Patel S, Brown J, Semper M European Society of Endodontology position statement: use of cone beam computed tomography in endodontics. Int Endod J. 2019; 52:1675-1678 https://doi.org/10.1111/iej.13187
Patel N, Gemmell A, Edwards D. When to consider the use of CBCT in endodontic treatment planning in adults. Dent Update. 2021; 48:932-941
Brown J, Jacobs R, Levring Jäghagen E Basic training requirements for the use of dental CBCT by dentists: a position paper prepared by the European Academy of DentoMaxilloFacial Radiology. Dentomaxillofac Radiol. 2014; 43 https://doi.org/10.1259/dmfr.20130291
Wenzel A. Radiographic display of carious lesions and cavitation in approximal surfaces: advantages and drawbacks of conventional and advanced modalities. Acta Odontol Scand. 2014; 72:251-264 https://doi.org/10.3109/00016357.2014.888757
Patel S, Brown J, Pimentel T Cone beam computed tomography in Endodontics – a review of the literature. Int Endod J. 2019; 52:1138-1152 https://doi.org/10.1111/iej.13115
Matherne RP, Angelopoulos C, Kulild JC, Tira D. Use of cone-beam computed tomography to identify root canal systems in vitro. J Endod. 2008; 34:87-89 https://doi.org/10.1016/j.joen.2007.10.016
Pinheiro BC, Pinheiro TN, Capelozza AL, Consolaro A. A scanning electron microscopic study of hypercementosis. J Appl Oral Sci. 2008; 16:380-384 https://doi.org/10.1590/s1678-77572008000600005
Bonsor SJ. Disinfection of the root canal system: what should the protocol be?. Dent Update. 2021; 48:836-844
Ng YL, Mann V, Gulabivala K. A prospective study of the factors affecting outcomes of nonsurgical root canal treatment: part 1: periapical health. Int Endod J. 2011; 44:583-609 https://doi.org/10.1111/j.1365-2591.2011.01872.x
Rodríguez G, Patel S, Durán-Sindreu F Influence of cone-beam computed tomography on endodontic retreatment strategies among general dental practitioners and endodontists. J Endod. 2017; 43:1433-1437 https://doi.org/10.1016/j.joen.2017.04.004
Lai PT, Yang SF, Lin YM, Ho YC. Computer-aided design-guided endodontic microsurgery for a mandibular molar with hypercementosis. J Formos Med Assoc. 2019; 118:1471-1472 https://doi.org/10.1016/j.jfma.2019.06.007
Radiography plays an integral role in endodontics. However, conventional radiographic techniques have limitations, such as background noise, providing only a two-dimensional representation of the image, superimposition and distortion. Cone beam computed tomography (CBCT) provides the clinician with a three-dimensional image of the structures involved in the clinical situation. When considering options for endodontic re-treatments, it is vital to identify the cause of the initial failure and here, the use of CBCT images can be beneficial. This is illustrated through an endodontic re-treatment case owing to a palatal canal missed with conventional radiographic techniques.
CPD/Clinical Relevance: Cone beam computed tomography can be beneficial in cases of endodontic re-treatment.
Article
When faced with a recurrent apical infection following primary endodontic treatment, the clinician must first identify the cause of the failure before embarking on re-treatment. Endodontic re-treatment can include non-surgical and surgical procedures. Radiography plays an integral role in endodontics; however, conventional radiographic techniques have limitations, such as background noise, providing only a two-dimensional (2D) representation of the image, superimposition and distortion.1,2
Following appropriate training in the use and reporting of cone beam computed tomography (CBCT),3 endodontic specialists, dentists with a special interest in endodontics, as well as general dental practitioners (GDPs) can now readily acquire three-dimensional (3D) images of the structures involved in the clinical situation in the form of CBCT scans. CBCT imaging can help overcome the various limitations affecting traditional peri-apical radiographs.1 However, the application of CBCT imaging should be considered on a case-by-case basis as CBCT does involve greater radiation exposure4. Factors influencing exposure dose include the CBCT unit being used, as well as the case requirements (ie size of the area being assessed).1
Clinicians still need to follow the ‘as low as reasonably achievable’ (ALARA) principle, as well as ensure a justification is recorded and informed consent gained. Following CBCT exposure, a report must be completed that records all clinically relevant and incidental findings, and when required, a second opinion gained.
Clinical case
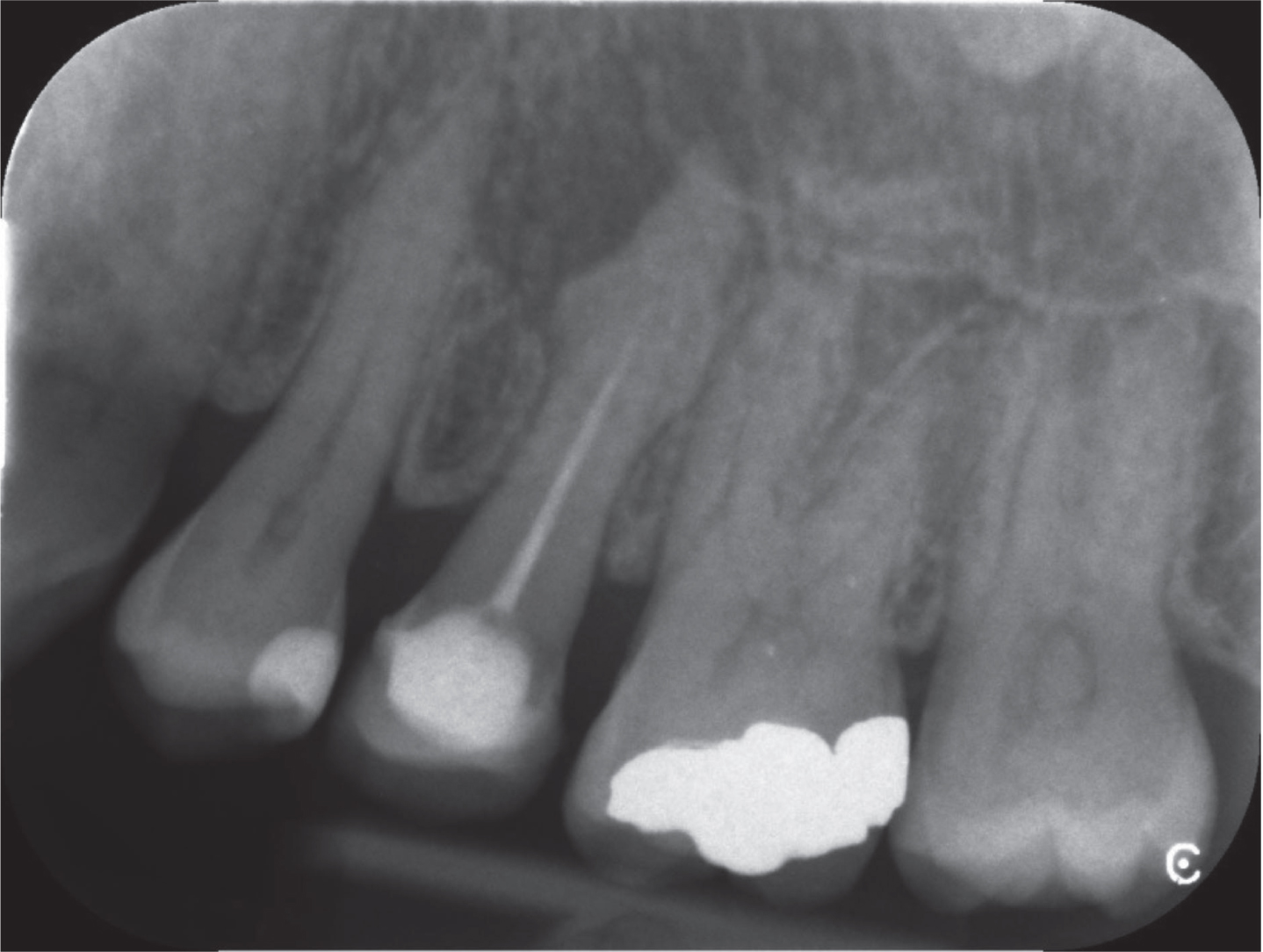
The following patient was referred for an assessment of the restorability and suitability of the tooth for endodontic re-treatment. A medically fit and well female patient, aged 51 years, was referred complaining of toothache and a swelling associated with her upper left second permanent premolar (UL5). This tooth had previously been restored with a laboratory-made temporary crown. Clinically, there was a 3-mm pocket associated with the buccal aspect of the tooth, which was grade 1 mobile. The temporary crown was restoratively sound, and the tooth was asymptomatic (no tenderness to percussion, or pain on pressure). No obvious sinus was noted either. Both the upper left first premolar (UL4) and first molar (UL6) were were positive to endo frost, although mesial caries was noted clinically in UL6. A peri-apical radiograph (Figure 1) was received with the referral showing the upper left canine, first and second premolar and molars (UL34567). The UL5 demonstrated an insufficient primary root treatment with a short root filling, and a large radiolucency was noted associated with the UL5. Furthermore a more complex apical anatomy was noted with UL5, with a thickened, abnormally shaped apical region characteristic of hypercementosis. Furthermore, and importantly, no obvious missed canal was noticeable at this angle.
Figure 1. Pre-operative peri-apical radiograph of UL5.
A diagnosis of chronic apical periodontitis associated with a failed primary endodontic treatment was made and the patient was given the following options:
No treatment (not advisable);
Re-treatment (non-surgical or surgical);
Extraction.
The patient opted for non-surgical endodontic re-treatment. At this point the potential need for an additional peri-apical radiograph at a different angle was discussed to see whether more information about the tooth could be gained. The potential use for a CBCT view of the tooth was considered and the patient was happy for it to be taken. The justifications for taking a CBCT scan of UL5 were:
The peri-apical did not provide the detail needed to ascertain why the primary treatment failed. Was it a missed canal or simply a short primary treatment?
The tooth may have more complex anatomy associated with the apical region.
It would enable the extent of the lesion, and also the current root filling to be assessed.
The author also discussed the use of a CBCT view of this tooth with two other endodontists and a consultant in restorative dentistry, with the majority confirming they would take a CBCT.
When comparing a CBCT view to a traditional peri-apical view of this tooth, peri-apical radiographs are likely to underestimate the true anatomical complexity of the root system, and this was important to consider in this case.5 A 2008 in vitro study demonstrated that endodontists failed to identify at least one canal in up to 41% of cases evaluated with a traditional peri-apical view when compared to CBCT.6 CBCT investigation improves the identification, location and evaluation of teeth with anomalous anatomy5 and improves the quality of referrals for specialist treatment. Therefore, the CBCT scan was tailored to the individual patient and diagnostic needs, and the benefits of the scan outweighed the risks of the exposure.
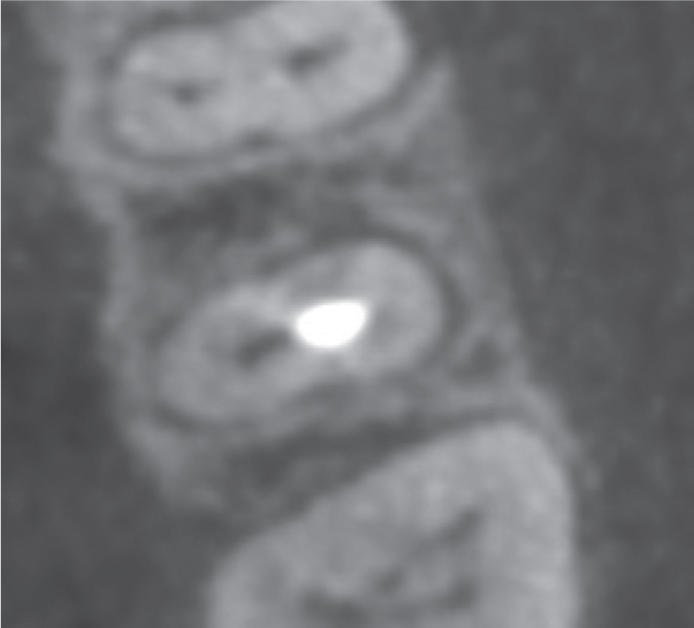
The patient was sent for a CBCT scan of the upper left quadrant including the UL3456. Following the CBCT scan, it was clear that the UL5 had an additional untreated canal palatally (Figure 2).
Figure 2. Axial CBCT view showing the missed canal palatally at UL5.
The scan also highlighted that the buccal canal was blocked apically. The cause of this blockage was unknown, but may have been related to previous treatment, or was potentially hypercementosis. A 2008 scanning electron microscopic study of hypercementosis demonstrated, in severe cases, a decrease in the number, and, sometimes obliteration, of the apical foramens.7 Treatment of the UL5 therefore required re-treatment of the buccal canal and the identification and treatment of the palatal canal. This treatment was completed over the course of three visits.
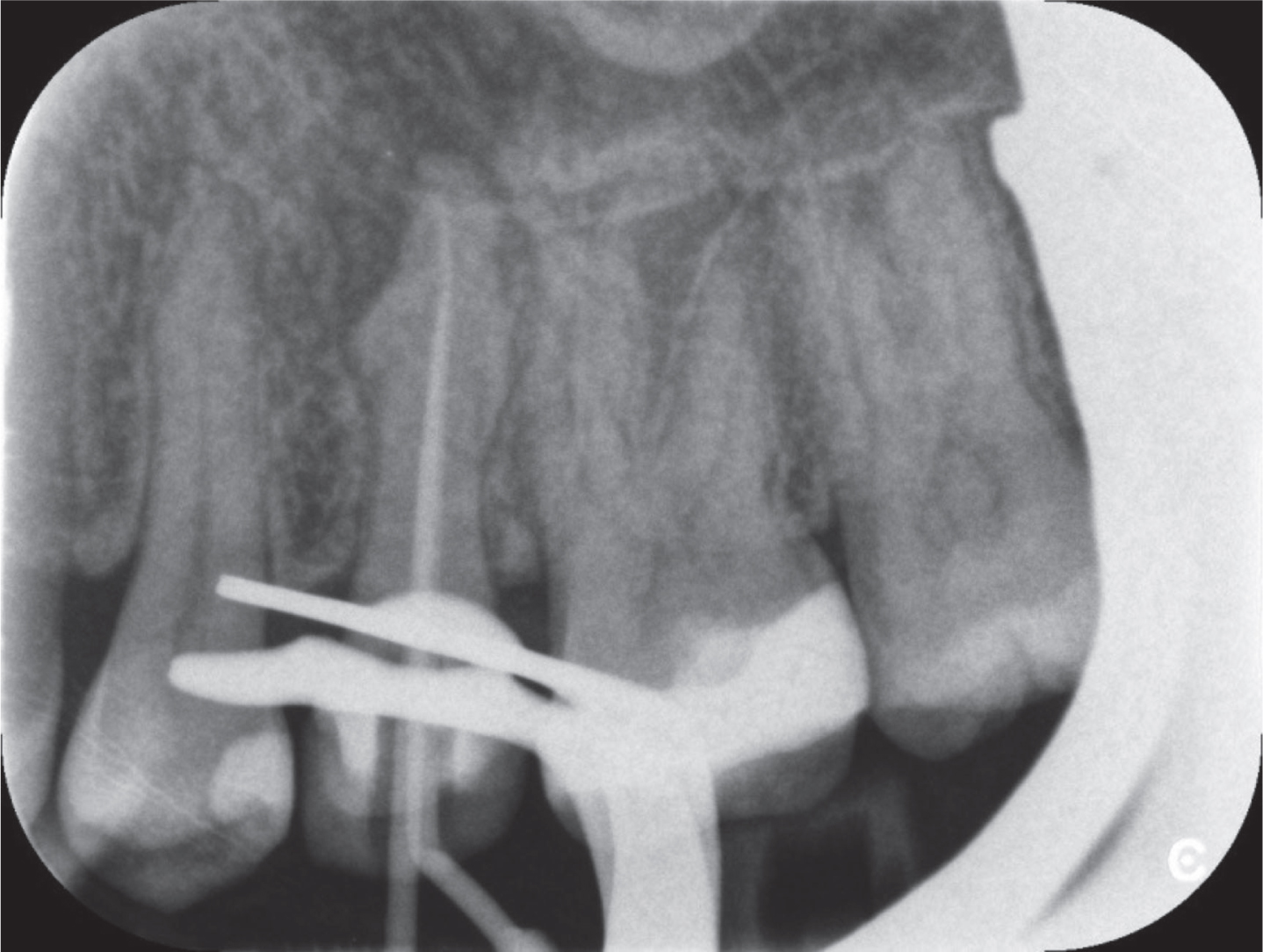
All treatment was completed under rubber dam isolation, using a dental operating microscope (Zeiss Extaro 300, Nuview Ltd). In the first session, the canals were located and the primary root filling was removed using the D1/2 Protaper Retreatment files (Dentsply Sirona) as well as the Acteon Ultrasonic Retreatment tips (Acteon Group Ltd, UK). The buccal canal was blocked and not patent. The palatal canal was recorded as 20.5 mm using an electronic apex locator (Morita Root ZX Apex Locator, J Morita Corp, Japan). Both canals were irrigated with sodium hypochlorite and patency was maintained in the palatal canal using a size 10K file to working length. At the end of this session a peri-apical showed that the majority of the previous root filling material had been removed (Figure 3).
Figure 3. Peri-apical radiograph taken at the end of the first session (note the restoration of caries identified in the UL6 completed by referring dentist).
The second session involved further preparation of both canals to F2 (Protaper Gold, Dentsply Sirona), the palatal canal being shaped with the S1/2 and F1 files first. Both canals were irrigated with sodium hypochlorite. Patency was maintained in the palatal canal as described previously. At this point, the tooth was ready for obturation, having remained asymptomatic since the first visit. However, because of the size, extent (Figure 4) and chronic nature of the lesion, it was decided to dress the tooth with non-setting calcium hydroxide.
Figure 4. (a) Sagittal and (b) axial CBCT views showing the extent of the lesion on the UL5.
The patient returned after a period of 1.5 months, partly due to restrictions in patient and dentist availability. At this appointment, the patient reported no further issues with the tooth. Clinically, there was no tenderness to percussion or finger pressure, mobility or swelling associated with the tooth. The patient did not report the need for pain relief or the experience of the discomfort she had before the start of treatment. Therefore, the decision to obturate the tooth at that appointment was made.
A pre-obturation cone fit peri-apical radiograph was taken (Figure 5) and the tooth was rinsed with sodium hypochlorite and prepared again with the F2 file to remove the dressing material. The canals were rinsed with sterile water to remove any residual sodium hypochlorite before the use of 17% EDTA. Sodium hypochlorite and EDTA interact chemically.8 The canals were then irrigated with 17% EDTA to remove the smear layer, which has been shown to have a positive effect on clinical outcomes in re-treatments.9 The canals were dried with paper points, and the canals remained dry, pus and blood free. The canals were obturated with F2 gutta perch matching points, AH plus sealer and accessory cones to the lengths prepared using cold lateral condensation (Figure 6). The orifices were covered with light-cured RIVA (SDI Ltd) glass ionomer cement, and then the access cavity was restored using etch, bond and SDR (Dentsply Sirona).
Figure 5. Pre-obturation cone fit radiograph.Figure 6. Post-obturation peri-apical radiograph at UL5.
The patient was discharged back to the referring dentist for routine dentistry. The tooth had already been restored with a laboratory-made temporary crown, which provided cuspal protection. Long term, if the tooth remained asymptomatic and the lesion showed signs of apical healing, then a new definitive crown could be provided.
Discussion
This case demonstrated the use of CBCT imaging in aiding the diagnosis of a failed primary root treatment. A 2017 study by Rodriguez et al investigated the impact of CBCT imaging on clinical decision making among GDPs and endodontists after failed root canal treatment.10 Eight patient cases were used, involving endodontically treated teeth diagnosed with symptomatic apical periodontitis, acute apical abscess or chronic apical abscess. These cases were given (along with clinical photographs and peri-apical radiographs) to examiners (80 GDPs and 40 endodontists) who were asked to choose their treatment plan and to assess the difficulty in clinical decision making.10 One month later the examiners reviewed the cases alongside the CBCT data. The results indicated changes in treatment planning in 49.8% of the cases.10 Therefore, CBCT imaging does influence clinical decision making with respect to endodontic re-treatment cases.
In this case, the traditional peri-apical radiograph lacked sufficient detail regarding a potential missed canal as well as anatomy of the apical region. CBCT has proved beneficial in the management of atypical root morphology including hypercementosis.11 The CBCT views are superior when identifying additional or supplement canals2 and helped to locate the presence and positioning of the missed palatal canal in this case. The application of a CBCT scan was justifiable in this case because it provided more diagnostic information about the UL5 than the traditional peri-apical radiograph. This additional information supplemented the consent process because it provided more information about the tooth for both the clinician and the patient. Furthermore, if needed, the data from the CBCT images could have facilitated an appropriate referral for specialist care.