Mustafa B. Using 3D animation and virtual reality in educations. Technium Soc Sci J. 2022; 27:269-289
Alcañiz M, Bigné E, Guixeres J. Virtual reality in marketing: a framework, review, and research agenda. Front Psychol. 2019; 10 https://doi.org/10.3389/fpsyg.2019.01530
Soltani P, Andrade R. The Influence of virtual reality head-mounted displays on balance outcomes and training paradigms: a systematic review. Front Sports Act Living. 2021; 2 https://doi.org/10.3389/fspor.2020.531535
Hung YC, Montazem A, Costello MA. The correlation between mandible fractures and loss of consciousness. J Oral Maxillofac Surg. 2004; 62:938-942 https://doi.org/10.1016/j.joms.2004.01.018
Giddins G, Giddins H. Wrist and hand postures when falling and description of the upper limb falling reflex. Injury. 2021; 52:869-876 https://doi.org/10.1016/j.injury.2020.11.056
Virtual reality (VR) is a computer-generated three-dimensional simulation, often used with a wireless headset and controllers. It provides the user with visual, auditory and tactile stimuli for an immersive experience. Popularity of VR devices has snowballed, with use in domestic, education, healthcare and business sectors. We present a patient who jumped off a plank into water in a virtual reality world, while in reality, the patient had jumped into their TV unit, striking their chin. This resulted in a displaced and mobile fracture of the mandibular parasymphysis that required reduction and fixation under a general anaesthetic. This novel technology is altering our world's interface in multiple fields, but there are potential risks associated with fully immersing ourselves in another world.
CPD/Clinical Relevance: It is important to be aware of trauma that can result from injuries during virtual reality headset use.
Article
Virtual reality (VR) is the creation of an immersive three-dimensional environment with the use of a computer, now frequently contained within a wireless headset and controllers. It provides the user with visual, auditory and tactile stimuli.1 Increasing affordability of VR devices for domestic use, as well as increasing recognition in the education, healthcare and business sectors, has resulted in a snowballing market.2,3 In 2016–2018, approximately 170 million active users of VR headsets were registered worldwide.1 In 2021, there were 0.81 billion augmented reality users, and by the end of 2023, this number is predicted to grow to 1.4 billion.4,5 We present the case of a patient who presented with a mandible fracture sustained while playing a VR game at home. A review of the literature identified two case reports of head and neck injuries sustained during VR gaming; however, this is the first known report of a maxillofacial bony injury that occurred with use of this novel technology.5,6
Case report
A 59-year-old female attended the emergency department with a facial injury. The injury had occurred following a mechanical fall while using a VR headset in a family member's home. The patient had been playing a VR game in which she was ‘walking the plank’ off a ship overlying the sea. The patient found the experience immersive and very realistic, and in fear, jumped off the plank, which led to the visual stimulus of her free-falling towards the water. In reality, the patient had physically jumped, resulting in an unbraced, low impact fall, hitting her chin against an adjacent television cabinet.
With symptoms of mandibular pain, altered occlusion and gingival bleeding, the patient attended the emergency department. On presentation, it was confirmed the patient had not experienced any loss of consciousness nor were there any concerns regarding a head injury. On clinical examination, the patient did not have cervical spine tenderness or limited neck movement and was neurologically intact. Oedema and contusion of the skin overlying the right parasymphysis was evident. The patient had a deranged occlusion with an occlusal step and diastema in the region of the right mandibular lateral incisor and canine. A gingival tear overlaid the fracture, and the saliva was blood-stained. No other traumatic injuries were identified.
The patient had no significant past medical history. Alcohol and recreational drugs were not a factor in this injury.
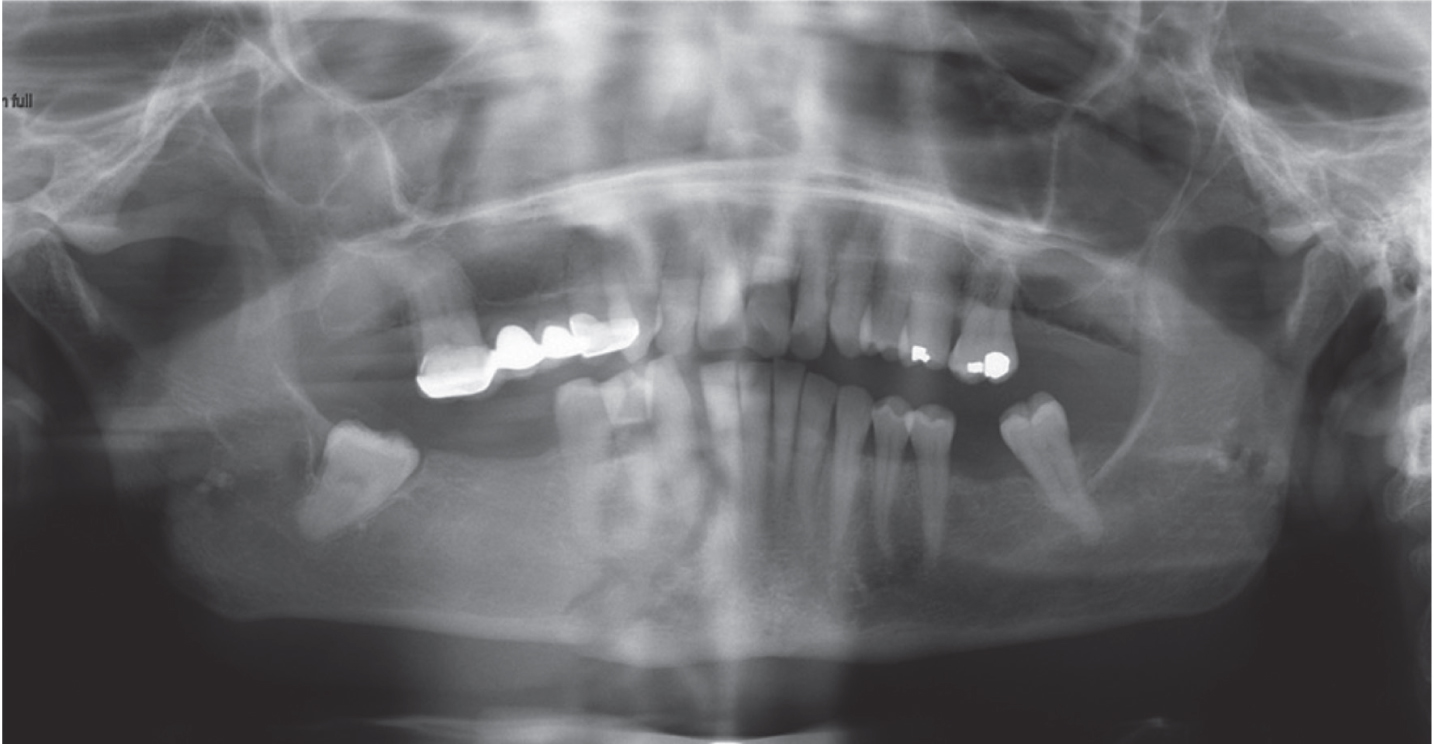
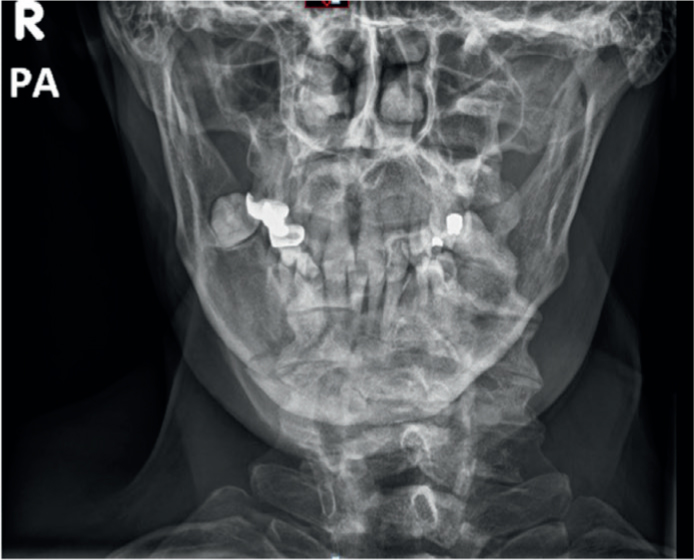
Radiographic investigations requested included an orthopantomogram (OPG) and posteroanterior (PA) mandible, which demonstrated a displaced fracture of the right mandibular parasymphysis (Figures 1 and 2).
Figure 1. Orthopantomogram (OPG) showing the right mandibular parasymphyseal fracture and altered occlusion.Figure 2. Postero-anterior (PA) mandible radiograph showing the displaced right mandibular parasymphyseal fracture.
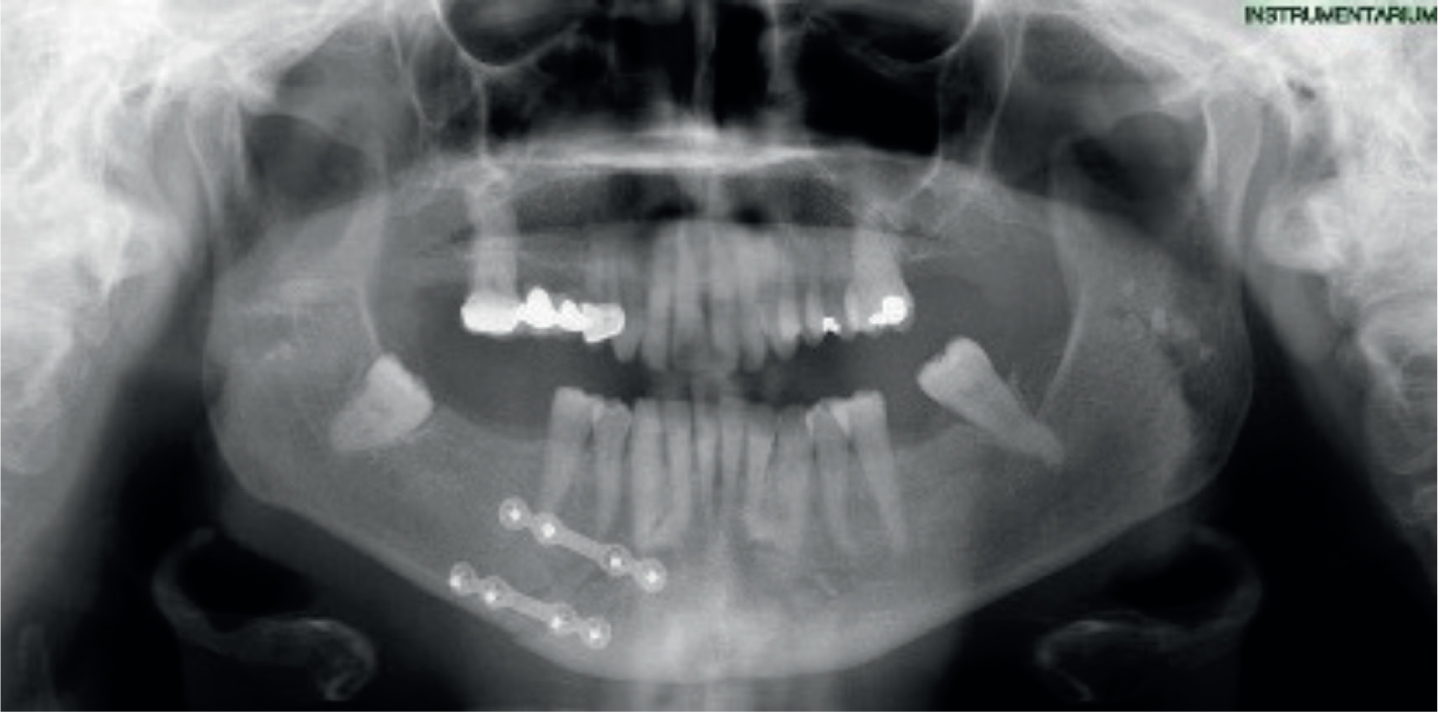
The patient was admitted under the care of the oral and maxillofacial surgery (OMFS) team, and the fracture was reduced with a bridle wire under local anaesthetic, while waiting for the operation. Bridle wiring involves passing a wire through the interproximal spaces of the teeth on either side of the fracture to stabilize and support the segments. This reduces movement of the fracture and thus, discomfort, for the patient, to help maintain oral intake and enable more comfortable speech.7 During admission, the patient received intravenous benzylpenicillin and metronidazole for their open fracture, chlorhexidine mouthwash to reduce the risk of secondary infection and analgesia. Open reduction and internal fixation (ORIF) was the surgical method used to repair the fracture, and it was carried out under a general anaesthetic the following day after admission. The patient was manually held in occlusion and the fracture reduced. Two 4-hole 4-mm spaced mini-plates were placed perpendicularly across the fracture line, with one approximately below the apices of the tooth roots, and the second at the lower border of mandible. The plates were secured with eight 5-mm screws. Occlusion was checked and stability confirmed. The sulcular incision was approximated and sutured with 4/0 synthetic resorbable material. Post-operative imaging was taken the following day (Figure 3), before the patient was discharged home. Routine follow-up was arranged at the patient's local OMFS unit.
Figure 3. Post-operative OPG demonstrating two spaced mini-plates for fixation of right parasymphysis fracture.
Findings from literature
A literature search for head and neck injuries with involvement of VR headsets was undertaken using Pubmed, Google Scholar and Google search engine. Only two relevant case reports were identified, neither of which included facial fractures.
Case report 1
The first report described a likely stress fracture of the 7th cervical vertebra following frequent VR gaming.1 The 31-year-old male had no prior history of injuries or deformities to his spine, and bone density was normal. The patient described in this case played VR games 1–4 hours almost daily for multiple months. It was thought that rapid movements during VR gaming can lead to repetitive strain to the cervical spine, and given the intensive hours playing in VR, this was deemed to be the most likely cause of injury.1 It is yet to be determined whether this is an isolated incident from unknown pre-existing factors, or whether the mechanism alone can lead to this vertebral trauma.
Case report 2
The second case of a VR-related trauma described a 57-year-old male ‘free-falling in an open void’ while using a VR headset, who experienced an unbraced, low-impact fall against a banister.6 This patient recalled standing with the VR headset on, during a forward free-falling scene. Owing to the visual and auditory stimuli of the open void, it was reported by observing family that he lost balance and did not move his hands into a protective position, resulting in the impact of his forehead against a banister. This patient sustained a loss of consciousness lasting 5 minutes, which resolved spontaneously. On presentation to hospital, it was reported that he attended with head and neck pain, paraesthesia of his upper limbs, confusion and disorientation. Examination and investigations revealed multiple neural and vascular injuries and a traumatic brain injury. Specific injuries were noted as frontal soft tissue lacerations, a spinal cord injury, hypoglossal nerve injury causing dysarthria and dysphagia, vertebral artery dissection and a traumatic brain injury. Treatment received by this patient included a neck brace, anti-platelet therapy, and multidisciplinary team neurological rehabilitation involving spinal physiotherapy, speech and language therapy and neuropsychology6.
Discussion
It is thought that postural safety reflexes were not triggered as the visual input from the VR headset overrode vestibular or postural input6. The vestibular system includes the inner ear and areas of brain that are affected by movement and is a key component of postural reflexes. Vestibular input is the sensation of change in position, direction or movement of the head. Vestibular information contributes to the development of muscle tone, righting reactions, balance, postural security, eye movements and overall alertness8, 9. If these inputs for the vestibular system are overridden, it could represent significant relevance to the risks of falls and associated trauma.
Conflicts between proprioceptive and vestibular sensory systems when there is the illusion of body movement, for example riding a VR rollercoaster, may result in a loss of balance and an affected ability to regain stability after balance loss. Therefore, patients may be more likely to fall in VR scenarios involving movement such as flying or jumping and would likely not have the appropriate reflex responses if the physical surroundings contained hazards not visible in the virtual world.10 However, there is also increasing research into use of VR headsets for assessment of falls risk in elderly as well as for treatment of fear of falling by aiding in the training of functional balance in safe environments.10
A retrospective service review in 2019 analysed patients sustaining maxillofacial fractures following simple falls. This review found that fractures of other parts of the body were significantly more common in falls without loss of consciousness than in falls with loss of consciousness. A reason for additional bodily fractures is likely related to initiation of reflexes associated with falling, for example the upper limb falling reflex.11,12 It was also found that patients whose falls occurred with a loss of consciousness sustained more severe maxillofacial fractures than those without.11
Relating this to the anecdotal evidence from the studies described above, the three VR cases describe injuries to the head and neck without additional bodily injuries. This highlights a potential comparison between falling in VR worlds and falling with a loss of or reduction in consciousness level, such as in a vasovagal syncope.
As VR headsets become increasingly popular for general consumers, injuries sustained during use may present to our departments more frequently. Manufacturer health and safety warnings currently advise use of VR devices in safe environments, specifically that trip hazards are cleared, and warn of the risk of loss of balance6. There are also additional optional settings with some manufacturers including portraying the outlines of surrounding objects in the VR visual field. It is not currently known whether the warnings are commonly referred to, or if the average user considers the risks associated prior to use6.
Conclusion
With a burgeoning demand for VR experience, the metaverse seems likely to become a reality and we suspect there will be an increase in patients presenting with trauma secondary to use of VR headsets. It is important to complete a full head and neck examination in patients that attend with facial injuries sustained following low-impact falls whilst using a VR headset, as they may present with more severe injuries than anticipated due to an override of protective reflexes.