Patel N, Gemmel A, Bonsor S, Edwards D. Re-endodontic treatment. Part 1: why and when?. Dent Update. 2022; 50:652-658
Dawood A, Patel S. The Dental Practicality Index – assessing the restorability of teeth. Br Dent J. 2017; 222:755-758 https://doi.org/10.1038/sj.bdj.2017.447
Tifooni A, Al-Nuaimi N, Dawood A Validation of the effectiveness of the Dental Practicality Index in predicting the outcome of root canal retreatments. Int Endod J. 2019; 52:1403-1409 https://doi.org/10.1111/iej.13142
Abbott PV. Assessing restored teeth with pulp and periapical diseases for the presence of cracks, caries and marginal breakdown. Aust Dent J. 2004; 49:33-39 https://doi.org/10.1111/j.1834-7819.2004.tb00047.x
Magne P, Spreafico RC. Deep margin elevation: a paradigm shift. Am J Esthet Dent. 2012; 2:86-96
Ng YL, Mann V, Gulabivala K. A prospective study of the factors affecting outcomes of nonsurgical root canal treatment: part 1: periapical health. Int Endod J. 2011; 44:583-609 https://doi.org/10.1111/j.1365-2591.2011.01872.x
Gutierrez JH, Aguayo P. Apical foraminal openings in human teeth. Number and location. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 1995; 79:769-777 https://doi.org/10.1016/s1079-2104(05)80315-4
Patel N, Edwards D. When to consider the use of CBCT in endodontics. Dent Update. 2021; 48:932-941
Krell KV, Caplan DJ. 12-month success of cracked teeth treated with orthograde root canal treatment. J Endod. 2018; 44:543-548 https://doi.org/10.1016/j.joen.2017.12.025
Edwards D, Bailey O, Stone SJ, Duncan H. How is carious pulp exposure and symptomatic irreversible pulpitis managed in UK primary dental care?. Int Endod J. 2021; 54:2256-2275 https://doi.org/10.1111/iej.13628
Patel S, Brown J, Semper M European Society of Endodontology position statement: use of cone beam computed tomography in endodontics: European Society of Endodontology (ESE) developed by. Int Endod J. 2019; 52:1675-1678 https://doi.org/10.1111/iej.13187
Plotino G, Grande NM, Isufi A Fracture strength of endodontically treated teeth with different access cavity designs. J Endod. 2017; 43:995-1000 https://doi.org/10.1016/j.joen.2017.01.022
Sundqvist G, Figdor D, Persson S, Sjögren U. Microbiologic analysis of teeth with failed endodontic treatment and the outcome of conservative re-treatment. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 1998; 85:86-93 https://doi.org/10.1016/s1079-2104(98)90404-8
Sjögren U, Figdor D, Persson S, Sundqvist G. Influence of infection at the time of root filling on the outcome of endodontic treatment of teeth with apical periodontitis. Int Endod J. 1997; 30:297-306 https://doi.org/10.1046/j.1365-2591.1997.00092.x
Gulabivala K, Patel B, Evans G, Ng YL. Effects of mechanical and chemical procedures on root canal surfaces. Endod Topics. 2005; 10:103-122
Byström A, Sundqvist G. Bacteriologic evaluation of the efficacy of mechanical root canal instrumentation in endodontic therapy. Scand J Dent Res. 1981; 89:321-328 https://doi.org/10.1111/j.1600-0722.1981.tb01689.x
Bonsor SJ. Disinfection of the root canal system: what should the protocol be?. Dent Update. 2021; 48:836-844
Stojicic S, Zivkovic S, Qian W Tissue dissolution by sodium hypochlorite: effect of concentration, temperature, agitation, and surfactant. J Endod. 2010; 36:1558-1562 https://doi.org/10.1016/j.joen.2010.06.021
Metzger ZV, Solomonov M, Kfir A. The role of mechanical instrumentation in the cleaning of root canals. Endod Topics. 2013; 29:87-109
Al-Jadaa A, Paqué F, Attin T, Zehnder M. Acoustic hypochlorite activation in simulated curved canals. J Endod. 2009; 35:1408-1411 https://doi.org/10.1016/j.joen.2009.07.007
Konstantinidi E, Psimma Z, Chávez de Paz LE, Boutsioukis C. Apical negative pressure irrigation versus syringe irrigation: a systematic review of cleaning and disinfection of the root canal system. Int Endod J. 2017; 50:1034-1054 https://doi.org/10.1111/iej.12725
Bystrom A, Claesson R, Sundqvist G. The antibacterial effect of camphorated paramonochlorophenol, camphorated phenol and calcium hydroxide in the treatment of infected root canals. Endod Dent Traumatol. 1985; 1:170-175 https://doi.org/10.1111/j.1600-9657.1985.tb00652.x
Trope M, Delano EO, Ørstavik D. Endodontic treatment of teeth with apical periodontitis: single vs. multivisit treatment. J Endod. 1999; 25:345-350 https://doi.org/10.1016/S0099-2399(06)81169-6
Ørstavik D, Kerekes K, Molven O. Effects of extensive apical reaming and calcium hydroxide dressing on bacterial infection during treatment of apical periodontitis: a pilot study. Int Endod J. 1991; 24:1-7 https://doi.org/10.1111/j.1365-2591.1991.tb00863.x
Edwards DC, Whitworth JM. Does an interim dressing with calcium hydroxide reduce endotoxins between endodontic appointments?. Evid Based Dent. 2021; 22:96-97 https://doi.org/10.1038/s41432-021-0199-6
Ehrmann EH, Messer HH, Adams GG. The relationship of intracanal medicaments to postoperative pain in endodontics. Int Endod J. 2003; 36:868-875 https://doi.org/10.1111/j.1365-2591.2003.00735.x
Segura-Egea JJ, Gould K, Şen BH European Society of Endodontology position statement: the use of antibiotics in endodontics. Int Endod J. 2018; 51:20-25 https://doi.org/10.1111/iej.12781
Abbott PV, Heithersay GS, Hume WR. Release and diffusion through human tooth roots in vitro of corticosteroid and tetracycline trace molecules from Ledermix paste. Endod Dent Traumatol. 1988; 4:55-62 https://doi.org/10.1111/j.1600-9657.1988.tb00295.x
Figini L, Lodi G, Gorni F, Gagliani M. Single versus multiple visits for endodontic treatment of permanent teeth. Cochrane Database Syst Rev. 2007; (4) https://doi.org/10.1002/14651858.CD005296.pub2
Bracciale F, Marino N, Noronha A Bacterial contamination of gutta-percha points from different brands and the efficacy of a chairside disinfection protocol. Eur Endod J. 2020; 5:282-287 https://doi.org/10.14744/eej.2020.44265
Aquilino SA, Caplan DJ. Relationship between crown placement and the survival of endodontically treated teeth. J Prosthet Dent. 2002; 87:256-263 https://doi.org/10.1067/mpr.2002.122014
BDS(Hons) MSc FHEA FDS RCPS(Glasg) FDFTEd FCGDent GDP
The Dental Practice, 21 Rubislaw Terrace, Aberdeen; Hon Senior Clinical Lecturer, Institute of Dentistry, University of Aberdeen; Online Tutor/Clinical Lecturer, University of Edinburgh, UK.
Where primary root canal treatment has failed, case selection is critical. If the reason for failure can be identified and overcome, then this is the main aim of re-treatment. The second of this two-part series discusses ways in which failed cases can be predictably re-treated, using a series of cases to illustrate key points.
CPD/Clinical Relevance: Root canal re-treatment can offer a predictable treatment option with awareness of common pitfalls..
Article
Part 1 of this series discussed potential reasons for endodontic failure and introduced the concept of assessing teeth to determine whether they should be considered for conventional root canal re-treatment, peri-radicular microsurgery or extraction.1 Part 2 now expands this discussion around pre-operative assessment and introduces techniques commonly used for re-endodontic treatment.
Assessment prior to re-treatment
Where a decision is made to undertake non-surgical re-treatment, additional assessment is required. Case selection is essential to providing predictable treatment and obtaining informed consent, with appropriate discussion of risks and benefits. It is essential to ascertain why the root canal treatment (RCT) has failed,1 and whether this can be addressed by further treatment. The following questions should be considered.
Is the tooth restorable?
Irrespective of technical shortfalls, anatomical complexities or iatrogenic errors, restorability of the tooth must be considered before investing clinician and patient time and resources. The dental practicality index (DPI)2 can be a useful tool to aid decisions regarding restorability and explaining these to patients. This assesses the structural integrity of the tooth, periodontal stability, endodontic need and other contextual factors, such as overall restorative needs, social, dental and medical factors. The DPI has been validated, being shown to predict the likely outcome of RCT.3 A first step may be the removal of existing restorations as part of the assessment of restorability, which may identify the reason for failure and critically, the restorability of the tooth. Caries, cracks and marginal breakdown are much more likely to be identified following restoration removal. For example, caries has been identified pre-operatively in 19.2% of teeth, whereas following restoration removal this increased to 86.1%.4 Furthermore, restoration removal will permit direct visualization of subgingival margins enabling a decision between extraction, marginal elevation5 or the ability to place an indirect restoration margin, as well as assessment of ferrule6 and better visualization of angulation for access.
What is the standard of the existing root canal treatment?
Can technical deficiencies be identified and improved? A comprehensive history may identify obvious technical deficiencies. For example, asking a patient whether they remember the use of rubber dam, or asking if they can remember the smell of ‘chlorine’ during treatment. Diagnostic imaging may identify further issues, such as ‘have all canals been treated to an acceptable working length, and if not, will it be possible to locate them?’ Considerations of whether success can be achieved, and whether there is justification for the clinical and financial resources required for re-treatment is important and should be discussed with the patient in an open and honest way.
It may be that more information is needed, such as cone beam computed tomography (CBCT), in order to properly assess the tooth prior to re-treatment. For example, the anatomical apex may be situated up to 3.8 mm from the radiographic apex, and the apical foramen frequently deviates to the side of the apex.7,8 such anomalies should be investigated by use of CBCT, which can be considered a much more precise assessment of the root filling terminus where this is unclear from 2D imaging.9
Is there a fracture or crack?
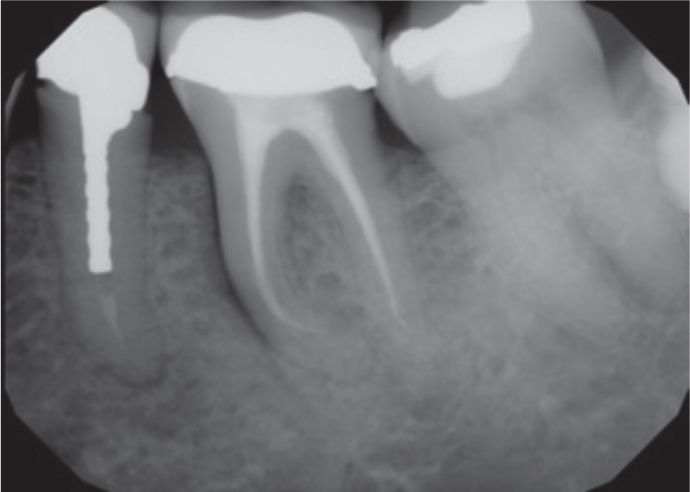
A fracture may be suggested clinically by a single deep narrow periodontal pocket associated with the affected tooth, looseness of a post and/or restoration, J-shaped lesion radiographically (Figure 1), loss of the periodontal ligament space, or through CBCT showing a fracture or pattern of bone loss suggestive of a fracture.10,11 Symptoms can vary, often including pain on biting, even in the endodontically treated tooth (ETT). The use of a tooth sleuth or wooden sticks can aid diagnosis. Dyes, good lighting and, above all, magnification are also beneficial. Where a fracture extends to the root surface, prognosis is often reduced, and treatment options limited to extraction or root resection in the case of molars. Peri-operatively, it may be possible to see a fracture extending down the proximal wall of the access cavity and pulp space, sometimes crossing the floor of the pulp chamber and/or involving a root. The IOWA staging index12 classifies teeth through stages I–IV according to their likely success rate, a probing pocket >5 mm (suggestive of a fracture) is considered stage IV, with the lowest success rate of 41%. In this situation, careful judgement is needed, with recent evidence suggesting these teeth may have a reasonable prognosis in the absence of vertical bone defects.12
Figure 1. The lower left first molar shows a deep radiolucency extending down the mesial aspect of the mesial root, strongly indicative of a root fracture.
Are there missed canals?
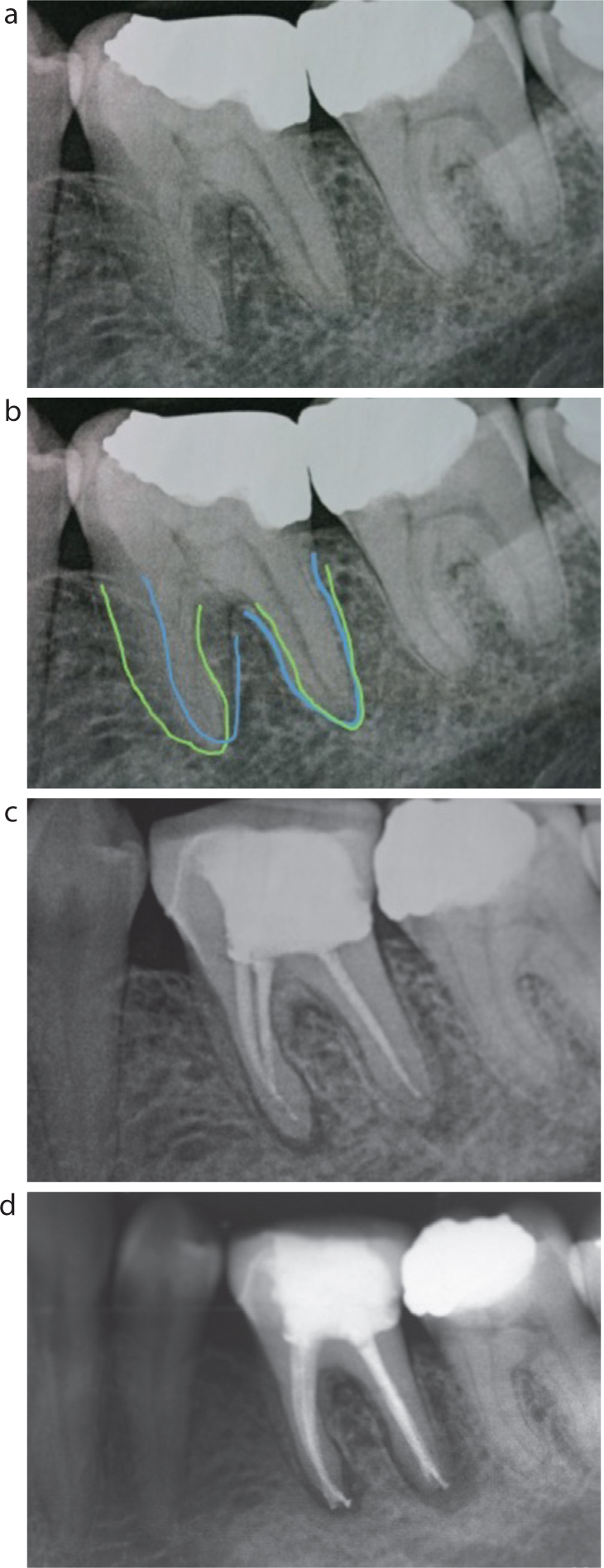
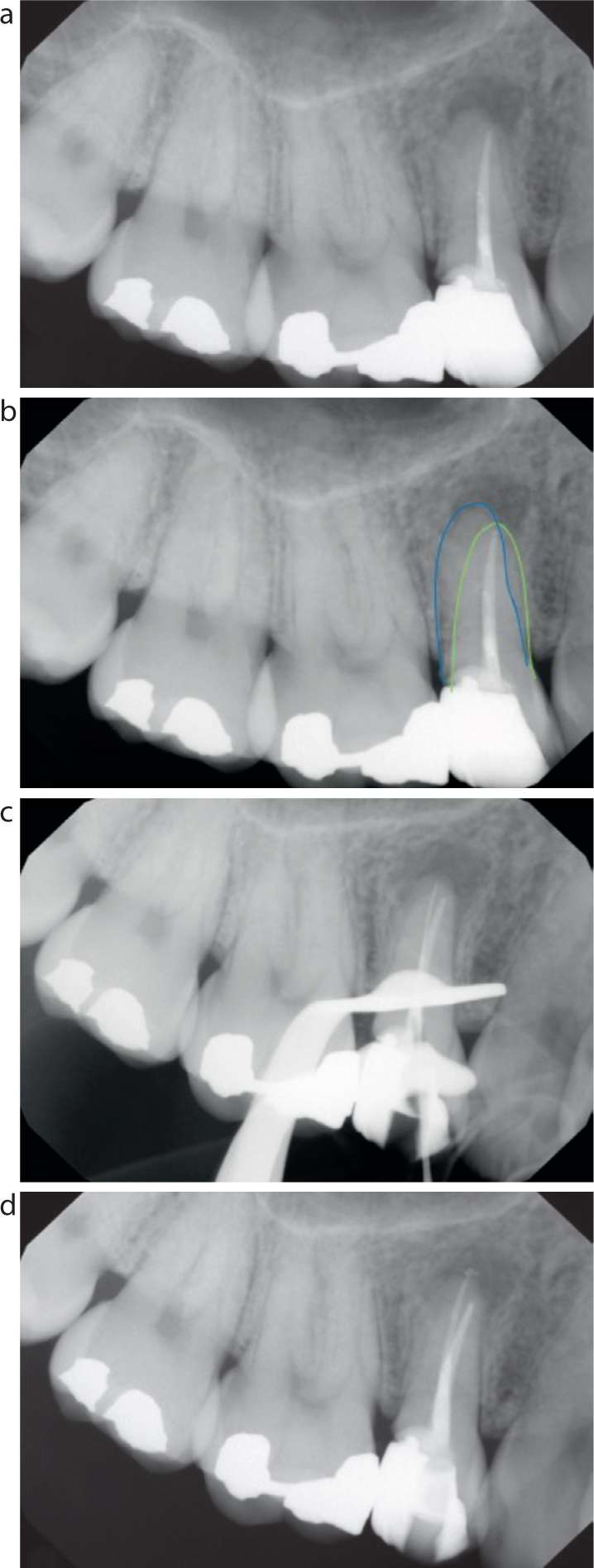
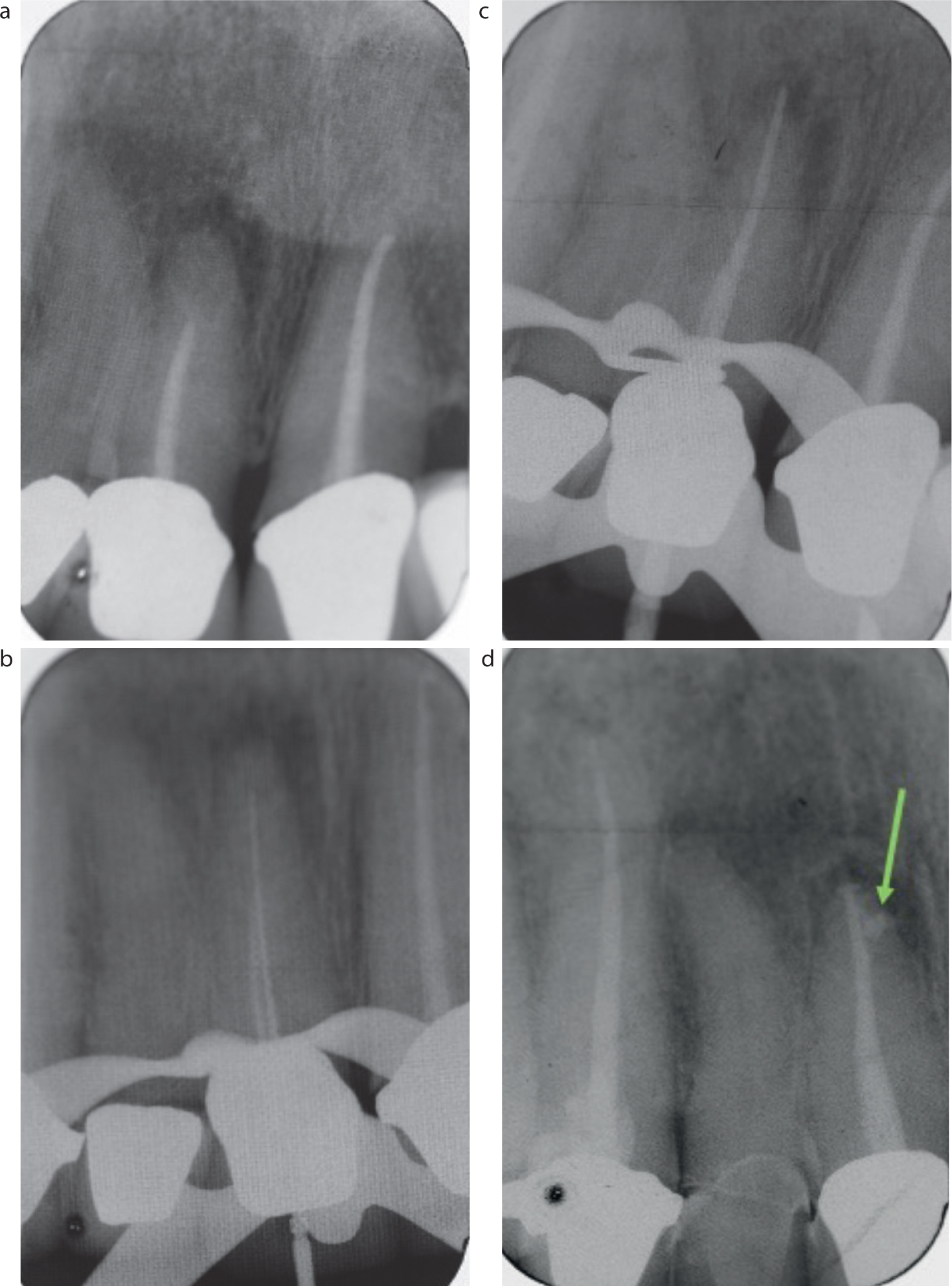
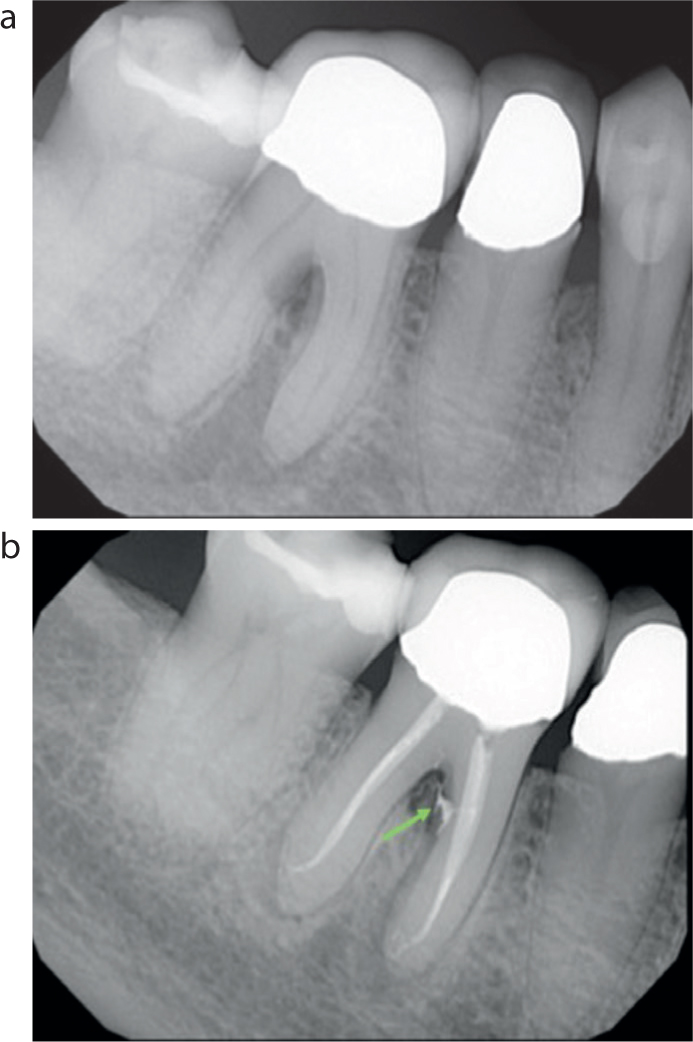
An awareness of the number of canals and the expected anatomy of the tooth is important. Thorough radiographic assessment to look for signs of additional canals on peri-apical radiographs (e.g. a ‘double’ lamina dura) and consideration of the use of CBCT9 are important if additional canals are suspected. Good light and magnification will allow improved location and negotiation of canals and detection of additional canals. Loupes are becoming more accessible in UK clinical practice with over two-thirds of practitioners having access to magnification.13Figure 2 and 3 show an example of missed canals that were contributing to non-healing. The location of bone loss may suggest the presence of lateral canals, which may be accessed and disinfected through careful scouting and active irrigation (Figures 4 and 5).
Figure 2. Re-treatment of LL6. (a,b) Careful assessment of pre-operative radiograph suggests two mesial and two distal canals. In addition to poor obturation, (c) the second distal canal has not been located and symptomatic apical periodontitis has developed. (d) Re-treatment resulted in the location of a second distal canal and improved obturation.Figure 3. (a) Failed endodontic treatment of UR4 with symptomatic apical periodontitis. (b) Evidence of second root canal on periapical radiograph. (c) Location of additional palatal canal and confirmation of working length using 15.02 K-file. (d) Re-treatment of both canals with evidence of bony healing following 6-week period of dressing with non-setting calcium hydroxide and iodoform.Figure 4. (a) Patient presented with symptomatic apical periodontitis of previously endodontically treated UR1. Not only is the obturation short, but the pattern of bone loss suggests the presence of a lateral canal. (b,c) Re-treatment was undertaken, and (d) the lateral canal was ultimately sealed using a thermoplastic obturation technique and bioceramic sealer.Figure 5. (a) Pre-operative radiograph of LR6 demonstrates inter-radicular bone loss and radiolucency. (b) Post-operative radiograph shows the presence of a lateral canal (green arrow) in the mesial root, which explains this pattern of bone loss.
Is there a perforation?
Perforations could be contributing to non-healing and persistent symptoms. They can be identified by magnification and the use of an electronic apex locator, which would give a zero reading. Additionally, the location of a sinus may distinguish between a furcal perforation and apical disease and a Gutta Percha (GP) tracing radiograph can help with this. The European Society of Endodontology position statement on the use of CBCT suggests this may be indicated in non-surgical re-treatment cases where there are suspected untreated canals or perforations and, in these cases, specialist referral may be prudent.14
Orthograde re-treatment technique
Once a decision has been made that non-surgical re-treatment is the most appropriate option and that such treatment is to be carried out in general dental practice, clinical technique and protocols that favour success should be employed.
Isolation
Good isolation is considered essential by the American Association of Endodontists (AAE) for RCT, being essential in re-treatment cases and contributing to successful outcomes.15 The advantages of rubber dam are listed in Table 1. It may be necessary to undertake pre-endodontic ‘build-up’ whereby a definitive or provisional restoration is used to aid rubber dam placement and temporization between appointments (Figure 6).
Table 1. Advantages of using rubber dam during root canal treatment.15
Airway protection
Reduces incidence of hypochlorite injury
Allows the safe use of the most effective irrigants, such as sodium hypochlorite
Prevention of contamination of the root canal system from the oral cavity
Prevention of excessive rinsing
Soft tissue retraction
Improves operator vision
Prevention of inhaling or ingesting dental materials or equipment
Figure 6. The use of composite to build up a heavily broken-down tooth, enabling the placement of rubber dam to permit isolation for successful endodontic treatment.
Previously discussed marginal elevation5 would fall into this category. The use of ‘caulking’ agents can also be useful in rubber dam placement. Examples include Oraseal (Optident, Ilkley, Yorkshire, UK) or Liquid Dam (Henry Schien, Melville, NY, USA).
Access and canal location
When accessing the tooth, it is helpful to align the handpiece and bur with the long axis of the tooth to help achieve straight line access. It has previously been discussed how the removal of existing indirect restorations can be beneficial in this respect; this can allow improved canal location, reduce the amount of tooth tissue removed and prevent technical errors. There is a shift towards a ‘conservative’ access cavity, which have shown higher fracture resistance compared to ‘conventional’ access, although the recently published ‘ninja’ or ‘Truss’ access cavities show no additional benefit in fracture resistance.16 However, fully unroofing of the pulp to gain straight line access, improve visualization and ensure removal of all coronal pulp tissue in root canal re-treatment is usually justified. Once the pulp has been reached, the use of a non-end cutting bur can remove the pulp chamber roof without risking damage to the pulpal floor, or perforation. Areas of calcification and dentine can be removed with fine ultrasonic tips.
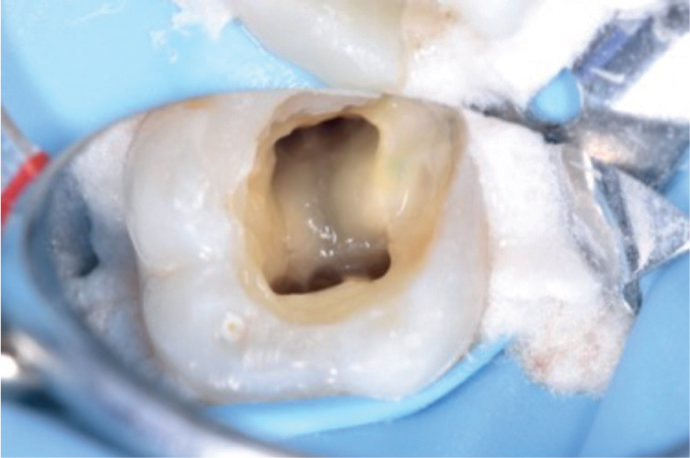
An understanding of the laws of pulp chamber anatomy (Table 2) regarding colour, symmetry, position and distance facilitate canal location and the detection of additional canals.17 If canals do not appear to follow these laws, additional canals may be present that contribute to symmetry and allow fulfilment of such laws, and so should be investigated (Figure 7). In addition, the anatomy of the root canal system must be considered,18 which will offer clues towards root canal location (Figure 8).
Table 2. Krasner and Rankow laws of canal location.17
Law of centrality
The floor of the pulp chamber is always located in the centre of the tooth at the level of the cemento-enamel junction (CEJ)
Law of concentricity
The walls of the pulp chamber are always concentric to the external surface of the tooth at the level of the CEJ
Law of the CEJ
The CEJ is the most consistent, repeatable landmark for locating the position of the pulp chamber
Law of colour change
The colour of the pulp-chamber floor is always darker than the walls
Law of symmetry 1
Except for maxillary molars, the orifices of the canals are equidistant from a line drawn in a mesial distal direction through the pulp-chamber floor
Law of symmetry 2
Except for the maxillary molars, the orifices of the canals lie on a line perpendicular to a line drawn in a mesial-distal direction across the centre of the floor of the pulp chamber
Law of orifice location 1
The orifices of the root canals are always located at the junction of the walls and the floor
Law of orifice location 2
The orifices of the root canals are located at the angles in the floor–wall junction
Law of orifice location 3
The orifices of the root canals are located at the terminus of the root developmental fusion lines
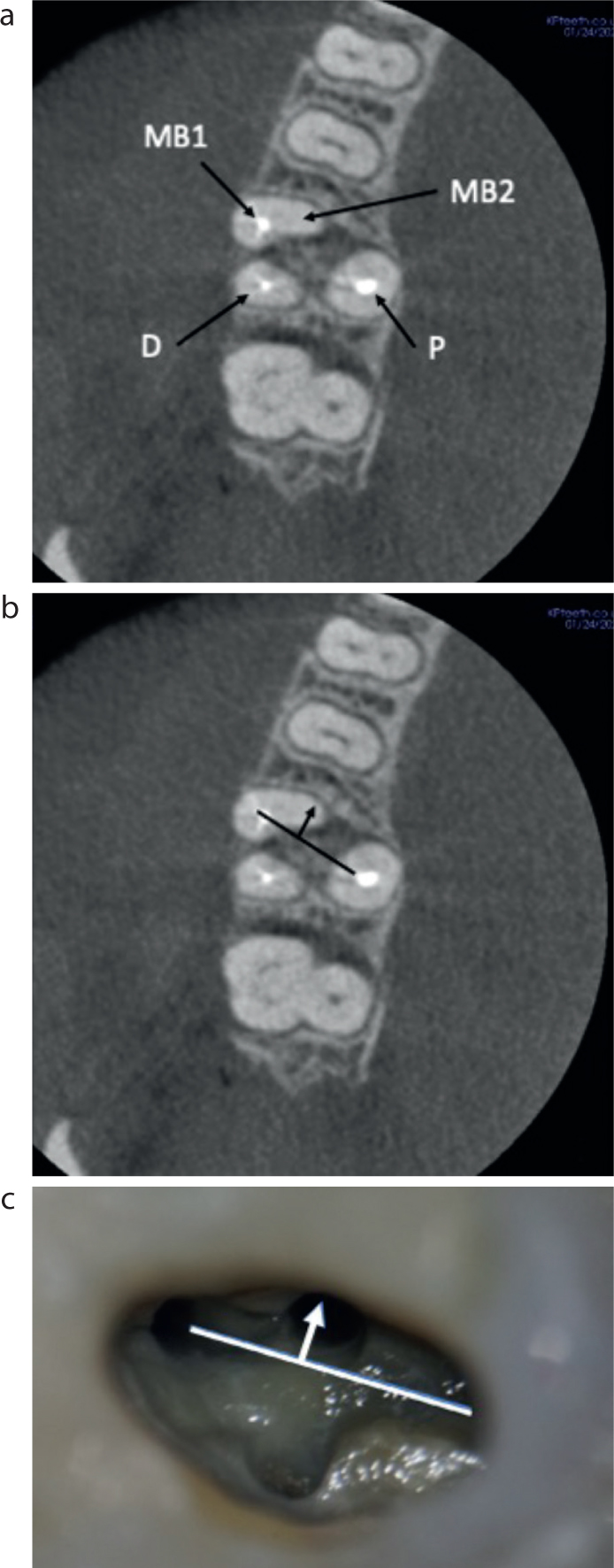
Figure 7. A lower first molar with an additional mesial canal, which, if not located, would significantly increase likelihood of failure.Figure 8. Once the root anatomy is considered, canal location becomes easier. (a,b) The majority of upper first molars have a second mesio-buccal canal (MB2), which is nearly always located to the palatal-mesial aspect of the first mesial buccal canal (MB1). (c) This image shows the typical shape of the MB root in cross section, which correlates with MB2 location.
Root filling removal
In re-treatment cases, there will almost always be existing GP in canals that requires removal, prior to shaping, disinfection and obturation. There are multiple techniques to remove existing root canal fillings, which can be classified as mechanical, chemical or thermal. In the case of a missed canal, a decision will need to be made whether to re-treat the obturated canal(s) or not – the anticipated ease of GP removal (e.g. presence of a separated instrument) and presence of apical periodontitis associated with that root will ultimately drive the decision. In many cases, GP removal can be straightforward, and the desirable approach is therefore to re-treat all canals.
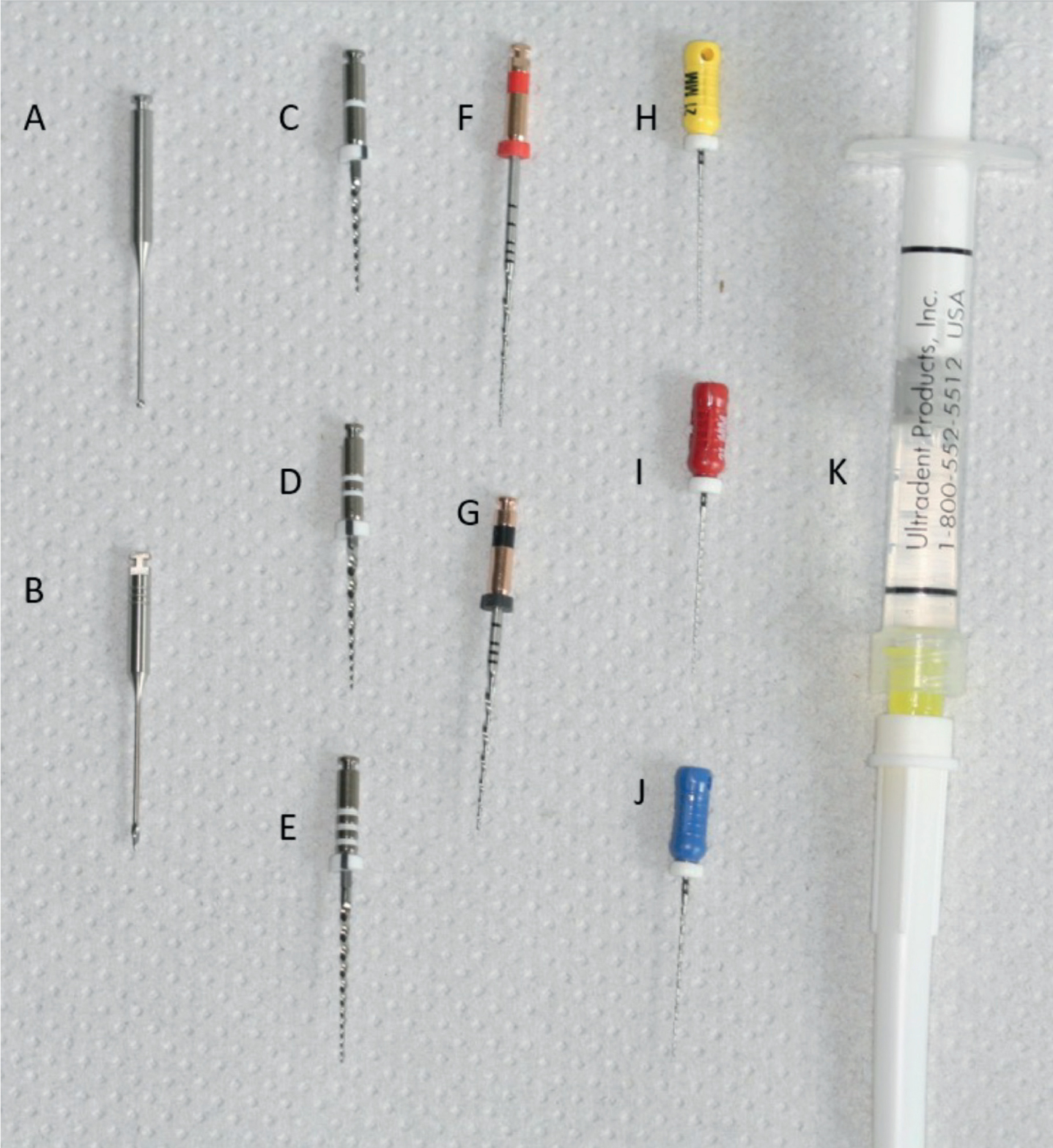
Gates Glidden burs rotary and reciprocating files and Hedström files are a useful armamentarium for mechanical removal and often will succeed in complete removal (Figure 9). In addition, goose-neck burs can be helpful to explore the pulp chamber, but caution should be applied to avoid iatrogenic damage. A 45° bend in a file or finger spreader can aid removal of GP fragments from lateral walls of canals. In cases where GP is overextended and requires removal, curving the tip of a Hedström file can be helpful. This can be achieved digitally by curving the file around the mirror handle or using an endo-bender. Specific rotary/reciprocating instruments for GP removal are available from several file systems (e.g. ProTaper D Files, Dentsply Sirona, Charlotte, NC, USA), but standard reciprocating systems (e.g. Reciproc, VDW Dental, München, Germany) can be extremely effective.
Figure 9. Armamentarium for tackling re-treatment cases. (A) Goose neck bur; (B) Gates Glidden 3; (C–E) Re-treatment files, such as ProTaper D1–D3; (F–G) non-heat treated reciprocating NiTi files, such as Reciproc 25,40; (H–J) Hedstrom files size 20–30; (K) solvent such as chloroform, Endosolv, eucalyptol.
A recommended removal protocol is:
Locate the canal orifice, using a goose neck bur to remove coronal GP, if necessary.
Simply using a reciprocating system directly in the canal will, in many cases, be sufficient to remove the GP.
Alternatively, if this is not successful, a crown down approach using Gates Glidden drills followed by Hedström files is effective. The Hedström files can be repeatedly rotated into the mass of GP rather than the walls of the canal, and ideally this will result in remaining GP being removed in a single piece (Figure 10).
Figure 10. (a,b) Fibre post and GP points removed using Hedstrom files. Interestingly the progression of biofilm from coronal microleakage is obvious. (c) The use of Hedstrom files to remove a single Gutta-Percha point.
Chemical techniques involve the use of solvents such as chloroform, eucalyptol, orange oils or bespoke solvents such as Endosolv (Septodont, Maidstone, Kent), which is a mixture of ethyl acetate, amyl acetate and thymol. Once used, it can be difficult to retrieve the GP in a single piece, and there is significant evidence that they result in increased remnants of sealer and GP on the canal walls, therefore the authors recommend that this is only used when mechanical retrieval is insufficient, or remaining GP that cannot be removed mechanically is visible on a radiograph. Paper points are recommended to remove softened GP following the use of solvents. Where canals are particularly curved, careful chemical retrieval of GP with chemical solvents may also be considered a safer approach.
Thermal techniques for removal include the use of devices designed for warm vertical condensation, such as System B (SybronEndo, Orange, CA, USA) or Elements (KerrDental, Uxbridge, UK). Thermal approaches can rapidly heat and remove the coronal portion of GP. Although useful in wide canals, these systems will only soften GP in the coronal portion of the canal, and alternative techniques are needed for the apical portion.
Preparation and disinfection
In re-treatment cases, primary failure can often be attributed to residual micro-organisms in the root canal system, therefore their elimination is critical for success.19 A negative bacterial culture prior to obturation was associated with significantly higher success rates than those with positive culture results.20,21 Mechanical instrumentation only reaches a proportion of the canal system, with 35–53% of the root canal system remaining uninstrumented by mechanical techniques alone.22 Irrigation and disinfection are essential to reach anatomical areas that filing cannot. In chronic infection, micro-organisms enter the dentinal tubules and accessory canals and cannot be retrieved by mechanical instrumentation, therefore supplementary disinfection in these areas is required.23 Failure can also be attributed to persistent micro-organisms or occasionally, viruses. Other irrigants may include povidone iodine, which has antibacterial and antiviral effects. This has been discussed in detail in Part 1,1 but with root canal re-treatment, special consideration must be given to gaining access to lateral canals and optimising dentine disinfection. The smear layer contains micro-organisms and nutrients and can prevent complete disinfection of the root dentine, therefore its removal is recommended.24 A systematic review has found the combination of NaOCl and 17% EDTA to improve prognosis in re-treatment cases7 and aid removal of the dentinal smear layer, allowing deeper penetration of the irrigant. The penultimate rinse should be with EDTA, and a final rinse with NaOCl to neutralize residual acidic effects from the EDTA and because EDTA may leave the organic portion of the smear layer behind.22
Greater efficacy can be achieved with agitation techniques in addition to heating and using increased concentrations of solutions in the case of NaOCl25. Agitation has a greater effect than temperature by improving flow through the canals, and is a critical step.25,26 This can be achieved manually with files or GP points (‘GP pumping’), ‘endo activators’, or by activating a file within the canal containing the irrigant using ultrasonics – this facilitates microstreaming and cavitation, as well as increasing penetration into dentinal tubules.24,26,27 These approaches eliminate air bubbles that can prevent irrigant reaching the full length of the root and are effective in pushing disinfectant solutions to all parts of the root canal system. Bespoke devices such as specific ultrasonic tips can be useful, and negative pressure irrigation syringes have recently been introduced to the market, although their effectiveness remains uncertain.28Figure 11 models and compares the effectiveness of irrigation with and without activation.
Figure 11. (a) An endodontic training block was prepared to length using a Reciproc system up to size R-25 and filled with black ink. (b) The canal was irrigated using a 27-gauge needle to length only, with (c) additional manual GP activation and with (d) additional activation of a size 10 K file with ultrasonics. (e) A previously extracted, single-rooted adult premolar tooth with a relatively straight root was prepared to length up to size 25.08 (Reciproc 25) and then sectioned. The image shows the depth to which a 27 gauge irrigation needle was able to reach within the tooth and the length of canal remaining that was not reached, highlighting the area that may remain un-irrigated unless activation techniques are used. Devices for activating irrigant: (f) ‘Endo Activator’; (g) and ultrasonic activator.
Based on the evidence available, the authors recommend the following disinfection protocol: 24
Flush canal(s) for at least 1-minute with ≥1% NaOCl;
Activate NaOCl with ultrasonics, endo activators or manual GP agitation;
Second rinse with ≥1% NaOCl;
Rinse with 17% EDTA for 1 minute;
Final rinse with ≥1% NaOCl for 1 minute;
Dry with paper points.
Temporization
Inter-appointment calcium hydroxide dressings have been shown to contribute to additional antimicrobial action compared to mechanical instrumentation and irrigation alone. Calcium hydroxide is bactericidal, denatures proteins and stimulates calcified tissue formation. These dressings are more likely to result in a negative bacterial culture within the canal system and have been associated with improvements in peri-apical health and treatment outcome in re-treatment cases.21,29,30,31,32,33 Antibiotic-steroid dressings (most commonly Ledermix (Ozdent, NSW, Australia) and Odontopaste (ADM, Queensland, Australia)) also demonstrate efficacy against endodontic bacteria, as well as the ability to diffuse through dentinal tubules to reach the periodontal and peri-apical tissues, and may reduce post-operative pain.32,34 However, the ESE position statement on the use of antibiotics in endodontic treatment reports limited evidence to support their use in root canal disinfection owing to risk of resistance of micro-organisms to tetracyclines, fungal growth and discolouration when used as intracanal medicaments, and their use is discouraged.35 Furthermore, the majority of the antibiotic component leeches out of the tooth, leading to systemic exposure and increasing risk of developing antimicrobial resistance.36 Symptomatic teeth contain higher bacterial levels31 and therefore in re-treatment cases, particularly when symptomatic, intracanal dressing with calcium hydroxide between appointments is strongly recommended.
Although this two-stage approach facilitates intracanal medication and has also been associated with reduced levels of post-operative pain,37 it provides an opportunity for leakage and bacterial ingress that can compromise treatment outcome, therefore adequate temporization is essential between appointments. Inadequate temporary restorations have been associated with continued pain during endodontic treatment.38 The restoration must be sufficient to prevent leakage of fluids and bacteria into the canals and escape of the dressing from the canals, therefore, satisfactory thickness and sealing of restorations is important, and these should ideally be in situ for a short period of time only.39 The authors recommend using glass polyalkenoate (glass ionomer) cement, with polytetrafluoroethylene (PTFE) tape packed into the access cavity to aide re-access. If sterile PTFE tape cannot be sourced within dental practice, it can be wrapped around wooden spatulas and autoclaved, or alternative options include sterile sponge.
Obturation
Following GP removal, thorough disinfection, and a period of at least 2-weeks with an intracanal dressing, the patient should be reviewed.33 If symptoms have resolved, it is appropriate to obturate, following calcium hydroxide removal and further disinfection using the protocol described above. Activation of irrigant solutions is the optimal way to remove all remaining intracanal dressing. Where the tooth remains symptomatic, it may be appropriate to disinfect the tooth again and re-dress with calcium hydroxide. If the tooth continues to remain symptomatic, it is sensible to investigate the cause prior to obturation. For example, could there be a fracture in the tooth or a missed additional canal? Any further investigations such as a CBCT scan may be ideal at this time, ensuring radiopaque dressings, such as calcium hydroxide, are removed to minimize scatter.
The apical extent of the root canal filling is essential to the healing of a peri-apical lesions, over-extrusion can reduce success and the highest likelihood of successful outcome is achieved with a flush root canal filling.22 Confirmation of working lengths using an electronic apex locator before taking master cone radiographs at this confirmed length is important to ensure the canal is filled to the apical constriction, but not beyond.
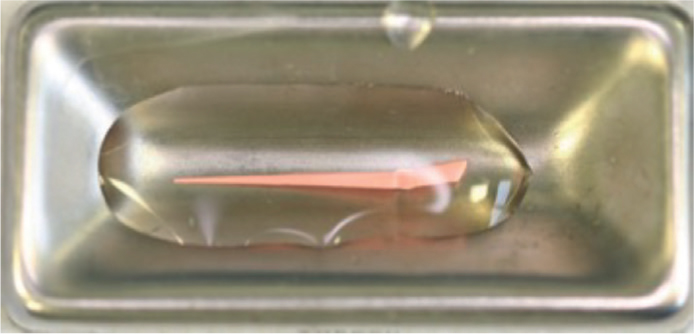
Since GP points are non-sterile, chairside submersion in NaOCl prior to obturation has been shown to be effective and is recommended by the AAE (Figure 12).40,41 This will disinfect and reduce the likelihood of introducing additional bacteria into the canals, which in the event of re-treatment, is likely to contribute towards success.
Figure 12. Submergence of a Gutta Percha point in sodium hypochlorite for disinfection prior to obturating a canal.
Restoration
Teeth can be weakened by endodontic treatment owing to the tooth tissue lost, loss of pulp tissue providing proprioception, and the use of NaOCl and calcium hydroxide that may degrade collagen42 and therefore, a suitable restoration is required following completion of treatment. As is the case following primary endodontic treatment, teeth should be restored with a sufficient coronal seal immediately following obturation, and cuspal coverage is recommended for posterior teeth, particularly if there is loss of a lot of coronal structure, including the marginal ridge.42,43
Follow up and review
As with primary treatment, endodontic treatment should be reviewed clinically and radiographically after a year,44 looking for favourable and unfavourable signs and symptoms of healing (see Table 1 in Part 11).
Conclusion
This two-part series has discussed the assessment of root canal treatment and how to determine whether re-treatment is an appropriate option, as well as considering when this can be carried out in general dental practice. Recommended protocols have been provided to help the general dental practitioner apply clinical techniques to maximize the likelihood of successful re-treatment