National Institute for Health and Care Excellence. Stable angina: management. Clinical guideline CG126. 2016. https://www.nice.org.uk/guidance/cg126 (accessed January 2023)
Ciantar M, Gibson J. Nicorandil-induced oral ulceration. Malta Medical J. 2008; 20:(1)
Dunn N, Freemantle S, Pearce G Safety profile of nicorandil – prescription-event monitoring (PEM) study. Pharmacoepidemiol Drug Saf. 1999; 8:197-205
Yamamoto K, Matsusue Y, Horita S Nicorandil-induced oral ulceration: report of 3 cases and review of the Japanese literature. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 2011; 112:754-749 https://doi.org/10.1016/j.tripleo.2011.05.031
Mental nerve paraesthesia secondary to nicorandil-induced oral ulceration: a case report Emma Morgan Lee Feinberg Bijaya Rajlawat Anne Field Dental Update 2024 50:1, 707-709.
Authors
EmmaMorgan
Academic Clinical Fellow and Dental Core Trainee, University of Liverpool
Nicorandil, used as a treatment for angina pectoris, continues to be prescribed in the UK. The association between nicorandil and oral ulceration is well documented. Nicorandil-induced oral ulceration characteristically presents as a persistent, large, deep ulcer that can have a great impact on quality of life. A 63-year-old female was referred to the oral medicine department with a non-healing ulcer and associated paraesthesia of the left lower lip. Her drug history included nicorandil 30 mg once daily. A provisional diagnosis was made of nicorandil-induced oral ulceration with associated paraesthesia, secondary to mental nerve involvement. Following liaison with cardiology, and cessation of nicorandil medication, the ulceration healed, and the patient reported improved sensation to the lower lip.
CPD/Clinical Relevance: Nicorandil-induced oral ulceration should be considered in the differential diagnosis of oral ulceration.
Article
Nicorandil was first introduced into the UK in 1994 and continues to be used as a treatment for angina pectoris.1 The yellow card scheme run by the Medicines and Healthcare products Regulatory Agency (MHRA) records information regarding suspected safety concerns or incidents involving medicines or medical devices. Between 1994 and 2020, 230 cases of nicorandil-induced oral stomatitis and ulceration were recorded.2 These data may under-represent the true number of cases as data collection relies on voluntary reporting by health professionals and patients. Despite this, the pathogenesis of nicorandil-induced oral ulceration is still unclear. Ulceration can present at any point while taking nicorandil, with oral ulceration reported less frequently than elsewhere in the gastrointestinal tract.3 Nicorandil-induced oral ulceration has distinctive features: persistent deep, large ulcers with an irregular border.4,5 Such deep ulcers, with associated inflammation and soft tissue swelling, may have the potential to affect underlying structures, including nerves. We present a case of nicorandil-induced oral ulceration, which presented as paraesthesia of the lower lip secondary to mental nerve involvement.
Case report
A 63-year-old female was referred to the department, via a 2-week suspected head and neck cancer pathway, with a non-healing ulcer in the buccal sulcus of the LL4, LL5 region. The ulcer had been present for 5 weeks, during which time it had caused an intermittent throbbing pain, affecting the patient's ability to speak and eat. The patient also described numbness of the lower left lip, which had been present for 2 weeks with no change. There was no history of trauma, previous ulcers or recent surgical intervention.
Her medical history revealed chronic obstructive pulmonary disease, ischaemic heart disease, peripheral vascular disease, previous stroke, underactive thyroid and gastro-oesophageal reflux disease. The patient had previously had an aortic bypass and was taking multiple prescribed medications, including aspirin 75 mg once daily (OD), atorvastatin 80 mg OD, bisoprolol 1.25 mg OD, clopidogrel 75 mg OD, furosemide 40 mg OD, gabapentin 100 mg three times daily, levothyroxine 100 μg OD, mirtazapine 75 mg OD, nicorandil 30 mg OD, perindopril 8 mg OD, ranitidine 150 mg OD, ranolazine 375 μg twie daily, salbutamol inhaler (100 μg/dose, two puffs taken as needed and Relvar Ellipta inhaler (Trelegy 92/55/22 μg, 1 puff every morning). Nicorandil medication was commenced 11 years prior to presentation. She had a 52-year history of smoking and, at the time of presentation, was smoking 20 cigarettes a day.
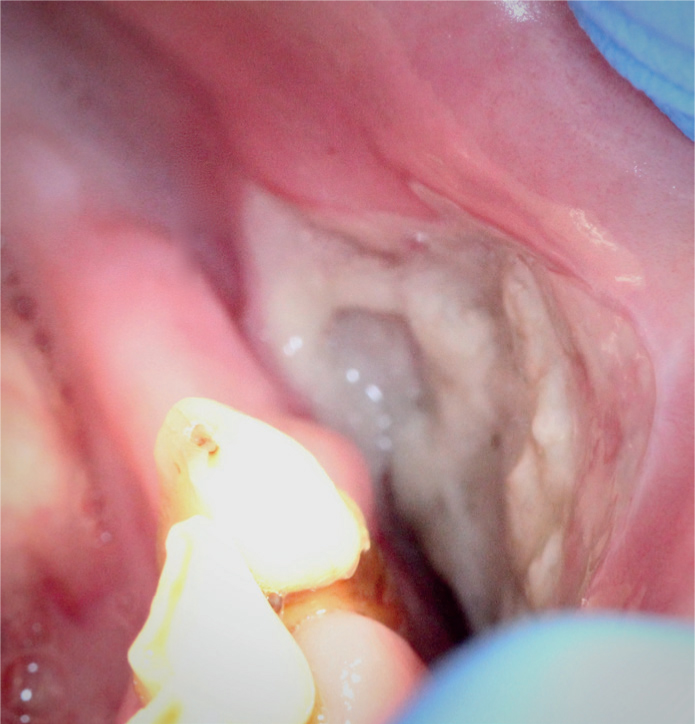
Extra-oral examination revealed no associated lymphadenopathy or facial swelling, and the patient was apyrexial. Using a two-point discrimination test, the mandibular branch of the trigeminal nerve showed a diminished sensation between the lower midline and left commissure. All other cranial nerves were intact. Intra-orally, the remaining dentition on the left side included LL3, LL2 and LL1. A deep ulcerated area, 3 cm in length and 1.5cm in width, with irregular borders and overlying white slough was present in the sulcus area of the left premolar region (Figure 1). The ulcer was extremely tender on palpation, soft, non-indurated, with no contact bleeding. An orthopantomogram was taken that showed a 4 x 2 mm radiolucency on the crest of the ridge in the LL4 region with a radiopaque fragment in the centre, possibly representing a piece of loose bone. There was no evidence of pathology associated with the retained roots in the lower left quadrant. The patient was unable to tolerate an intra-oral radiograph. She had undergone a CT angiogram of the neck 2.5 years earlier for assessment of common carotid stenosis and consideration for stenting on which there was a small radiolucency visible at the crest of the ridge. Given that this area was at the crest of the ridge, asymptomatic and distinct to the ulceration, it was not considered to be related.
Figure 1. Clinical presentation of the ulceration in the LL4, LL5 region on initial presentation.
A provisional, clinical diagnosis of nicorandil-induced oral ulceration was given. The paraesthesia of the lower lip was attributed to secondary mental nerve involvement owing to the depth of the ulcer into the buccal sulcus. An urgent letter was sent to the patient's cardiologist requesting possible discontinuation of the nicorandil. Triamcinolone 2 mg mouthwash (prepared by the hospital pharmacy) and benzydyamine hydrochloride 0.15% mouthwash (Difflam, MEDA, Sweden) was prescribed for initial symptomatic relief. Blood tests including FBC, B12, folate, ESR, U+E, LFT and HbA1C were undertaken and results were within normal limits. A review appointment was made for 10 days' time, with a view to possible biopsy if there was no improvement. Subsequent review was delayed for 6 weeks as the patient was hospitalized with pneumonia.
Within 3 weeks of the initial presentation, nicorandil had been discontinued by her cardiologist, with an increased dose of furosemide (loop diuretic) and ranolazine (sodium channel blocker) as replacements. At the subsequent review 6 weeks later, following cessation of nicorandil treatment, the patient reported improvement; however, the ulcer was still painful and affecting her ability to eat. On examination, the ulcerated area had reduced in size, although the area was still tender on palpation. The diminished sensation over the lower left lip remained the same, with the patient reporting continued numbness. Symptomatic management including triamcinolone 2 mg mouthwash and benzydyamine hydrochloride 0.15% mouthwash was continued. The patient continued regular follow-up appointments during which her symptoms, of both oral discomfort and sensory loss, improved as the ulcer began to heal. Approximately 3 months following the discontinuation of nicorandil, the ulcer had healed (Figure 2). Healing resulted in the formation of dense fibrous tissue in the area, but this was symptom free. The normal sensation of the lip was gradually returning at the 3-month review, but she then requested discharge from the department. This adverse drug reaction was reported through the yellow card reporting system.
Figure 2. Clinical presentation of the healed area on review approximately 3 months later.
Discussion
Nicorandil continues to be used as a second-line treatment for angina pectoris in the UK.1 Common adverse reactions associated with the drug include headaches, dizziness and nausea.6 The precise incidence of nicorandil-induced oral ulceration is unknown; however, evidence from a prescription event monitoring study showed that 0.4% (n=49) of the 13,260 patients followed up had developed mouth ulcers while taking nicorandil.6 The clinical presentation in this case was a persistent large deep ulcer, consistent with previously reported cases.4,5,7 Such ulcers can have great impact on quality of life, demonstrated in this case.7,8
The deep and persistent nature of nicorandil-induced oral ulceration can mimic the appearance of oral squamous cell carcinoma (OSCC). Previous case reports have highlighted OSCC as a differential diagnosis and have suggested distinguishing clinical features between nicorandil-induced oral ulceration and OSCC.5 Nicorandil-induced oral ulceration tends to present as a deep ulcer that is painful from the onset, whereas OSCC commonly present as indurated, exophytic or as red, white or speckled lesions with late-onset pain.5 Resolution of ulceration following cessation of nicorandil varies, and can often be protracted, therefore continued examination and review is essential to ensure adequate healing. Despite cessation of nicorandil eventually leading to resolution of ulceration, symptomatic management should be provided in order to relieve pain. The associated paraesthesia of the lower lip is a previously unreported finding. It is likely to be due to the ulcer affecting superficial branches of the mental nerve. Following cessation of the nicorandil, the ulceration and reduced sensation symptoms improved. Therefore, the paraesthesia was considered to be secondary to involvement of the mental nerve branches in the ulcerative and associated inflammatory process. Previous evidence regarding mental nerve neuropathy identifies invasive dental procedures, inflammatory apical pathology and malignant lesions as aetiological factors.9
Conclusion
In conclusion, the ulcer's clinical appearance in this case correlates with that of previous studies. The secondary mental nerve involvement was an unreported and unusual finding, which adds to the available body of evidence. This case highlights the importance of a knowledge of local anatomy, in order to contextualize the history and clinical findings. It also highlights the clinician's role in reporting adverse drug reactions to the MHRA via the yellow card scheme.1