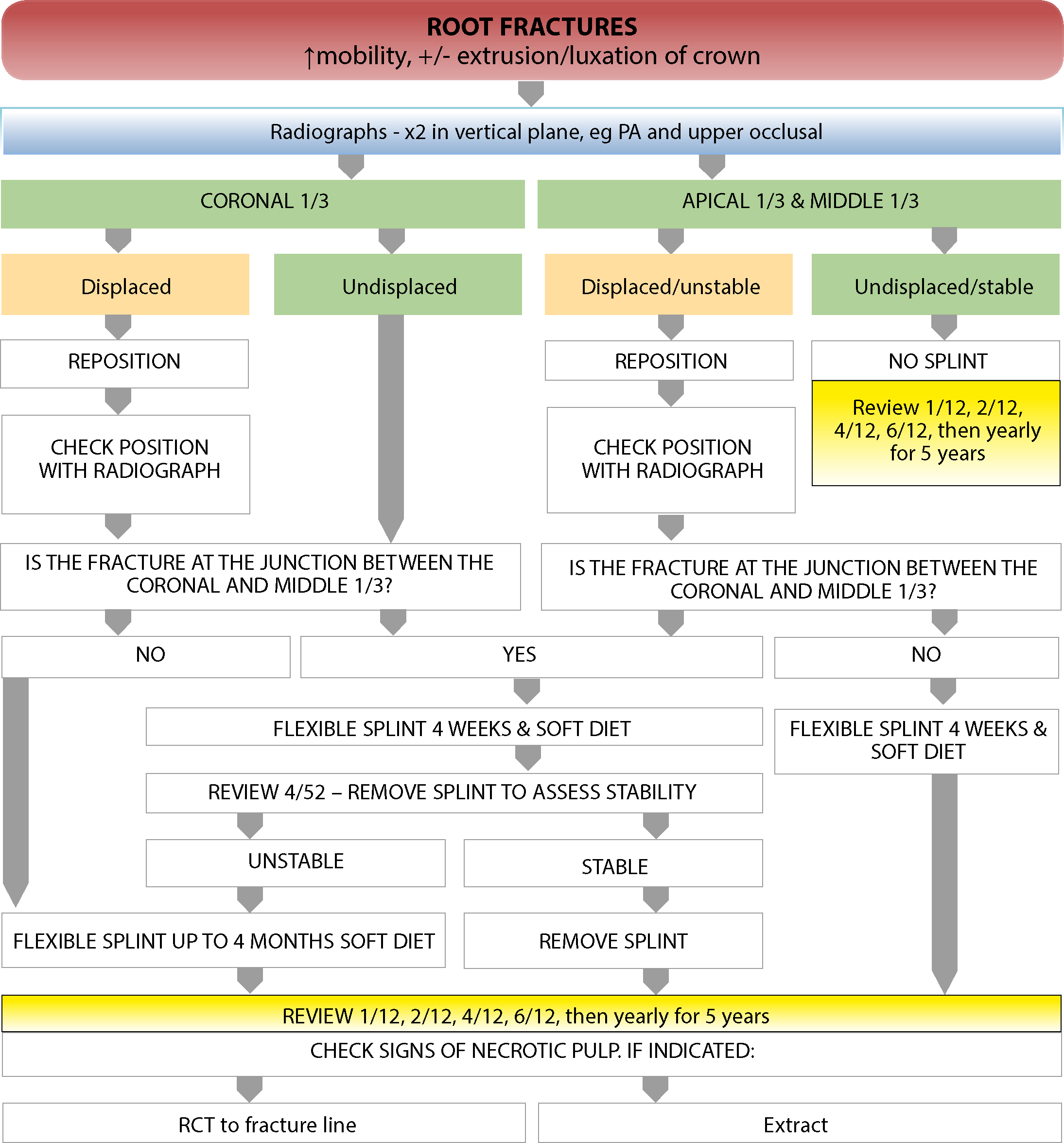
If a potential root fracture is suspected (Figure 8), two radiographs will be required at different planes to assess the position of the fracture. To get an indication of the position of the fracture, feel where the fulcrum of movement is when checking for mobility.
Figure 8. Treatment for root fracture injuries.
If the fracture is in the coronal third, it will require repositioning if displaced and splinted for up to four months with a flexible splint.4 These fractures are often very unstable and this should allow enough time for hard callus formation. Advice should be given regarding soft diet and oral hygiene during this period. The patient should be reviewed at 1, 2, 4 and 6 months, then yearly for 5 years, checking for signs of a necrotic pulp.4 If indicated, apply root treatment to the fracture line4,16 or extract.
If the fracture is found to be at the apical or middle third and is stable, no splint is required,15 but soft diet should be advised. However, for displaced or unstable fractures, repositioning will be required and a flexible splint should be placed for up to four weeks,4 in addition to soft diet. Again, review after one, two, four and six months, then yearly for five years. Be vigilant for signs of necrosis that would require root treatment to the fracture line16 or extraction.
If, however, the fracture occurs between the middle and coronal third and length of splint time is uncertain, it is advised to splint for four weeks then review the case.4 If the fractured portion is stable after this time, the splint can be removed. However, if there is still pronounced instability, continue to splint for up to four months.4
Alveolar fractures
When treating alveolar fractures (Figure 9) a radiograph is taken to confirm diagnosis. An OPT or occlusal are the most appropriate for this purpose. Reposition the fracture and splint with a flexible splint for 4 weeks.4 Review the patient after 1, 2, 4 then 6 months, followed by yearly for 5 years. At these reviews, assess the prognosis of the affected teeth and treat as necessary.
Figure 9. Treatment for alveolar fracture injuries.
Conclusion
In all stressful situations, having a structured pathway of management can reduce uncertainty and improve outcomes. These algorithms are not set in stone however. Always apply common sense, work within your abilities and, whenever in doubt, refer early.