
Article
Hyoid bone ghosting on panoramic radiographs
We saw a 56-year-old gentleman who presented with a 4-week history of slow growing swelling of floor of the mouth and refractory pain. He had visited an emergency dentist who noted that his lower left canine and first premolar were infected and loose, and advised a course of antibiotics. During this course, the lower left first premolar tooth exfoliated on its own. He also complained of odynophagia and throat pain. His past medical history was insignificant. He smoked about 10 cigarettes/day and consumed on average, approximately 56 units of alcohol per week.
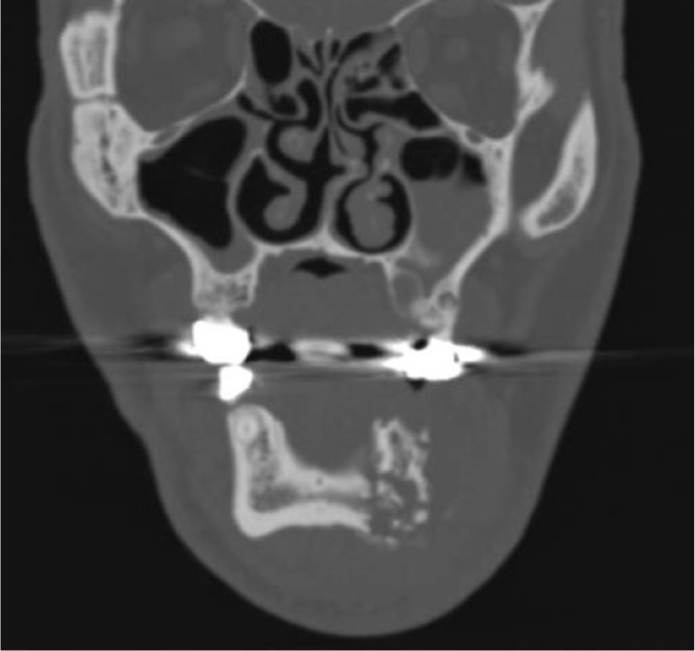
On examination, he had firm submental swelling measuring approximately 4–5 cm in diameter with overlying erythema. Additionally, there was a firm, non-tender swelling of the floor of the mouth with an open socket of lower left first premolar tooth (LL4) showing pus discharge. The lower left canine tooth (LL3) was Grade 3 mobile and non-tender. The associated gingiva was firm and indurated. No obvious worrying signs of airway compromise were noted. A panoramic radiograph (Figure 3) showed an empty socket of LL4 and pronounced bone loss associated with LL3. The lower left first molar tooth was grossly decayed. There were faint lucent lines on the associated mandibular bone. There was increased amount of hyoid bone and cervical spine ‘ghosting’ of the left mandibular region preventing further analyses. A CT scan was requested that showed destructive process of the left mandible leading to pathological fracture. Histopathological evaluation of bone was consistent with chronic osteomyelitis of the jaw (Figures 4 and 5).
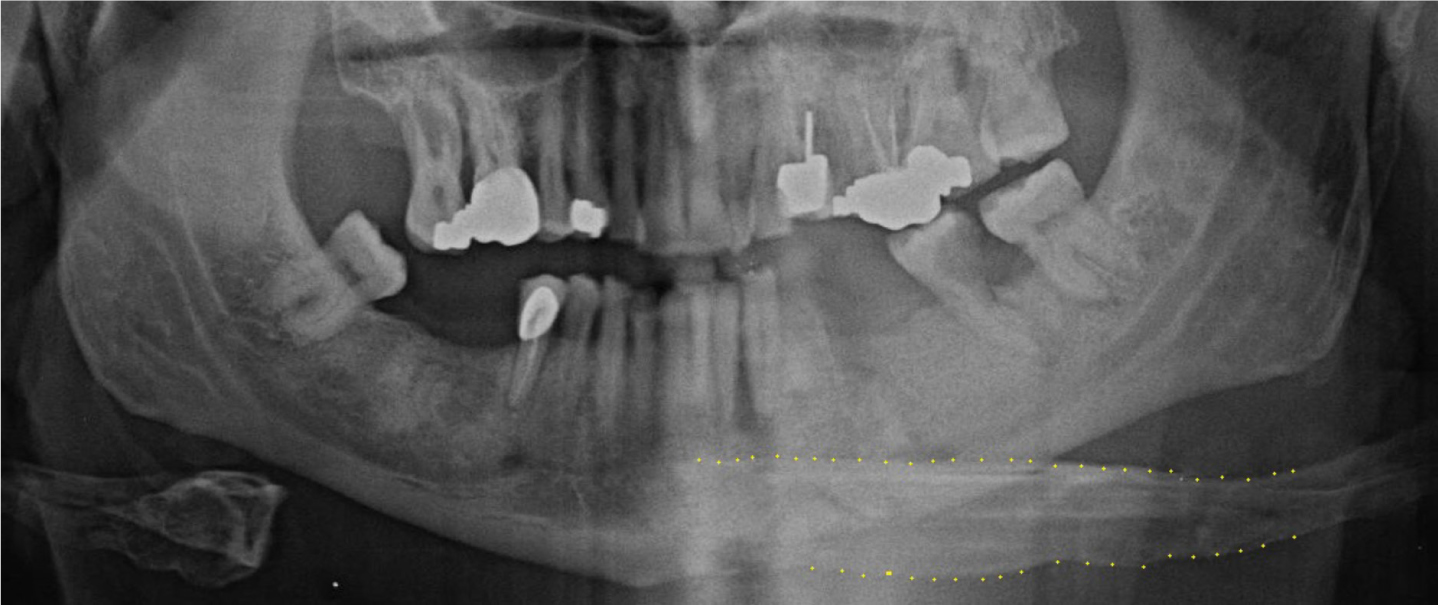

Panoramic radiographs are an important and primary investigation in secondary care for patients presenting with orofacial/cervical infections. Unfortunately, they are riddled with deficiencies and errors that compromise a clinician's ability to diagnose accurately. Various studies have been performed to highlight the level of errors made on panoramic radiographs. Rushton et al reported that out of 1813 radiographs taken, 99.2% had errors.1 The hyoid bone is a ‘U’-shaped structure situated in the anterior neck. It is usually notable on a panoramic radiograph inferior to the mandibular ramus bilaterally, when the patient is in optimal positioning. Often, when the chin is tipped too low (ie the Frankfurt plane not being parallel with the floor) during the imaging process, it can cause an elongated double or ‘ghost’ image of the hyoid bone onto the ramus of the mandible, causing a more radio-opaque region to appear apical to the mandibular teeth. This could be perceived as normal anatomy whereby disease may be masked. In fact, one study found that superimposition of the hyoid bone had occurred in 26.3% of cases – the second most common error reported, although this is rarely discoursed in literature.2 It is important that we, as clinicians, can recognize these deficiencies and errors to determine whether further investigation is necessary in aiding diagnosis.