Smith JG, Elias LA, Yilmaz Z The psychosocial and affective burden of posttraumatic neuropathy following injuries to the trigeminal nerve. J Orofac Pain. 2013; 27:293-303 https://doi.org/10.11607/jop.1056
Renton T, Van der Cruyssen F. Diagnosis, pathophysiology, management and future issues of trigeminal surgical nerve injuries. Oral Surgery. 2019; 13:389-403 https://doi.org/10.1111/ors.12465
Renton T, Adey-Viscuso D, Meechan JG, Yilmaz Z. Trigeminal nerve injuries in relation to the local anaesthesia in mandibular injections. Br Dent J. 2010; 209 https://doi.org/10.1038/sj.bdj.2010.978
Juodzbalys G, Wang HL, Sabalys G. Injury of the inferior alveolar nerve during implant placement: a literature review. J Oral Maxillofac Res. 2011; 2 https://doi.org/10.5037/jomr.2011.2101
Pigg M, Nixdorf DR, Law AS New international classification of orofacial pain: what is in it for endodontists?. J Endod. 2021; 47:345-357 https://doi.org/10.1016/j.joen.2020.12.002
Klasser GD, Kugelmann AM, Villines D, Johnson BR. The prevalence of persistent pain after nonsurgical root canal treatment. Quintessence Int. 2011; 42:259-269
Matani JD, Kheur MG, Kheur SM, Jambhekar SS. The anatomic inter relationship of the neurovascular structures within the inferior alveolar canal: a cadaveric and histological study. J Maxillofac Oral Surg. 2014; 13:499-502 https://doi.org/10.1007/s12663-013-0563-y
Fanibunda K, Whitworth J, Steele J. The management of thermomechanically compacted gutta percha extrusion in the inferior dental canal. Br Dent J. 1998; 184:330-332 https://doi.org/10.1038/sj.bdj.4809618
Blanas N, Kienle F, Sandor GK. Injury to the inferior alveolar nerve due to thermoplastic gutta percha. J Oral Maxillofac Surg. 2002; 60:574-576 https://doi.org/10.1053/joms.2002.31858
Stojicic S, Zivkovic S, Qian W Tissue dissolution by sodium hypochlorite: effect of concentration, temperature, agitation, and surfactant. J Endod. 2010; 36:1558-1562 https://doi.org/10.1016/j.joen.2010.06.021
Giuliani M, Lajolo C, Deli G, Silveri C. Inferior alveolar nerve paresthesia caused by endodontic pathosis: a case report and review of the literature. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 2001; 92:670-674 https://doi.org/10.1067/moe.2001.117269
Renton T. Prevention of iatrogenic inferior alveolar nerve injuries in relation to dental procedures. J S African Dent Assoc. 2020;
Coulthard P, Kushnerev E, Yates JM Interventions for iatrogenic inferior alveolar and lingual nerve injury. Cochrane Database Syst Rev. 2014; https://doi.org/10.1002/14651858.CD005293.pub2
Schultze-Mosgau S, Reich RH. Assessment of inferior alveolar and lingual nerve disturbances after dentoalveolar surgery, and of recovery of sensitivity. Int J Oral Maxillofac Surg. 1993; 22:214-217 https://doi.org/10.1016/s0901-5027(05)80638-1
Burklein S, Grund C, Schafer E. Relationship between root apices and the mandibular canal: a cone-beam computed tomographic Analysis in a German population. J Endod. 2015; 41:1696-1700 https://doi.org/10.1016/j.joen.2015.06.016
Denio D, Torabinejad M, Bakland LK. Anatomical relationship of the mandibular canal to its surrounding structures in mature mandibles. J Endod. 1992; 18:161-165 https://doi.org/10.1016/S0099-2399(06)81411-1
Shah NP, Murtadha L, Brown J. Bifurcation of the inferior dental nerve canal: an anatomical study. Br J Oral Maxillofac Surg. 2018; 56:267-271 https://doi.org/10.1016/j.bjoms.2018.01.016
Rood JP, Shehab BA. The radiological prediction of inferior alveolar nerve injury during third molar surgery. Br J Oral Maxillofac Surg. 1990; 28:20-25 https://doi.org/10.1016/0266-4356(90)90005-6
Gutierrez JH, Brizuela C, Villota E. Human teeth with periapical pathosis after overinstrumentation and overfilling of the root canals: a scanning electron microscopic study. Int Endod J. 1999; 32:40-48 https://doi.org/10.1046/j.1365-2591.1999.00185.x
Vieyra JP, Acosta J, Mondaca JM. Comparison of working length determination with radiographs and two electronic apex locators. Int Endod J. 2010; 43:16-20 https://doi.org/10.1111/j.1365-2591.2009.01620.x
Perotti S, Bin P, Cecchi R. Hypochlorite accident during wndodontic therapy with nerve damage - A case report. Acta Biomed. 2018; 89:104-108 https://doi.org/10.23750/abm.v89i1.6067
Ahlgren FK, Johannessen AC, Hellem S. Displaced calcium hydroxide paste causing inferior alveolar nerve paraesthesia: report of a case. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 2003; 96:734-737 https://doi.org/10.1016/j.tripleo.2003.08.018
Byun SH, Kim SS, Chung HJ Surgical management of damaged inferior alveolar nerve caused by endodontic overfilling of calcium hydroxide paste. Int Endod J. 2016; 49:1020-1029 https://doi.org/10.1111/iej.12560
Poveda R, Bagan JV, Fernandez JM, Sanchis JM. Mental nerve paresthesia associated with endodontic paste within the mandibular canal: report of a case. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 2006; 102:e46-49 https://doi.org/10.1016/j.tripleo.2006.03.022
Orstavik D, Kerekes K, Eriksen HM. The periapical index: a scoring system for radiographic assessment of apical periodontitis. Endod Dent Traumatol. 1986; 2:20-34 https://doi.org/10.1111/j.1600-9657.1986.tb00119.x
Levander E, Bajka R, Malmgren O. Early radiographic diagnosis of apical root resorption during orthodontic treatment: a study of maxillary incisors. Eur J Orthod. 1998; 20:57-63 https://doi.org/10.1093/ejo/20.1.57
Assessing inferior dental nerve injury risk in orthograde root canal treatment Paul Cruci Allen Gaon St John Crean Jackie Brown John Rout Dental Update 2024 50:4, 707-709.
Clinical Lecturer in Endodontics, Barts and The London School of Medicine and Dentistry, Queen Mary University of London, Specialist in Endodontics, Gerrards Cross, Buckinghamshire
Clinical Lecturer in Endodontics, Barts and The London School of Medicine and Dentistry, Queen Mary University of London, Specialist in Endodontics, Edgware, Middlesex
Pro Vice Chancellor (Research, Innovation and Enterprise), Professor of Medicine in Dentistry, Consultant Oral and Maxillofacial Surgeon, University of Central Lancashire
Nerve injury associated with root canal treatment is relatively rare, but can lead to significant morbidity. The role of 2D and 3D radiography in case assessment is explored and a new three-tier grading system is proposed to aid in risk assessment and clinical decision-making. This grading system would assist dentists to fully appraise patients, gain appropriate informed consent and guide treatment of endodontic cases where there is an increased risk of nerve injury.
CPD/Clinical Relevance: A new three-tier grading system to assist in the pre-operative assessment and risk management of endodontic cases where there is an increased risk of nerve injury is proposed.
Article
Nerve injury is a relatively uncommon, but nonetheless serious, side effect of root canal treatment of mandibular posterior teeth.1,2 It can result in permanently altered sensation, which can have serious effects on a patient's quality of life, both functionally and psychologically.3 It is largely avoidable with correct pre-operative assessment and treatment protocols.
The diagnostic criteria and management protocols for post-traumatic neuropathy lie outside the scope of this article. Readers must familiarize themselves with established and published protocols to guide early post-treatment intervention to optimise treatment and nerve injury resolution.4 Advice on urgent recognition, diagnosis, referral and management of endodontic-related nerve injury, with or without pain, can be found at: trigeminalnerve.org.uk
Inferior dental nerve (IDN) and mental nerve (MN) injuries are most commonly (but not exclusively) reported in relation to mandibular second molars and premolars. An understandable desire to retain teeth, coupled with complex restorative histories, increasingly presents practitioners with challenging endodontic cases that may involve greater risk of nerve damage.
Incidence of mandibular post-endodontic nerve injuries
The literature contains significant references to persistent altered inferior dental nerve sensation resulting from the administration of local anaesthesia, particularly by IDN block techniques.5,6 While the authors recognize this as an important cause of nerve injury, this subject lies outwith the scope of this article, which focuses on radiographic assessment criteria.
Classification of nerve injury was first described by Seddon and Sunderland.7 The least severe injury in which nerve integrity is retained, but where signalling ability is temporarily impaired, is termed neurapraxia. Partial damage to the axon, which may recover in 2–12 months, is termed axonotmesis. Extensive damage to the full axon thickness and associated connective tissue is termed neurotmesis.
The clinical effect of these lesions may be categorized as paraesthesia, which is a sensory disturbance resulting in, for example, sensations such as burning, tingling or partial numbness. Hypo-aesthesia refers to a state of reduced sensitivity to stimulation, and hypo-algesia to a decreased response to a stimulus that is normally painful. Hyperaesthesia describes a sensation of heightened sensitivity to stimulation and hyperalgesia to an increased response to a stimulus that is normally painful. Allodynia refers to pain elicited by a stimulus that does not normally provoke pain, and anaesthesia refers to complete insensitivity to stimulation. These states tend to be dynamic, frequently changing over time, following the nerve injury.8
Referring to the International Classification of Orofacial Pain (ICOP), root canal treatment may give rise to post-traumatic trigeminal neuropathic pain (ICOP Code 4.1.2.3) occurring after accidental trauma or surgical injury of the peripheral nerve branches, the IDN or MN. Therefore, careful post-treatment evaluation of a patient presenting with local somatosensory symptoms or signs, whether negative (hypo-aesthesia and/or hypo-algesia) or positive (hyperalgesia and/or allodynia) must be undertaken. It is essential for correct and timely management to differentiate between a dental, periodontal or a neuropathic aetiology.9
Most reports of post-endodontic nerve injuries are case studies. Knowles et al investigated paraesthesia related to root canal treatment of 832 mandibular premolars, reporting an incidence of 0.96%.10 Klasser et al found a 7% incidence of chronic neuropathic pain among 2338 patients who underwent a single root canal treatment procedure.11
Pogrel reported on a series of 61 patients over a 7-year period with endodontic sealer extruded into the inferior dental canal (IDC).1 Six of the cases exhibited radiological evidence of sealer in the IDC, but were asymptomatic. The author hypothesized that the lack of symptoms may have been due to relatively low neurotoxicity of the sealer and/or lack of penetration of the epineurium. In 42 cases, there was evidence of sealer or obturation material in the IDC, but either symptoms were mild or too great a time delay was judged to have elapsed for surgical treatment to be likely to succeed. Fewer than 10% of these cases experienced resolution of symptoms.
Potential causes of nerve injury related to endodontic intervention (Table 1)
Direct trauma
This may result from over-instrumentation with hand or rotary instruments, poor placement of irrigating needles or overextension or extrusion of intermediate dressings or obturation materials, including single gutta percha (GP) cones, thermoplasticized GP and root canal sealers. Pressure ischaemia can arise from haemorrhage into the IDC following extra-canal instrumentation and laceration of the inferior dental artery or vein, which is located superiorly to the IDN within the IDC.12
Table 1. Risk factors relating to potential for nerve injury in orthograde root canal treatment.
Anatomical
Proximity of IDC or MF to apex of treatment tooth
Integrity of cortical outline of IDC
Root shape and apical curvature (eg towards or away from IDC)
Internal and external resorptive lesions, lateral canals and fenestrations
Previous iatrogenic effects (eg transportation or perforation)
Sclerotic canals
Pathological
Presence of peri-apical pathology, size of area of apical bone destruction (odontogenic/non-odontogenic) (eg granuloma, cyst or neoplasia)
Quality of bony margins of apical lesion (poorly defined/well defined/corticated)
Distance between edge of apical lesion and IDC/MC/MF
Root resorption (internal and external)
Inflammatory changes to shape and size of apical foramen(ae)
Infective and inflammatory mediators impacting on the IAN/MN
Procedural
Instrumentation
Direct mechanical trauma (eg instrumentation, inoculation/laceration injury or forced obturation of material through root apex impacting on IDC and IDN directly)
Chemical trauma
Irrigants: forced extrusion or uncontrolled diffusion of, for example sodium hypochlorite, EDTA, chlorhexidine, citric acid, hypochlorous acid, alcohol
Intermediate medicaments or dressings, solvents, sealants, root filling materials
Local anaesthetic solutions, particularly via intrapulpal route
Thermal trauma
Warm vertical compaction (continuous and interrupted wave)
Over-instrumentation is best avoided by careful pre-operative assessment, including radiographic length estimation using 2D or 3D modalities, as required. The routine use of an electronic apex locator should be considered obligatory for any orthograde root canal treatment, and together with development of a well-designed apical capture zone, will help to control the displacement of obturation materials into the peri-apical tissues.
Where obturation materials are heated prior to vertical condensation, extrusion of the thermoplasticized material in proximity of the IDN can lead to thermal injury.13,14
Chemical trauma
Extra-radicular extrusion of sodium hypochlorite (NaOCl) solution can result in severe damage to neural tissue because of its high pH and action in breaking down fatty and amino acids. The trend towards using more concentrated NaOCl solutions as endodontic irrigants may potentiate this effect. The speed of dissolution of pulp fragments was found to be directly proportional to the NaOCl solution concentration.15
Neurapraxia of infective origin
Peri-apical lesions near the IDN can cause pressure injuries because of local oedema. In established peri-apical disease, mechanical pressure from the inflammatory process can exert a compressive force on both MN and the IDN.
Associated inflammatory mediators such as interleukin-1, tumour necrosis factor and nitric oxide have neurotoxic potential owing to their low pH. Bacteria and their by-products may also produce chemically mediated neural effects.16,17
In recognizing the challenge of determining aetiology, arriving at an accurate diagnosis and managing trigeminal nerve injuries, Renton has suggested a useful pathway for supportive management of such injuries.18,19 Little is known about the potential for recovery, especially in the case of longer-standing lesions. Schultze-Mosgau et al suggest that the potential for sensory recovery after several months is low.20
It is important that the practitioner recognizes the existence of neuropathy in relation to a peri-apical lesion or acute infection. Part of the patient history in assessment of a mandibular posterior tooth should therefore include enquiry as to any sensory changes in the distribution of the IDN.
In cases where neuropathy has been reported, immediate measures should be undertaken to decompress the lesion, manage the infection at the earliest opportunity and monitor sensory changes with early specialist referral as necessary.
The potential for development of acute infection, especially following the initial stages of root canal treatment, means that consent documents should recognize and include reference to the possibility of sensory alteration or loss as a result of treatment.
Anatomical proximity of the IDC relative to root apices
Bürklein et al examined 626 cone-beam computed tomography (CBCT) scans of male and female subjects to investigate the shortest distance between the IDC and the root apices of second premolars, first, second and third molars. A total of 1974 teeth were included. Mean distances were 4.2, 4.9, 3.1 and 2.6 mm, respectively. These distances were significantly shorter in women than men.21 Importantly, the study also identified a direct relationship between root apices and the IDC in 3.2%, 2.9%, 15.2% and 31.3% of teeth, respectively. These communications were seen almost twice as frequently in women as in men.
Denio et al studied the spatial relationship of the mandibular canal to the posterior teeth in 22 mature dried mandibles. Second premolars and second molars had the closest mean distances to the canal (4.7 and 3.7 mm, respectively). The apices of the mesial roots of the first molars were found to have a mean distance of 6.9 mm.
The canal pathway in mature mandibles followed in S-shaped curve in 31% of the cases, with the canal being located buccally to the distal root of the second molar, crossing lingually below the second molar mesial root to lingual aspect of the first molar and then crossing back buccally to below the second premolar apices. In 19% of cases, the canal pathway was located lingually to the apices of the posterior teeth, with it appearing 17% buccally and 5% directly inferiorly. In 28% of the cases, the canal could not be identified clearly in the second premolar and first molar regions, appearing more as a coalescence of trabecular bone. Hence, based on these findings, the mandibular second premolar and second molar are the most likely teeth to be involved in accidental damage to the mandibular canal during root canal therapy.22
In addition, significantly shorter distances from the IDC to root apices were seen in patients aged under 35 years compared with older patients. Thus, caution is warranted when planning root canal treatment of mandibular second and third molars in younger female patients as the tooth root apices are frequently not only closer to the canal, but also more often directly communicating with it.
Bifurcation of the IDC
In a CBCT study of 281 patients, Shah et al identified a 38% incidence of IDC bifurcation. Some patients had multiple bifurcations.23 Bifurcation was most commonly found posterior to the third molar or within 2 mm of the third molar roots. The study also found that the sensitivity of panoramic radiography in detecting canal bifurcation was poor. Most bifurcations ran in a superior direction in the same plane as the main canal, with smaller proportions running in superobuccal and superolingual directions. Therefore, in advance of undertaking an endodontic procedure with the potential for IDN damage, it is critical to determine the true location of the IDC in respect to the peri-apical anatomy of the treatment tooth.
Traditionally, dentists relied on 2D interpretation drawn from intra-oral peri-apical radiographs taken, at best, with a paralleling technique. This methodology provided some general comfort if the classical IDC ‘tramlines’ or, more accurately, the corticated canal borders, were evidenced to be distant from tooth apices. However, the process is technique sensitive and relies on correct positioning of the intra-oral film or sensor relative to the target area and X-ray tube. Often, this is not achieved, and leads to image angular foreshortening or elongation. Additionally, superimposition of local bony anatomy, for example, the external oblique ridge can often lead to further misrepresentation. Inability to clearly visualize the IDC in the field of view does not exclude it from risk of damage.
Traditionally, when considering pre-operative radiographs, usually panoramic imaging, for the extraction of mandibular wisdom teeth, a series of classic radiographic appearances was used to assess proximity of a tooth to the IDC:24
Change of density (radiolucency) of the root;
Loss of lamina dura around the root where it is crossed by the canal;
Constriction or narrowing of the root;
Curvature or hooking of the root where it abuts up against the roof of the canal;
Change in direction of the canal as it crosses the root;
Loss of one or both of the cortical outlines (tramlines) of the canal;
Constriction or narrowing of the canal.
Transferring this to root canal treatment management may help to provide useful guidance in determining the proximity, and hence risk of potential damage, to the IDN.
2D imaging is always the first-line approach when determining risk, but any doubt arising should warn the operator to consider the follow-up use of 3D imaging to determine the precise spatial relationship of the peri-apex and the topography of the IDC in cases deemed high-risk.
A small volume, high definition CBCT scan will reveal the spatial relationship between teeth and vital structures. It will also help to provide information regarding root canal morphology and any aberrations (including unexplored and lateral canals, calcifications, previous treatments, perforations, or canal transportation) and importantly the visualization of the degree of apical root resorption. This may well be visually challenging or missed entirely on a 2D image. Importantly, the integrity of the lingual cortical plate and its relative proximity to molar apices will also be shown.
Instrumentation and procedural considerations
Preparation and length control in the apical third of the root canal is vital in limiting the potential for neural and vascular laceration, displacement of infected canal debris or extrusion of intermediate dressings or obturation materials. This is particularly important in the management of apical resorption cases which present with irregularly shaped and widened apical foramina.
It is important to visualize that the tooth roots and IDC exist within a milieu of cancellous bone of various density and adjacent to a corticated neurovascular channel of varying integrity. The shape and structure of the bony trabeculae and medullary spaces or vacuoles can easily allow tracking of hydraulically extruded materials well beyond the physiological terminus of the root. A sparse trabecular pattern is common in the posterior mandible and may increase the risk of an iatrogenic hydraulically induced extrusion reaching the IAC. When in doubt, CBCT analysis is particularly useful in enabling practitioners to determine the bony topography. A list of potential causes for reduced alveolar bone density has been listed in Table 2.
Table 2. Potential causes for reduced alveolar bone density. Italic: commonly encountered in practice.
Idiopathic and natural anatomical variation
Osteoporosis
Osteopenia
Hypophosphatasia
Postmenopausal women
Hypophosphataemia
Hyperparathyroidism
Papillon–Lefèvre syndrome
Histiocytosis X
Agranulocytosis
Leukocyte adherence deficiency
Neutropenia
Leukaemia
Diabetes mellitus
Scleroderma
Fibrous dysplasia (only in very early stages)
Acrodynia
Down syndrome
Chédiak–Higashi syndrome
Thalassemia
Sickle cell disease
Over-preparation of the canal can also lead to disruption of the natural architecture of the root canal terminus, which can increase the likelihood of diffusion of irrigation solutions, intermediate dressings, and medicaments into the peri-apical area. Without a well-constructed apical capture zone, the final obturation material may extrude into the peri-apical region leading to a potential chemical- and mechanical-induced neuropathy.16,25
Clearly, when embarking on root canal treatment it is essential to determine as accurately as possible where the root canal terminates and where the peri-apical tissues start in order to minimize the inoculation of potentially infected debris in or around the IAC. The apical terminus can be reliably determined by using a calibrated EAL.26
The reliance solely on a radiographic working length has been shown to be inaccurate and can lead to over preparation in many cases.27 Therefore, an accurate, reproducible, and ‘live’ linear feedback regarding instrument tip position is essential when approaching the canal terminus to ensure precision in preparation.
Irrigation
Sodium hypochlorite (NaOCl) is still considered the gold standard irrigant in endodontics because of its ability to disinfect and dissolve necrotic and infected material in the root canal. Therefore, sacrificing the effectiveness of root canal cleaning by using less efficacious irrigants would seem ill advised if there is a risk of persistent infection.
Great care must be taken to ensure that any irrigant always remains within the canal and does not extrude under pressure as this may cause local tissue necrosis due to its caustic nature.28 The use of negative pressure irrigation systems may be indicated in these high-risk cases.
Intermediate dressings
The uncontrolled placement of intermediate dressings can lead to extrusion and morbidity if contact with neural tissue occurs. As discussed, extrusion of material can have both chemical and compressive effects on the peri-apical tissues which in turn can lead to temporary or permanent changes in adjacent neural tissue. The ideal pH of an endodontic medicament or sealer should approximate to that of body fluids (approx. pH 7.3) otherwise there is a risk of neural toxicity caused by the chemical insult in the event of extrusion. Calcium hydroxide is a commonly used an intermediate dressing has a pH of 10–14. A large extrusion of calcium hydroxide-based sealer in the peri-apical tissues was found not only to have a chemical effect, but also a mechano-compressive effect on the IDN leading to paraesthesia.29,30
Obturation
Obturation materials including sealers should be confined to the root canal and various tributaries and should not extend to the peri-apical tissues or neighbouring structures.31,32 Gutta-percha (GP) is the most commonly used obturation material. GP has low relative cytotoxicity, however in the presence of tissue fluids leaching of potentially harmful constituent parts (eg zinc oxide) could contribute to its longer-term toxicity.33 When heated material is extruded in the vicinity of neural tissue it may induce thermal, chemical and/or mechanical trauma. Clearly, the potential for any contact with neural tissue must be recognized and addressed at the earliest opportunity.13,34
Although minor extrusions, traditionally known as ‘sealer puffs’, are generally well tolerated, in high-risk areas they must be anticipated and minimized by appropriate apical capture zone design and well-controlled obturation techniques.
Introduction to the pre-operative risk assessment classification
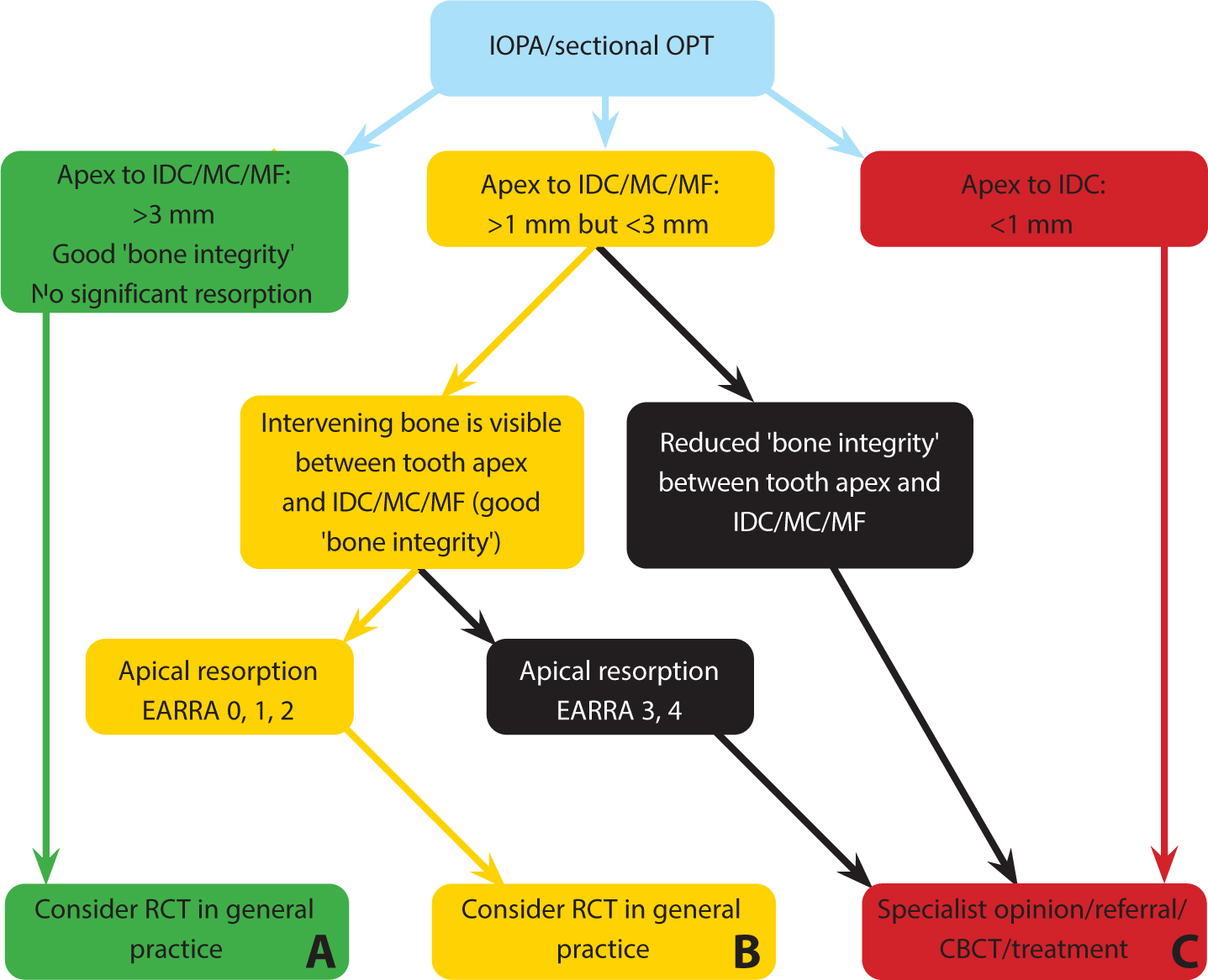
This assessment algorithm is based on three radiographically assessed parameters (Table 3, Figure 1):
Table 3. The tier structure: pre-endodontic assessment tool for lower premolars and lower molars.
Tier A
1
Closest apex of the treatment tooth is > 3mm from the Superior border of IDC/MCMF
If Yes, go to 2
If No, go to 5
2
Bone is visible between treatment tooth apex and IDC/MC/MF. Bone integrity: good
If Yes, go to 3
If No, go to 10
3
External apical root resorption assessment
If EARRA 0,1,2, go to 4
If EARRA 3, 4 Go to 10
4
Consider treating in general practice (A)
Tier B
5
Closest apex of the treatment tooth is >1 mm <3 mm from the superior border of IDC/MC/MF
If Yes, go to 6
If No, go to 9
6
Bone is visible between treatment tooth apex and IDC/MC/MF. Bone integrity: good
If Yes, go to 7
If No, go to 10, (B+)
7
External apical root resorption assessment
If EARRA 0,1,2, go to 8
If EARRA 3, 4 Go to 10, (B+)
8
Consider treating in general practice (B)
Tier C
9
Closest apex of the treatment tooth is <1 mm from superior border of IDC/MC/MF
If Yes, go to 10
10
Consider specialist referral for assessment, CBCT investigation and treatment (C)
Figure 1. Flow diagram assessment tool for the pre-endodontic radiographic assessment of mandibular premolars and molars. Assessment is based on a good-quality paralleling technique peri-apical. If this fails to show the ID canal, consider performing peri-apical radiography after local analgesia and placing the film vertically into the lingual sulcus as far down as possible, or consider a sectional panoramic radiograph of the lower quadrant in question.
Distance of treatment tooth apex to IDC (or MC and MF);
Presence of intervening bone and assessment of ‘bone integrity’;
Extent of any apical resorption.
‘Bone Integrity’ is a term coined to reflect the intervening alveolar bone density, which could be ‘good’ (ie normal density as assessed for the patient's age), ‘reduced’ (eg osteoporotic) or even ‘increased’ (sclerotic, eg a localized sclerotic osteitis, or a chronic sclerosing osteomyelitis). If ‘reduced’, this may reflect the presence of odontogenic infection or other diseases (Table 2). Any patient declaring a medical history that may affect bone density should raise concerns over resistance to extruded material.
The evaluation of the status of peri-apical tissues in endodontics is traditionally assessed according to the Peri-apical Index (PAI) developed by Ørstavik.35 However, the External Apical Root Resorption Assessment scale by Levander and Malmgren provided a more focused assessment of the degree of radiographically visualized root resorption and would reflect the architectural changes at the root terminus specifically, and therefore the potential risk for iatrogenic damage (Table 4).36
EARR from 2 mm to one-third of the original root length
4
EARR exceeding one-third of original root
El Ayouti et al suggested that in premolars and molars a radiographically determined working length ending 0–2 mm short of the radiographic apex presented a higher risk for unintentional over instrumentation.37
Therefore, an EARRA score of >2 mm is taken to suggest that the apical constriction and may have been compromised, leading to reduced apical resistance form and thereby increasing the risk of an extrusion.
A practitioner's clinical experience will influence their ability to undertake a particular case. Where there is an increased risk of morbidity, or the operator is in doubt, a specialist opinion should be always be sought.
The management of a post endodontic treatment nerve injury can be distressing, onerous and challenging for both the patient and operator. Therefore, careful planning and preparation with judicious execution of the treatment will help to mitigate many of the potential pitfalls as described above and reduce the risk of postoperative morbidity. The radiation dose received by the patient must always be kept as low as reasonably practicable (ALARP), while still achieving a satisfactory clinical diagnosis.
A question may arise regarding the threshold chosen to expose a patient to a CBCT scan. It is the belief of the authors that in Tier B+ and Tier C cases the extra information provided by 3D imaging can provide valuable clinical information over and above that of a 2D modality (Table 5).
Table 5. Suggested CBCT prescription and reporting criteria.
Request
Small field of view (FOV), high definition CBCT of the treatment tooth (endodontic quality)
It is important to ensure that the entire CBCT volume is reported on by a suitably qualified person. Ideally, a specialist dental and maxillofacial radiologist
Areas to consider for reporting
IDC/MC pathway and MF position and anatomical variants (eg bifidity, anterior loop)
Spatial position and proximity of IAC/MC/MF to the apices of treatment tooth
Identify any IDC bifurcations
Quality/integrity of bony cortication of the IDC/MC/MF in the vicinity of the treatment tooth
Relative density of the local trabecular pattern and ratio of intertrabecular spaces, presence of sclerosis
Peri-apical/root resorptive pattern
Root canal anatomy, including lateral canal anatomy
Proximity of the roots to the lingual plate and mylohyoid attachment and effects of inflammatory disease on adjacent cortical plates (determination of submandibular space infection risk)
A further detailed assessment of the remaining volume must be undertaken to report on adjacent teeth and structures, incidental findings and pathologies
Ultimately, the authors want to provide the GDP with a simple to use tool to assess risk and plan the treatment of endodontic cases where there is risk of increased neural injury and provided a coherent referral pathway for more challenging cases (Figure 1).
In higher-risk Tier A and B+ cases, the recommendation is to follow a Tier C pathway and liaise with a specialist endodontist for assessment, CBCT imaging and possible treatment.
As stated in the GDC ‘Standards for the Dental Team’, dentists should work within their professional competence and only carry out a treatment for which they are appropriately trained.38
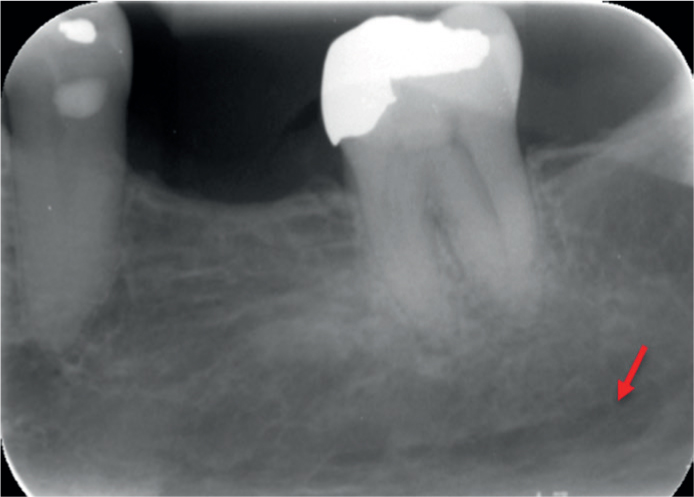
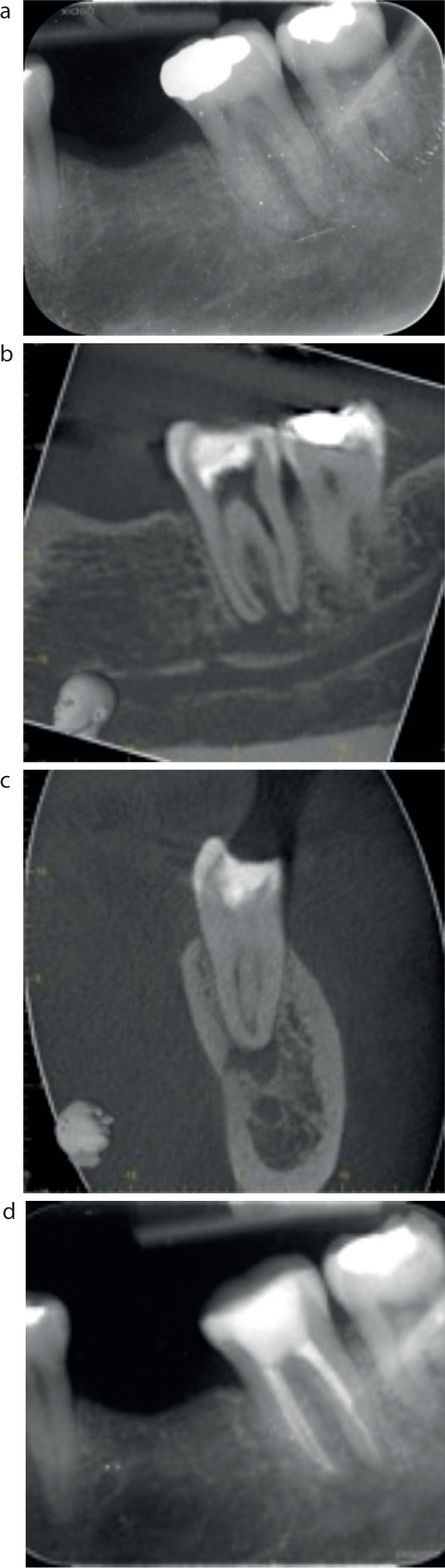
Figure 5. (a–d) The intervening bone is clearly visible between the treatment tooth apex and IDC, but there is a reduction of bone density associated with the distal root, making this case a Tier B+.
Closest apex of the treatment tooth is >1 mm and <3 mm from superior border of IDC
Bone is visible between treatment tooth apex and IDC
Bone integrity: reduced
EARRA: 0–2
Tier B+ upgraded to Tier C pathway: consider referral for specialist opinion, scan and treatment.
Tier B+ cases are recommended to be placed on a Tier C pathway because there is an increased risk of neural injury. These patients are recommended to have a specialist review and CBCT investigation. In this case, a CBCT scan revealed a superior accessory branch of the IDC below the distal root of LL6. This higher-risk B+ case was completed in specialist practice.
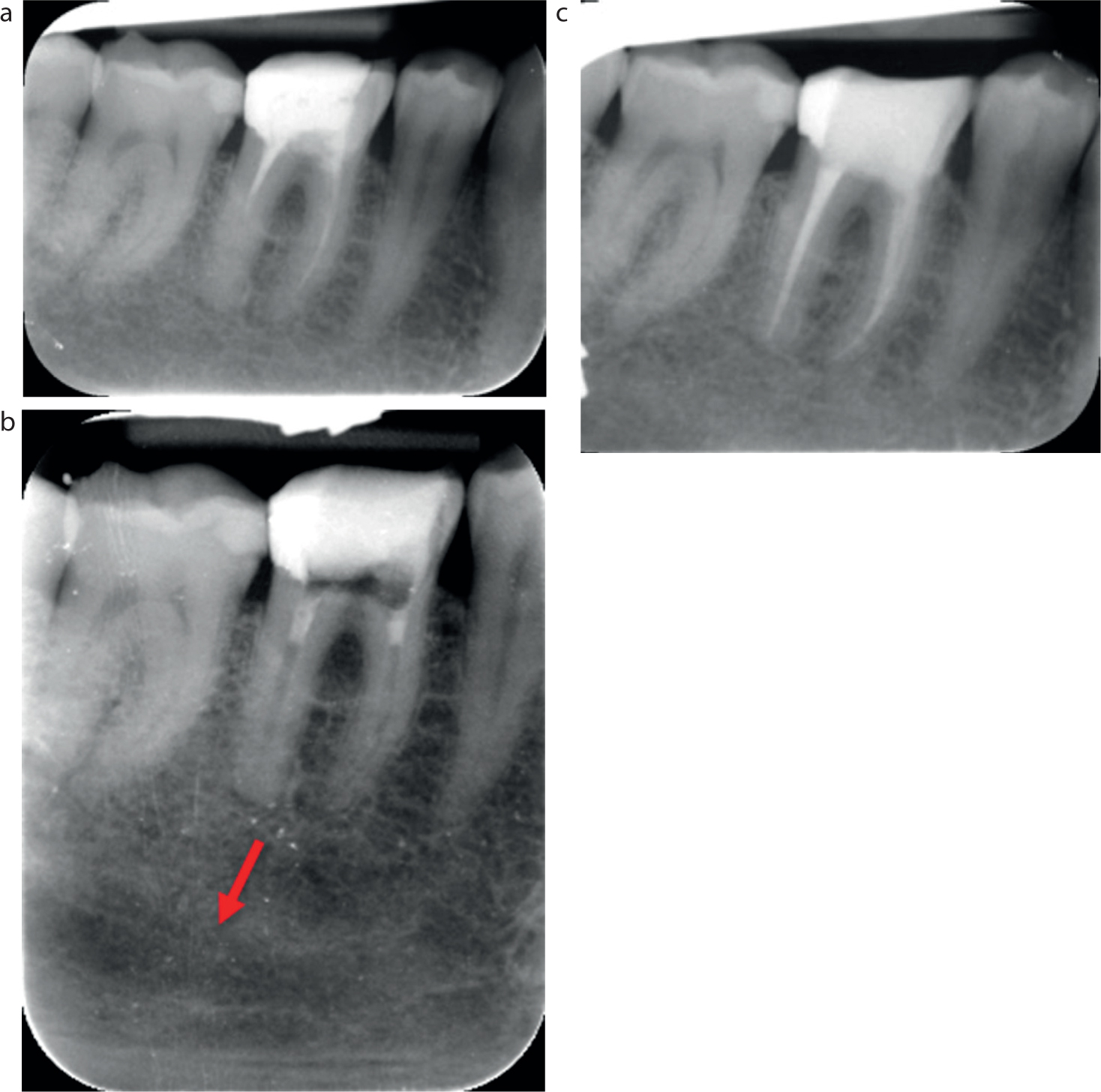
Figure 6. (a–d) The upper border of the IDC and the peri-apical lucency is highlighted. Note the lack of intervening bone in relation to the mesial root apex and the IDC. Intervening bone is visible between treatment tooth apex and IDC, but there is a peri-apical lucency and reduced bone density associated with the mesial root apex, making this case a Tier B+.
Closest apex of the treatment tooth is >1 mm and <3 mm from superior border of IDC
Bone is visible between treatment tooth apex and IDC
Bone integrity: reduced
EARRA: 0–2
Tier B+ upgraded to Tier C pathway: consider referral for specialist opinion, scan and treatment.
Tier B+ cases are recommended to be placed on a Tier C pathway as there is increased risk of neural injury. These patients are recommended to have a specialist review and CBCT investigation. In this case, a CBCT scan revealed significantly reduced density of intervening bone in relation to the treatment root apex and the IDC. This would have offered little resistance to any possible extrusion. This higher-risk Tier B+ case was completed in specialist practice.
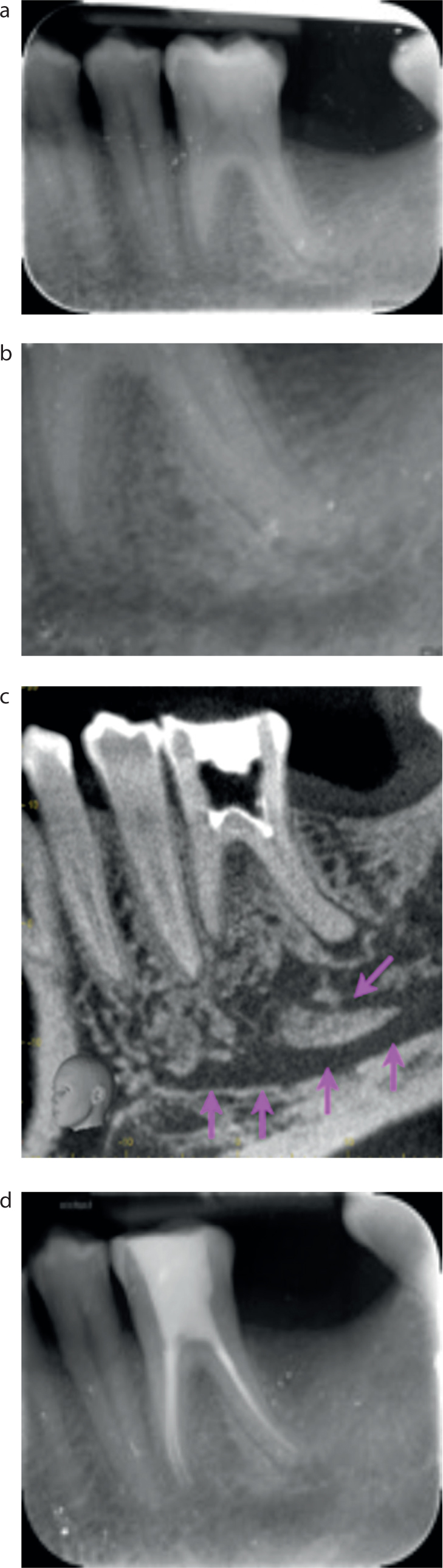
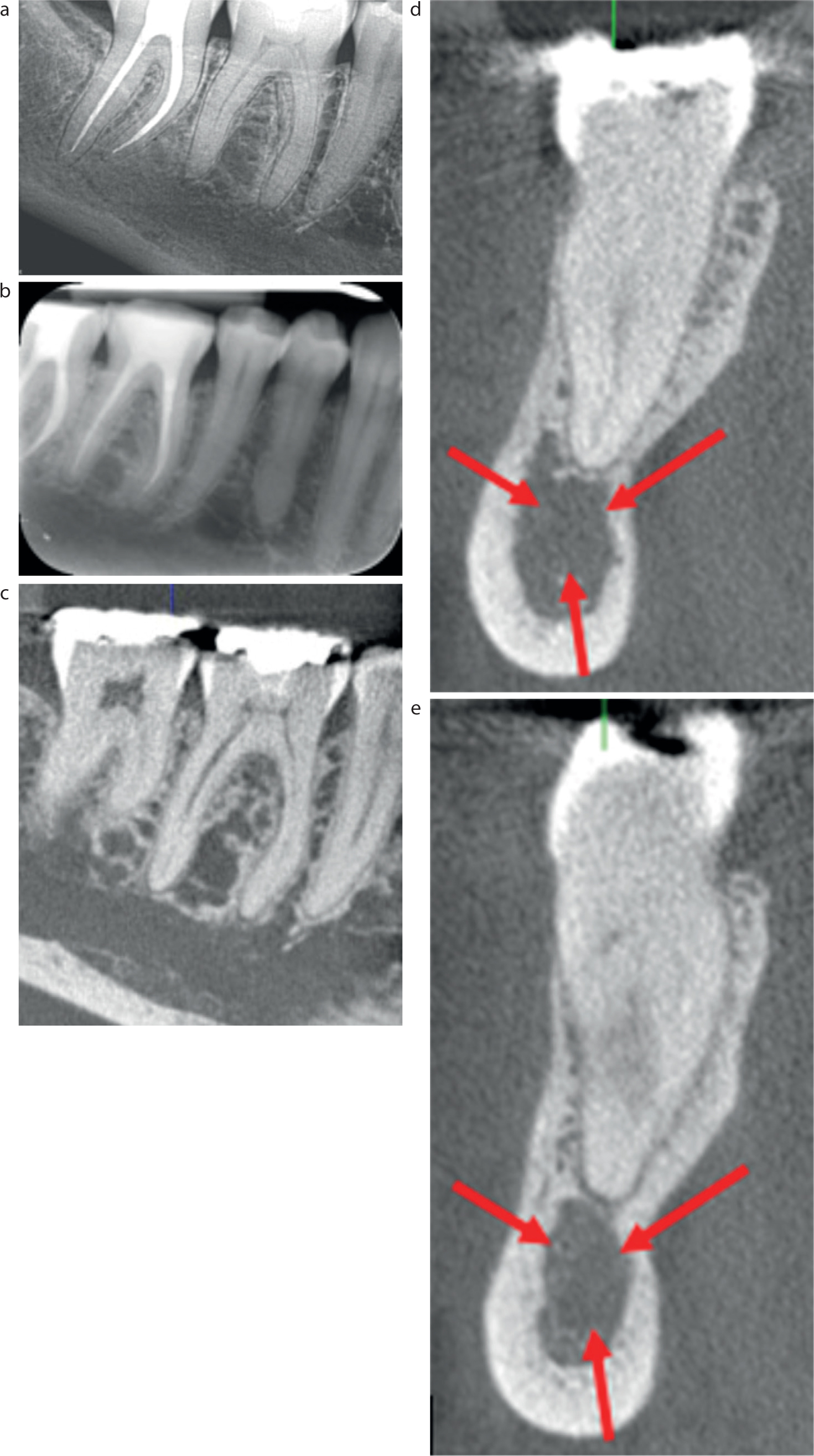
Figure 7. (a–e) No IDC could be determined from the IOPA despite the full depth of the mandible having been imaged.
Diagnosis: Pulpal: SIP; Apical: normal
Closest apex of the treatment tooth is <1mm from the superior border of IDC
Tier C: referral for specialist opinion, scan and treatment.
The recommendation in this high-risk Tier C case was to liaise with a specialist endodontist for assessment and CBCT imaging. Questioning of the patient identified a recent CBCT scan undertaken for treatment of LL7. This was made available, which revealed significantly reduced bone density and very poor IDC cortication in this osteopenic patient. Sharing the scan obviated the need for a further imaging in this case and reduced the patient's risk to further radiographic exposure. This higher-risk Tier C case was completed in specialist practice.
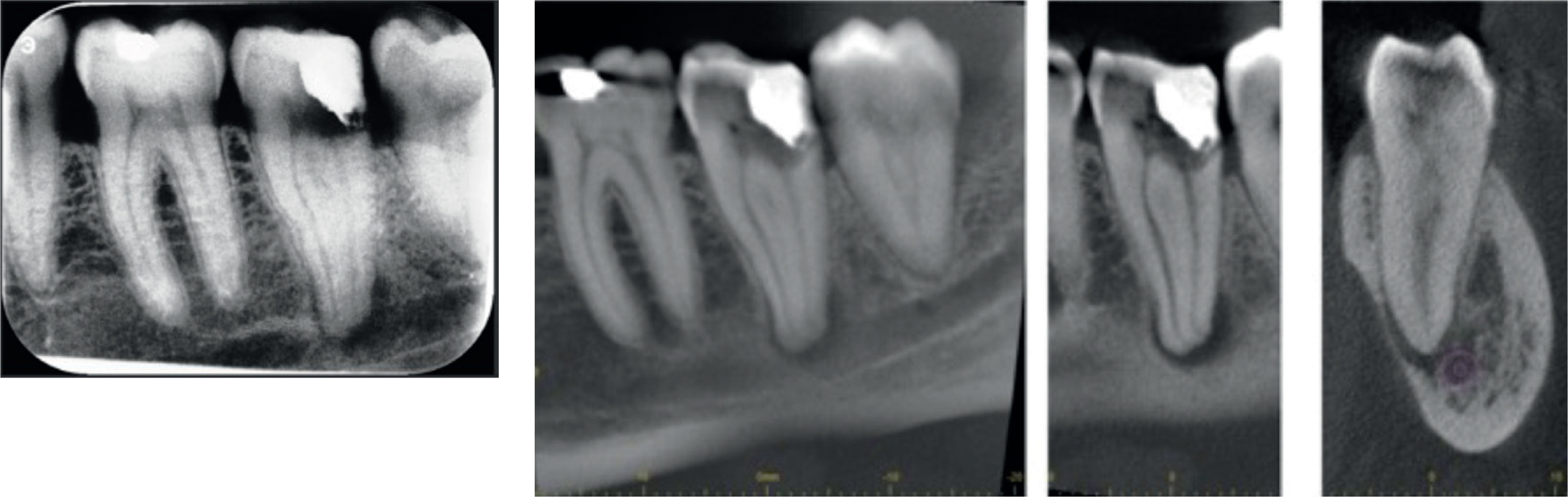
Figure 8. Note the intimate proximity of the apical foramen and the IDC.
Diagnosis: Pulpal: necrotic; Apical: SAP
Closest apex of the treatment tooth is <1mm from superior border of IDC
Tier C: referral for specialist opinion, scan and treatment.
The recommendation in this high-risk Tier C case was to liaise with a specialist endodontist for assessment, including CBCT scanning. Once the risk of a potential neural injury and challenging restorative considerations were outlined to the patient, he elected to have this tooth removed. This was performed by a specialist oral surgeon. Of note was the length of the roots of LL7 and their proximity to the thin lingual plate. Untreated, this could have increased the risk of a submandibular space infection.
Conclusion
The potential for neural injury is ever present when undertaking mandibular molar and premolar endodontic treatment. It is hoped that this new three-tier grading system will provide a useful guide for colleagues to more accurately carry out a pre-operative risk assessment and help mitigate the chances of a potentially life-changing injury occurring.