Conte M, Lombardi P, Linfant J. A supernumerary tooth fused to the distal surface of a mandibular third molar. J N J Dent Assoc. 2002; 73:8-9
Littner MM, Gordon M, Engelberg ME, Kaffe I. Fusion of a supernumerary tooth to third mandibular molar. Refuat Hashinayim. 1984; 2:16-18
Morris DO. Fusion of mandibular third and supernumerary fourth molars. Dent Update. 1992; 19:177-178
Chi AC, Neville BW, Damm DD, Allen C. Oral and Maxillofacial Pathology.: Elsevier Health Sciences; 2017
Ruprecht A, Batniji S, el-Neweihi E. Double teeth: the incidence of gemination and fusion. J Pedod. 1985; 9:332-337
Gera N, Tripathi S, Naik NS, Astekar M. Triplication in permanent teeth: a rare case report. J Oral Maxillofac Pathol. 2017; 21:145-148 https://doi.org/10.4103/jomfp.JOMFP_155_16
Labanca M, Azzola F, Vinci R, Rodella LF. Piezoelectric surgery: twenty years of use. Br J Oral Maxillofac Surg. 2008; 46:265-269 https://doi.org/10.1016/j.bjoms.2007.12.007
Abella F, de Ribot J, Doria G Applications of piezoelectric surgery in endodontic surgery: a literature review. J Endod. 2014; 40:325-332 https://doi.org/10.1016/j.joen.2013.11.014
Bhati B, Kukreja P, Kumar S Piezosurgery versus rotatory osteotomy in mandibular impacted third molar extraction. Ann Maxillofac Surg. 2017; 7:5-10 https://doi.org/10.4103/ams.ams_38_16
Sivolella S, Berengo M, Bressan E Osteotomy for lower third molar germectomy: randomized prospective crossover clinical study comparing piezosurgery and conventional rotatory osteotomy. J Oral Maxillofac Surg. 2011; 69:e15-23 https://doi.org/10.1016/j.joms.2010.12.036
Fusion of an Impacted Third and Supernumerary Fourth Molar Tooth with Concrescence of the Second Molar Julian Leow Kohmal Solanki Mahesh Kumar Dental Update 2024 50:9, 707-709.
Authors
JulianLeow
BDS, MFDS RCPS (Glasg), PGCert (MedEd)
Oral and Maxillofacial Surgery Senior House Officer
We report the case of a symptomatic 41-year-old female presenting with fusion of an impacted third (LL8) and fourth (LL9) mandibular molar tooth with concrescence of the second molar tooth (LL7). Cone-beam computed tomography showed direct contact with the inferior dental nerve (IDN) and lingual aspect of the double tooth. The patient underwent surgical removal of the LL8–LL9 using piezoelectric surgery. We present the first case of successfully using pre-operative CBCT in the planning of surgery and piezoelectric surgery to separate an impacted fused LL8–LL9 from a concrescent LL7 without causing trauma to the LL7 or intimately positioned IDN.
CPD/Clinical Relevance: An impacted fused mandibular third and supernumerary fourth molar with concrescence of the second molar requires very careful management.
Article
There are numerous developmental abnormalities in the shape of teeth. Connate or double teeth with dentine and/or pulp union may either be a result of the conjoining of two adjacent tooth buds, usually with two separate root canal systems (fusion) or the partial division of a single tooth bud into two, usually with a single root canal (gemination). Concrescence is the joining of two teeth by cementum only, with non-contiguous dentine. Whereas fusion and gemination are congenital abnormalities, concrescence may either occur at the developmental stage or as a post-eruption abnormality caused by inflammation.
We report the case of a symptomatic 41-year-old female presenting with fusion of an impacted third and fourth mandibular molar tooth with concrescence of the distal root of the second molar tooth (LL7). Although fusion of mandibular third (LL8) and fourth molar (LL9) teeth has been previously reported in the literature,1,2,3 to the best of our knowledge, this is the first report of a fused third and fourth molar, complicated not only by concrescence to the distal root of the second molar, but also by impaction and direct relation to the left inferior dental nerve (IDN). We share our experience of pre-operative cone beam computed tomography (CBCT) to aid surgical treatment planning as well as the novel use of piezoelectric surgery to divide the concrescent distal root of the LL7 from the mesial aspect of the double tooth.
Case report
A 41 year old female was referred to the oral and maxillofacial surgery clinic with a history of pain on the left hand side of her jaw that had recently caused an episode of left facial swelling. The patient had also noted discharge intra-orally in the lower left quadrant. Her past medical history was unremarkable. She did not smoke or drink alcohol and worked as a software engineer.
Clinical examination revealed what was thought to be a partially erupted lower left wisdom tooth, with some tenderness, bleeding and granulation tissue suggestive of an ongoing infective process.
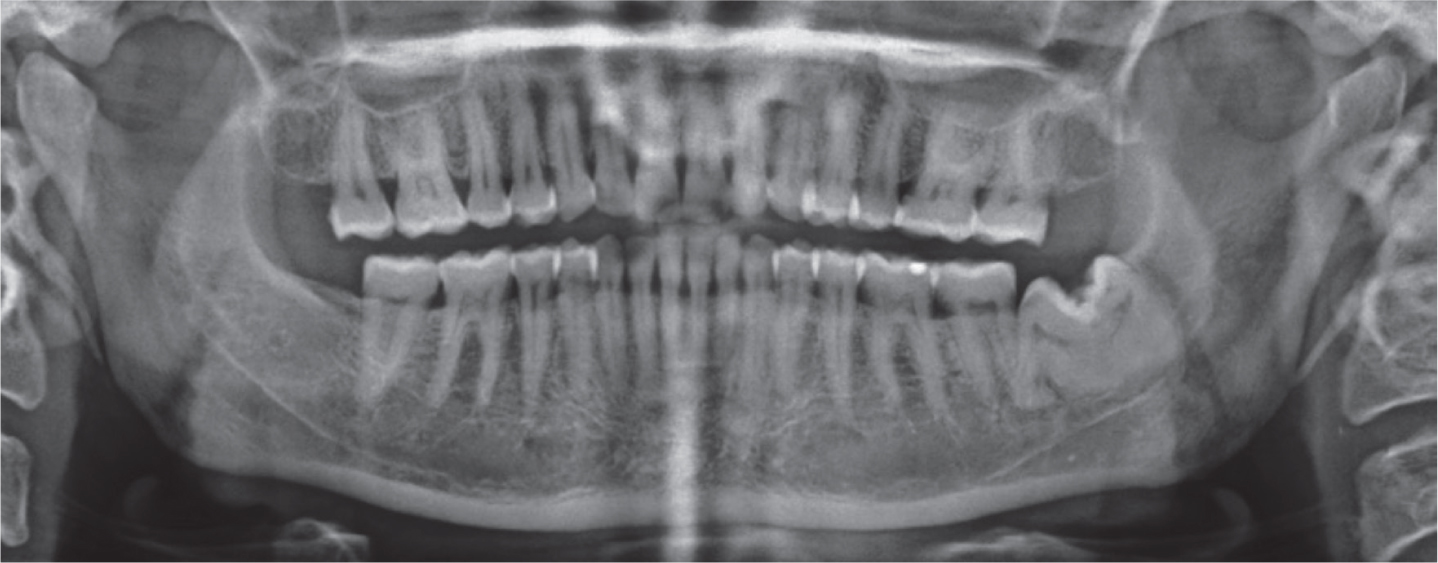
A panoramic radiograph (Figure 1) revealed an impacted lower left third molar tooth (LL8) with apparent fusion to a retromolar supernumerary tooth (LL9). Furthermore, the mesial root of the fused teeth appeared fused by cementum to the distal root of the lower left second molar tooth (LL7). The distal root of the LL9 appeared to overlap with the left IDN. There was no associated peri-apical pathology. The other third molars (LR8, UL8 and UR8) were congenitally absent. The remaining dentition was fully present and normally erupted, and the supporting alveolar bone appeared normal.
Figure 1. Pre-operative panoramic radiograph of the entire dental arch.
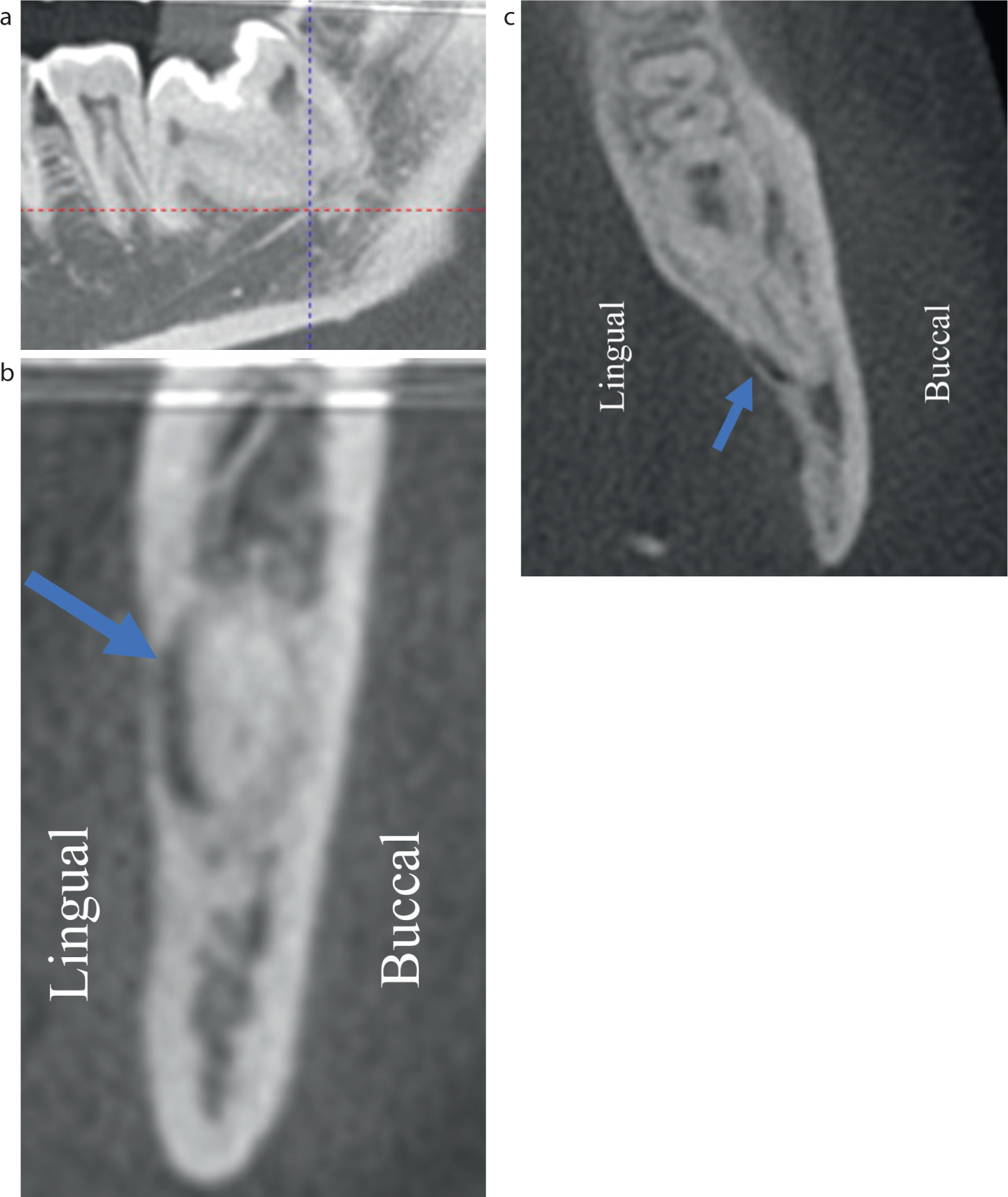
To aid in better determining the morphology of the double tooth and its relationship to both the LL7 and IDN, a CBCT was performed (Figure 2). This showed that the large distal root of the LL8 was fused with the body of the root system of the supernumerary LL9. The pulp chamber extended down the distal root as a wide root canal. The LL9 had a conical root system containing two fused roots. The left IDN passed lingually, making direct contact with the mid third of the LL9 root, and with the apical third of the LL8. The mesial root of the double tooth appeared conventional, but was fused by concrescence to the distal root of the LL7.
Figure 2. Cone beam computed tomogram of the lower left mandible. (a) Sagittal view through the LL8–LL9 double tooth showing fusion to LL7 by cementum only and close relationship to the left ID canal. (b) Coronal view showing the lingual location of the left ID canal (blue arrow). (c) Axial view showing the lingual location of the left IDN and thinning of the lingual cortex (blue arrow). Images not to scale and shown for illustrative purposes.
Surgical options of either coronectomy or complete extraction of the LL8/LL9 were offered to the patient, with the final decision to be made intra-operatively. The patient was made aware of the risk of damage to the left ID and lingual nerves with potential permanent numbness in the chin, lower lip and tongue regions with either option, although reduced with a coronectomy. In addition, the potential risk of damage to the LL7, with a potential need for future root canal therapy or extraction was also explained. The patient was listed for surgical removal or coronectomy of the LL8–LL9 under general anaesthetic, with a view to separating the concrescent LL7 from the LL8–LL9 using piezoelectric surgery to minimize the risk of damage to the LL7 distal root.
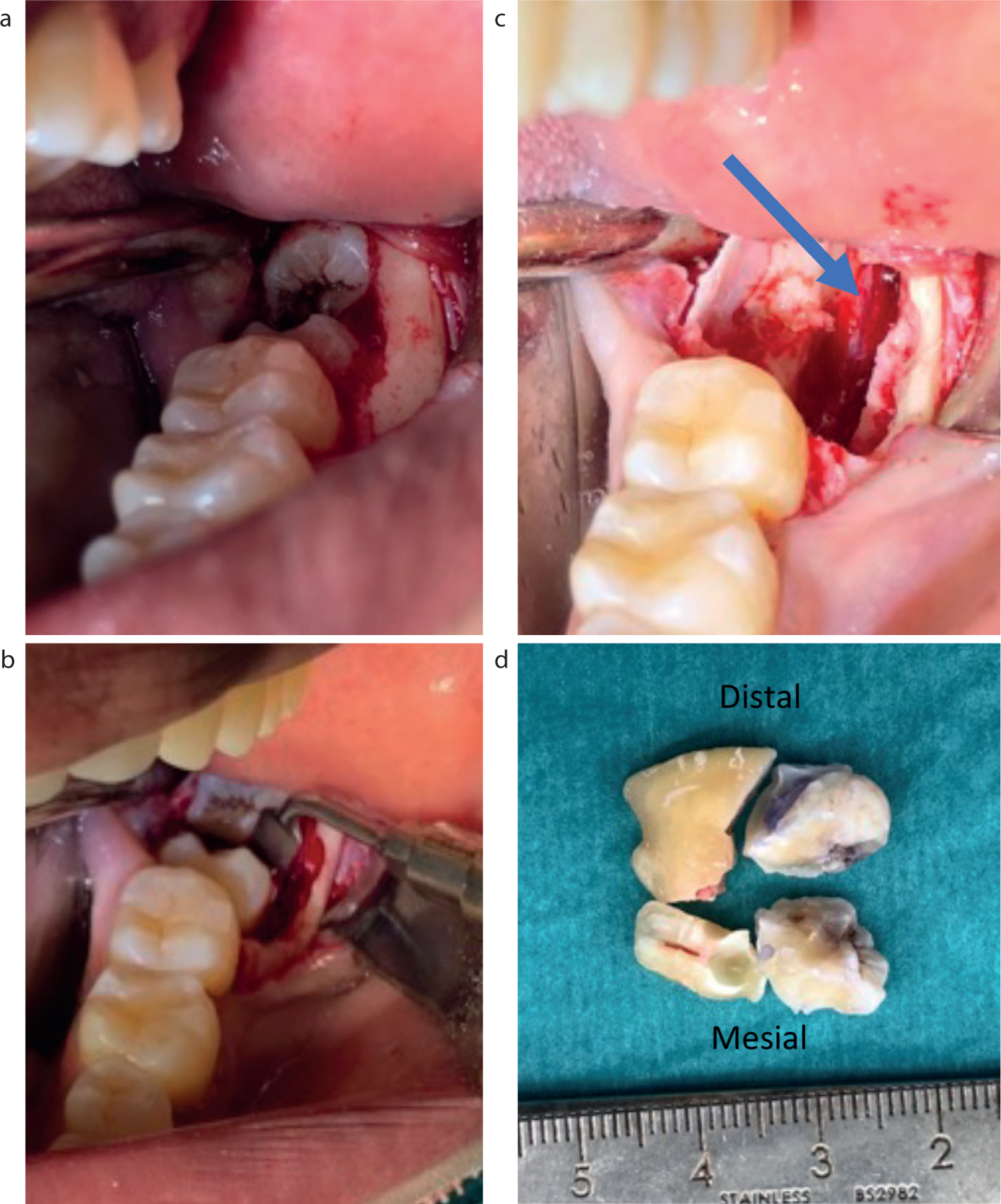
For long-acting post-operative pain relief and decreased use of post-operative opioids, 15 ml bupivacaine 0.5% in 1:200,000 adrenaline was administered as a left IDN block and locally infiltrated buccally. A full-thickness mucoperiosteal flap was raised and bone removal performed using a tungsten carbide fissure bur to expose the tooth (Figure 3a). A piezosurgery handpiece with cutting saw tip (DePuy Synthes, Raynham, MA, USA) was used to section the distal root of the LL7 from the mesial root of the LL8. A fissure bur and piezoelectric saw was used to section and decoronate the LL8–LL9 (Figure 3b). Owing to the mobility of the LL8–LL9 roots, it was decided that it would be possible to gently elevate the LL8 and LL9 roots separately and minimize trauma to the lingually placed left ID canal. The left ID canal was visualized and was intact (Figure 3c). Absorbable gelatin sponge (Surgifoam, Ethicon Inc, Somerville, NJ, USA) was used to pack the cavity and provide haemostasis. Mucosal closure was performed with 3-0 vicryl rapide (Ethicon Inc, Somerville, NJ, SA). The patient was discharged with oral amoxicillin for 1 week.
Figure 3. Intra-operative clinical photographs. (a) Full thickness mucoperiosteal flap raised and LL8–LL9 double tooth shown. (b) Piezoelectric saw used after fissure bur to section tooth when in close proximity to IDN. (c) Left IDN visualized and intact (blue arrow). (d) Sectioned LL8–LL9 double tooth post-extraction.
The patient was reviewed 2 weeks post-operatively. The patient was pain free, and clinically the intra-oral operative site was healing well, with no evidence of infection. There was also no numbness or paraesthesia of the lower lip, chin or tongue. She was thus discharged back to the care of her general dental practitioner.
Discussion
The management of symptomatic impacted mandibular wisdom teeth can be challenging. We report the novel use of pre-operative CBCT and intra-operative piezosurgery to treat a very rare case of an impacted fused mandibular third and fourth molar with concrescence of the second molar and in direct contact with a lingually placed left ID canal.
Fusion and gemination are rare developmental anomalies that most frequently occur in the anterior and maxillary regions.4 Studies have shown an incidence in the primary dentition of 0.5–2.5% and 0.3–0.5% in the permanent dentition.5 Differentiating between fusion and gemination can be clinically and radiographically difficult. It has been proposed that fusion should be defined as a double tooth where the tooth count reveals a missing tooth when the abnormal tooth is counted as one, whereas in gemination the tooth count is normal.4 However, this definition is complicated somewhat when the conjoined tooth involves a supernumerary. Triple teeth are an even rarer phenomenon, nearly always occurring in the primary dentition. We were able to find only a single report of triplication in the permanent dentition.6 Although our case is not a ‘true’ triple tooth with dentine union across all three teeth, a fused permanent double molar tooth (including a supernumerary LL9) and concrescence of another molar tooth in the mandible is, as far as we know, unreported.
CBCT permits the three-dimensional planning of surgery to assess tooth morphology and neurovascular relationships, at the cost of increased radiation exposure, time and expense. As opposed to panoramic radiography alone, we were able to assess the lingual relationship of the ID canal with respect to the LL8–LL9 roots and thus better inform our intra-operative approach. In our case, CBCT was also able to confirm the diagnoses of fusion and concrescence, and thus permit the option of preserving the LL7 distal root.
Piezoelectric surgery was introduced, initially for oral and maxillofacial surgery, over 20 years ago and provided an alternative to mechanical rotary instruments in cutting bone atraumatically with respect to the surrounding soft tissues.7 It uses piezoelectric vibrations to cut mineralized tissue, without cutting neurovascular tissue or other soft tissues. Although initially used for osteotomies, piezosurgery has also found success with dental hard tissues in endodontic surgery, being used in root end resection and preparation.8 Piezosurgery is also routinely used in the operative management of impacted third molars; however, it is usually used to perform the osteotomy rather than tooth sectioning.9,10 In our patient, in comparison to a conventional rotary instrument, the novel use of piezosurgery permitted precise sectioning of the LL7 from the LL8–LL9, while reducing the risk of damage to the LL7 distal root and the ID and lingual nerves.
In summary we present the only known case of an impacted fused mandibular third and supernumerary fourth molar in direct contact lingually with the ID canal with concrescence of the second molar. Our case report demonstrates how pre-operative CBCT and the novel use of piezosurgery can be used to surgically treat symptomatic complex dental hard tissue development anomalies with a satisfactory outcome.
Conclusion
In summary we present the only known case of an impacted fused mandibular third and supernumerary fourth molar in direct contact lingually with the ID canal with concrescence of the second molar. Our case report demonstrates how preoperative CBCT and the use of piezosurgery can be used to surgically treat symptomatic complex dental hard tissue development anomalies with a satisfactory outcome.