Smitha T, Venkatesh D, Veeresh M The cusp of Carabelli: Frequency, distribution and type in the Bengaluru population. J Oral Maxillofac Pathol. 2018; 22:418-422 https://doi.org/10.4103/jomfp.JOMFP_254_18
Mallineni SK, Panampally GK, Chen Y, Tian T. Mandibular talon cusps: A systematic review and data analysis. J Clin Exp Dent. 2014; 6:e408-13 https://doi.org/10.4317/jced.51476
Mavrodisz K, Rózsa N, Budai M Prevalence of accessory tooth cusps in a contemporary and ancestral Hungarian population. Eur J Orthod. 2007; 29:166-169 https://doi.org/10.1093/ejo/cjl084
Welbury R., 5th edn. Oxford: Oxford University Press; 2018
Rao YG, Guo LY, Tao HT. Multiple dens evaginatus of premolars and molars in Chinese dentition: a case report and literature review. Int J Oral Sci. 2010; 2:177-180 https://doi.org/10.4248/IJOS10052
Levitan ME, Himel VT. Dens evaginatus: literature review, pathophysiology, and comprehensive treatment regimen. J Endod. 2006; 32:1-9 https://doi.org/10.1016/j.joen.2005.10.009
Oehlers FA. Dens invaginatus (dilated composite odontome). I. Variations of the invagination process and associated anterior crown forms. Oral Surg Oral Med Oral Pathol. 1957; 10:1204-1218 https://doi.org/10.1016/0030-4220(57)90077-4
Ridell K, Mejàre I, Matsson L. Dens invaginatus: a retrospective study of prophylactic invagination treatment. Int J Paediatr Dent. 2001; 11:92-97 https://doi.org/10.1046/j.1365-263x.2001.00234.x
Alani A, Bishop K, Knox J. Dens invaginatus as a microsymptom of canine ectopia: a case series. Orth Update. 2009; 2:90-93
Ash MM, Nelson SJ. Wheeler's Dental Anatomy, Physiology, and Occlusion, 8th edn. St Louis, MO, USA: Elsevier; 2003
Orton-Gibbs S, Crow V, Orton HS. Eruption of third permanent molars after the extraction of second permanent molars. Part 1: assessment of third molar position and size. Am J Orthod Dentofacial Orthop. 2001; 119:226-238 https://doi.org/10.1067/mod.2001.111556
Dens invaginatus occurs in varied forms with potential impact on the restorability, potential for pulpal infection of the tooth and difficulty in undertaking endodontic treatment of the tooth. Diagnosis of dens invaginatus and the particular type of dens invaginatus can be challenging. This article describes abnormality of crown morphology, a classification of dens invaginatus, and its pathology and illustrates the diagnosis and management of an unusual case of dens invaginatus in a maxillary left second permanent molar diagnosed with the help of CBCT.
CPD/Clinical Relevance: Dens invaginatus is a common occurrence and therefore all dentists need to have an appreciation of it.
Article
Anomalies of tooth formation can be difficult to decipher clinically. Teeth can be anomalous in size, structure, number and shape. Anomalies of the cuspal morphology can take the form of accessory cusps, dens evaginatus, and dens invaginatus (Figure 1).
Figure 1. Illustration of dens evaginatus and dens invaginatus.
Additional cusps are common and usually affect molar teeth. The most common is the cusp of Carabelli on the mesio-palatal line angle of the upper first permanent molar, which is present in 87% of the population1 and thus, may be considered normal. Incisors can have additional cusps from the palatal cingulum, ‘talon cusps’. These have a prevalence of 0.06–7.7%2 and occur most commonly in maxillary lateral incisors. The aetiology of accessory cusps is unknown. Genetic and exogenous factors may combine together to cause the cusp to develop.3 Additional cusps may be problematic for occlusal interference and aesthetics. They are often treated by repeatedly grinding the cusp over an extended period to reduce the height and allow reactionary dentine to form,4 but careful radiographic examination, ideally CBCT, should be carried out to find the exact extent of pulpal involvement and avoid an exposure. Selective grinding can have varied success, depending on the size of the cusp.
Dens evaginatus is uncommon and is almost exclusively found in patients of Chinese descent, affecting 1–4% in this group.5 It manifests as a tubercle from the occlusal surfaces of posterior teeth, second molars most commonly, and lingual surfaces of anterior teeth. The tubercle has similar tooth tissue, pulp covered by dentine and enamel. They form from unusual proliferation of the inner enamel epithelium into the stellate reticulum of the enamel organ.6 They are normally fractured off or worn down and are vulnerable to pulp exposure.7 Some authors believe the talon cusp should be differentiated from dens evaginatus because of its site, prevalence and appearance8 whereas others assert that they are the same type of anomaly.7
Dens invaginatus is an infolding within the crown of the tooth lined by enamel. It can range from a mild enamel-lined pitting that ends as a blind sac inside the crown, to an invagination extending through the crown and root and exiting through the periodontal ligament.9 It is caused by the inner enamel epithelium invaginating into the dental papilla prior to calcification.10
The most common classification of dens invaginatus is that of Oehlers (Figure 2).11 This is based on the extension of the invagination from the coronal to the apical hard tissue and its association with the periodontal tissues. Type I is the most commonly observed, being found in 79% of all dens invaginatus, and often seen on the palatal aspect of maxillary lateral incisors, followed by type II (15%) with type III (5%) being the rarest.12 Recognizing dens invaginatus appropriately is important because it may be vulnerable to caries and precipitate peri-apical pathology.13
Figure 2. Illustration of Oehler's classification of dens invaginatus. Type I: mild invagination within the crown of the tooth and not going beyond the cemento-enamel junction. Type II: the invagination extends to the root, but does not communicate with the periodontal ligament. Type IIIA: the invagination extends through the root to the peri-apical tissues laterally through an extra foramen. It is not in association with the pulp. Type IIIB: the invagination extends through the root to the to the peri-apical tissues at the apical foramen. There is normally no association with the pulp.
SEDENTEXCT (Safety and Efficacy of a New and Emerging Dental X-ray Modality) produced definitive guidelines for cone beam CT for dental and maxillofacial radiology.14 Regarding endodontics, the guidelines conclude that CBCT is not indicated as a standard method for demonstration of root canal anatomy. However, limited-volume, high-resolution CBCT may be indicated for cases where intra-oral radiographs give equivocal, or inadequate, information for treatment planning. Furthermore, it highlights atypical pulp anatomy as an indication.
This article uses a clinical case to illustrate unusual crown morphology where diagnosis may be challenging and may influence the long-term prognosis of a tooth.
Case report
An 18-year-old fit and well male presented to an orthodontic specialist practice 3 years following completion of his orthodontic treatment. He complained of swelling associated with his maxillary left second molar. This had been causing some pain and discomfort.
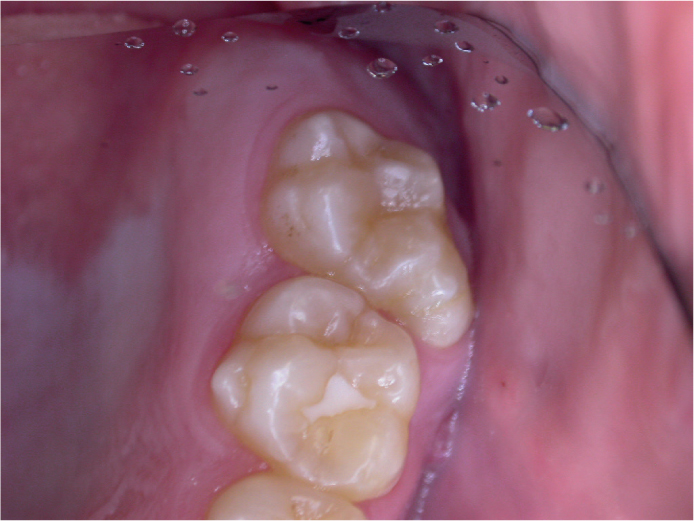
On examination, there was a buccal swelling overlying the maxillary left second molar (UL7) (Figure 3) and the morphology of this tooth was unusual. Usually, the maxillary second molar has four cusps, two buccal and two palatal, a rhomboid-shaped occlusal surface, a large mesial fossa and smaller distal fossa.15 The presenting maxillary second molar had an additional cusp on the mesiobuccal aspect of the crown (Figure 4).
Figure 3. Left buccal view demonstrating swelling associated with UL7.Figure 4. Occlusal view demonstrating unusual morphology of the UL7.
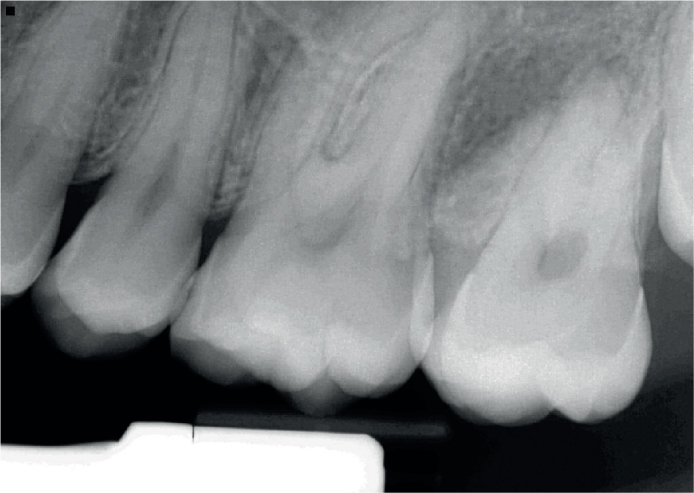
The tooth was tender to percussion, but positive to ethyl chloride cold sensitivity testing. It was not mobile, and was examined by a specialist periodontist who confirmed that periodontal probing was normal. Panoramic radiological examination revealed unusual root morphology of UL7 compared with UR7 and a peri-radicular radiolucency associated with the mesial aspect of the UL7 (Figure 5). The peri-radicular pathology is more evident on the intra-oral peri-apical radiograph (Figure 6)
Figure 5. Panoramic radiograph demonstrating unusual root morphology of UL7 in comparison to UR7.Figure 6. Intra-oral peri-apical radiograph demonstrating peri-apical pathology and dens invaginatus canal from the occlusal surface.
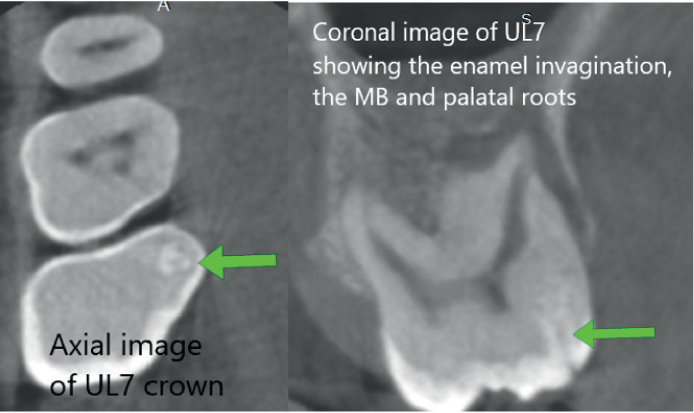
A cone beam computed tomograph (CBCT) of the upper left maxillary teeth was taken and reported by a dental and maxillofacial radiologist. This showed the additional cusp on the mesio-buccal aspect in the 3D view (Figure 7). There was a dens invaginatus extending from the enamel surface of the extra cusp communicating with the pulp (Figure 8). There were three roots, mesio-buccal, disto-buccal and palatal, and the mesio-buccal root had an unusual morphology with the root split apically to form an MB1 and MB2 apex. The MB1 canal was wide with a wide apical foramen, the MB2 had a very fine canal. There was a peri-apical pathology at the mesio-buccal apex that also tracked along the mesio-buccal aspect of the mesio-buccal root and breached the buccal bone in the crestal region (Figure 9).
Figure 7. CBCT 3D image of occlusal surface.Figure 8. Sagittal view of CBCT demonstrating the split in the root canal in the mesio-buccal root into a wide open MB1 canal and a very fine MB2.Figure 9. Axial view showing the site of the dens invaginatus and coronal view showing the extent of the dens invaginatus into the coronal structure.
The patient was referred to an endodontist who felt that root canal therapy, while possible, had a high risk of failure owing to the complex canal architecture. Orthodontic review confirmed that, as the patient had an unerupted UL8, it was likely that if the UL7 was extracted UL8 would drift into its space.
Discussion
The diagnosis was of an additional cusp associated with a dens invaginatus. The Oehlers classification (Figure 1) for dens invaginatus is more commonly applied to incisor teeth, but could also be applied to a molar.3 The presence and nature of the dens invaginatus is not readily apparent on the peri-apical radiograph. However, the CBCT showed the dens invaginatus was contained within the crown of the tooth, with little or no extension beyond the cemento-enamel junction. Therefore, it would be best considered to be a type I dens invaginatus. It did communicate with the pulp allowing bacterial ingress and an inflammatory reaction. The pulpal tissue in the MB root subsequently became necrotic and periradicular pathology developed around this root. The multi-rooted tooth is likely to have developed only a partial necrosis, accounting for the positive response to cold testing and the lack of peri-apical pathology at the disto-buccal and palatal oots.
The CBCT allowed an accurate diagnosis and provided the information about the root morphology and likelihood of successful root canal treatment. This proved valuable as it showed the root morphology was too complex to easily find the canals, instrument them sufficiently to allow proper cleaning and finally obturate to achieve a hermetic seal and prevent proliferation of micro-organisms in the root canal space. Clinically, the enamel dens invaginatus was not clear.
Extraction of the second molar was therefore advised as the tooth was of uncertain prognosis and the third molar was still unerupted. When second molars are extracted and the third molar is unerupted, the third molar tends to erupt in a favourable position especially in the maxilla.16
Conclusion
This case highlights the importance of careful investigation of unusual crown morphology and its possible complications. All teeth with unusual crown morphology should be fully investigated, particularly before any other teeth are extracted for orthodontic purposes.