McArdle L The prevention and management of distal cervical caries of the mandibular second molar. Dent Update. 2019; 46:406-410
Knutsson K, Brehmer B, Lysell L, Rohlin M Pathoses associated with mandibular third molars subjected to removal. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 1996; 82:10-17 https://doi.org/10.1016/s1079-2104(96)80371-4
Allen RT, Witherow H, Collyer J The mesioangular third molar – to extract or not to extract? Analysis of 776 consecutive third molars. Br Dent J. 2009; 206 https://doi.org/10.1038/sj.bdj.2009.517
Toedtling V, Coulthard P, Thackray G Distal caries of the second molar in the presence of a mandibular third molar-a prevention protocol. Br Dent J. 2016; 221:297-302 https://doi.org/10.1038/sj.bdj.2016.677
McArdle LW, McDonald F, Jones J Distal cervical caries in the mandibular second molar: an indication for the prophylactic removal of third molar teeth? Update. Br J Oral Maxillofac Surg. 2014; 52:185-189 https://doi.org/10.1016/j.bjoms.2013.11.007
Broadbent JM, Thomson WM For debate: problems with the DMF index pertinent to dental caries data analysis. Community Dent Oral Epidemiol. 2005; 33:400-409 https://doi.org/10.1111/j.1600-0528.2005.00259.x
Juodzbalys G, Daugela P Mandibular third molar impaction: review of literature and a proposal of a classification. J Oral Maxillofac Res. 2013; 4 https://doi.org/10.5037/jomr.2013.4201
Yilmaz S, Adisen MZ, Misirlioglu M, Yorubulut S Assessment of third molar impaction pattern and associated clinical symptoms in a central Anatolian Turkish Population. Med Princ Pract. 2016; 25 https://doi.org/10.1159/000442416
Kumar S, Al-Hobeira H, Shaikh S Distribution of impacted third molars based on gender and patterns of angulation in dental students of the Hai'l Region, Saudi Arabia: a panoramic radiographic (OPG) study. Int J Contemp Med Res. 2017; 4:1829-1832
Ferraro M, Vieira AR Explaining gender differences in caries: a multifactorial approach to a multifactorial disease. Int J Dent. 2010; 2010 https://doi.org/10.1155/2010/649643
Lukacs JR, Largaespada LL Explaining sex differences in dental caries prevalence: saliva, hormones, and ‘life-history’ etiologies. Am J Hum Biol. 2006; 18 https://doi.org/10.1002/ajhb.20530
Third molars: not so NICE? risk factors for distal caries in mandibular second molars Amir Treifi Jessica Cooper Julian Yates Dental Update 2024 50:2, 707-709.
Authors
AmirTreifi
BDS, MFDS RCPS(Glasg)
Dental Core Trainee in Oral Surgery, University Dental Hospital of Manchester
UK guidelines currently advise against the prophylactic removal of mandibular third molars. However, growing evidence shows that asymptomatic impacted mandibular third molars may contribute to the formation of distal caries in mandibular second molars. Patients should be made aware that these guidelines do not necessarily prevent the potential development of decay or loss of mandibular second molars. A retrospective review, over 6 months, analysed the incidence and evaluated the risk for developing caries on the distal aspect of mandibular second molars, in patients referred for assessment of impacted third molars. Distal caries in the mandibular second molar was present in 24.1% of cases. Of these patients, 9% demonstrated caries bilaterally. In those who developed distal caries in the mandibular second molar, 76% of adjacent third molars demonstrated mesio-angular impaction, 91% of third molars were partially erupted, and 95% of third molars were either touching or in close proximity to the ACJ of the second molar tooth. The prophylactic removal or coronectomy of mesio-angluar or horizontally impacted third molars that are partially erupted and closely related to the ACJ of mandibular second molars may result in improved long-term patient outcomes.
CPD/Clinical Relevance: The prophylactic removal or coronectomy of certain third molars may result in improved long-term patient outcomes.
Article
In 2000, the National Institute for Health and Clinical Excellence (NICE) first introduced their guidance on the extraction of mandibular third molar teeth.1 This guidance states that the removal of these teeth should be limited to those displaying certain symptoms, thus discouraging the prophylactic removal of pathology-free third molars. This guidance still stands over 20 years later.
Partially erupted and impacted mandibular third molar teeth present a challenging environment for oral hygiene; most notably with mesio-angular impaction against the amelocemental junction (ACJ) of the adjacent second molar. There is growing evidence to suggest that this increases the risk of caries development on the distal aspect of the mandibular second molar.2,3,4,5 This risk is heightened by several factors, including the angulation of impaction and the proximity to the ACJ of the second molar.6 Furthermore, there is evidence to suggest that patients with a low risk of developing caries are still susceptible to the development of distal caries in mandibular second molar teeth.2 Once present, the management of these carious lesions is often challenging because effective caries removal and restoration of the tooth is regularly impeded by the adjacent impacted third molar. Furthermore, as these lesions are often diagnosed at a late stage, and restoration is not always possible, patients are often subjected to extraction of the carious second molar, frequently alongside the removal of the impacted third molar. This then leads to the patient undergoing the removal of two, or potentially four teeth, if the decay has occurred bilaterally.
A better understanding of the risk factors involved in the development of distal caries in mandibular second molar teeth would allow for patients to be more informed, ensuring that they are aware of the long-term prognoses of both the third and second molar teeth. If identified early enough, this would prevent the development of distal caries in the second molar tooth and could avoid the need for the unnecessary extraction of multiple teeth, resulting in the planned extraction of the third molar only. This would ultimately result in improved treatment and long-term outcomes for the patient. Additionally, this could reduce the risk of pain, swelling and infection commonly seen with grossly carious teeth.
This article assesses the incidence of, and evaluates the clinical factors that increase the risk of distal caries development in mandibular second molar teeth.
Assessment
Clinical records of patients referred to the University Dental Hospital of Manchester for assessment of their mandibular third molar teeth were reviewed. Patients without an adjacent second molar tooth were discounted from the study. Data were collected retrospectively over 6 months (January-June 2019).
Data collection included:
Age;
Sex;
Reason for referral;
Treatment performed;
Decayed, missing or filled (DMF) score;
Angulation of the mandibular third molar;
Eruption status of the mandibular third molar;
Proximity of the mandibular third molar to the ACJ of the mandibular second molar.
DMF scoring is a well-established method of assessing a patient's caries risk and allows quantification of the number of decayed, missing or filled teeth.7 In this study, the DMF score was used as an indication for general dental health, and is a validated method for this purpose. The score was calculated via assessment of the patients’ radiographs. We excluded the score of a mandibular second molar if distal caries was the only lesion present on the tooth.
Angulation of the mandibular third molar was calculated using Winter's classification. This widely used classification assesses the inclination of an impacted third molar tooth in relation to the long axis of the second molar.8 Third molar teeth are considered impacted horizontally if the inclination angle is between 80° and 100°, mesio-angular impacted if the inclination angle is between 11° and 79°, vertically impacted if the inclination angle is between 10° and -10° and disto-angular impacted with an inclination angle between -11 and -80°.9 Radiograph viewing software was used to measure the intersecting angle between the long axis of the third and second molar teeth.
Treatment options were delivered to patients based on current NICE guidance. Patients meeting the criteria for treatment were given the following treatment options, if relevant to their presentation:
Leave and monitor;
Extraction of the mandibular third molar tooth;
Coronectomy of the mandibular third molar tooth;
Extraction of the mandibular second molar tooth (if extensive caries evident);
Extraction of the maxillary third molar tooth.
The statistical analysis performed in this article is with a confidence interval of 95% and deemed significant if a P value of <0.05 was obtained. Normality of the data was assessed with the Kolmogorov-Smirnov test. The results of this test determined the data was not normally distributed, therefore, appropriate non-parametric tests were undertaken.
Reason for referral
Percentage (number)
Pericoronitis
44% (99)
Pain
12% (27)
Caries
30% (68)
Peri-apical pathology
5% (12)
Periodontal disease
3% (5)
Assessment/impaction
6% (13)
Ethical approval was not needed as the data was retrospectively and anonymously collected. An ethical approval on-line tool was used to determine this outcome (http://www.hra-decisiontools.org.uk/ethics/).
Findings
In total, 224 patients were included in this study, resulting in the assessment of 278 mandibular third molar teeth. Of these 224 patients, 72 were male and 152 were female. The age of patients ranged from 16 to 64 years (median, 29 years). The age range for all male patients was 16-64 years (median 31 years) and for all female patients was 17-63 years (median 29 years). Statistical evaluation of the ages revealed no significant difference between males and female patients (Mann-Whitney U-test: P>0.05).
A lack of full mouth radiographs only allowed for an accurate calculation of a DMF score in 50 (22%) of patients, which averaged at 5.1.
The reasons for patient referral to secondary care consisted of pericoronitis, pain, caries, peri-apical pathology, periodontal disease and for the assessment of impaction (Table 1). The most common reason for referral was pericoronitis.
Treatment recommended to the GDP, or completed within secondary care, included extraction of the mandibular third molar, coronectomy of the mandibular third molar, extraction of the mandibular second molar, extraction of the maxillary third molar or leave and monitor (Table 2). Of the 224 patients, 5% (n=10) underwent the extraction of both the mandibular second and third molar teeth.
Angulation of impaction, eruption status and proximity to the ACJ of the 278 mandibular third molar teeth assessed can be seen in Table 3. The majority of teeth were either found to be mesio-angularly impacted (46%), partially erupted (77%) or at the ACJ of the adjacent second molar (56%).
Treatment undertaken
Percentage (number)
Extraction mandibular third molar
58% (203)
Extraction mandibular second molar
6% (21)
Leave and monitor
10% (35)
Extraction maxillary third molar
23% (82)
Coronectomy mandibular third molar
3% (12)
Molar status
Percentage (number)
Angulation
Mesio-angular
46% (128)
Disto-angular
21% (59)
Vertical
22% (61)
Horizontal
11% (30)
Eruption status
Partially erupted
77% (215)
Fully erupted
22% (61)
Unerupted
0.7% (2)
Proximity to the ACJ
Contact at the ACJ
56% (156)
Close to the ACJ
19% (53)
Not in contact with ACJ
25% (69)
Molar status
Percentage (number)
Angulation
Mesio-angular
76% (51)
Disto-angular
7% (5)
Vertical
7% (5)
Horizontal
9% (6)
Eruption status
Partially erupted
91% (61)
Fully erupted
9% (6)
Proximity to the ACJ
Contact at the ACJ
81% (54)
Close to the ACJ
13% (9)
Not in contact with ACJ
6% (4)
Distal caries in the mandibular second molar was present in 24.1% (n=67) of cases. The age range of these patients was between 22 and 62 years (median 29 years). The median age of male patients with distal caries in the mandibular second molar was 32 years while in female patients it was 27 years, and this was significant (P<0.05). Of the 67 cases, 9% (n=6) developed bilateral caries on the distal aspect of the mandibular second molar teeth. The angulation, eruption status and proximity to the ACJ of the mandibular third molar teeth in cases where distal caries was present in the adjacent second molar tooth can be seen in Table 4. Of the 352 treatments performed or recommended to GDPs, 4% (n=15) involved the extraction of the mandibular second molar due to distal caries.
Discussion
This study provides an overview of the referrals received at the University Dental Hospital of Manchester, UK, for the management of mandibular third molar teeth between January and June 2019. The most common reason for referral was pericoronitis, experienced in 44% of patient referrals received, followed by caries in the mandibular third and/or second molar in 30% of cases.
Treatment performed varied greatly between patients, with the majority of those assessed meeting the NICE guidance criteria for the extraction of mandibular third molar teeth. The most common treatment performed was the extraction of the mandibular third molar, which occurred in 58% of cases.
Further analysis of patients with established distal caries in the mandibular second molar demonstrated that caries was visible on the distal aspect of the adjacent mandibular second molar tooth in approximately a quarter (24.1%) of patients assessed, a figure that is approximately 14% lower than reported by Toedtling et al.5 In this patient group, which has established distal caries in the mandibular second molar, we observed that 91% of impacted third molars were partially erupted. When comparing between cases that had resulted in the formation of distal caries and those which did not, caries was present in 22% of cases with partially erupted third molars.
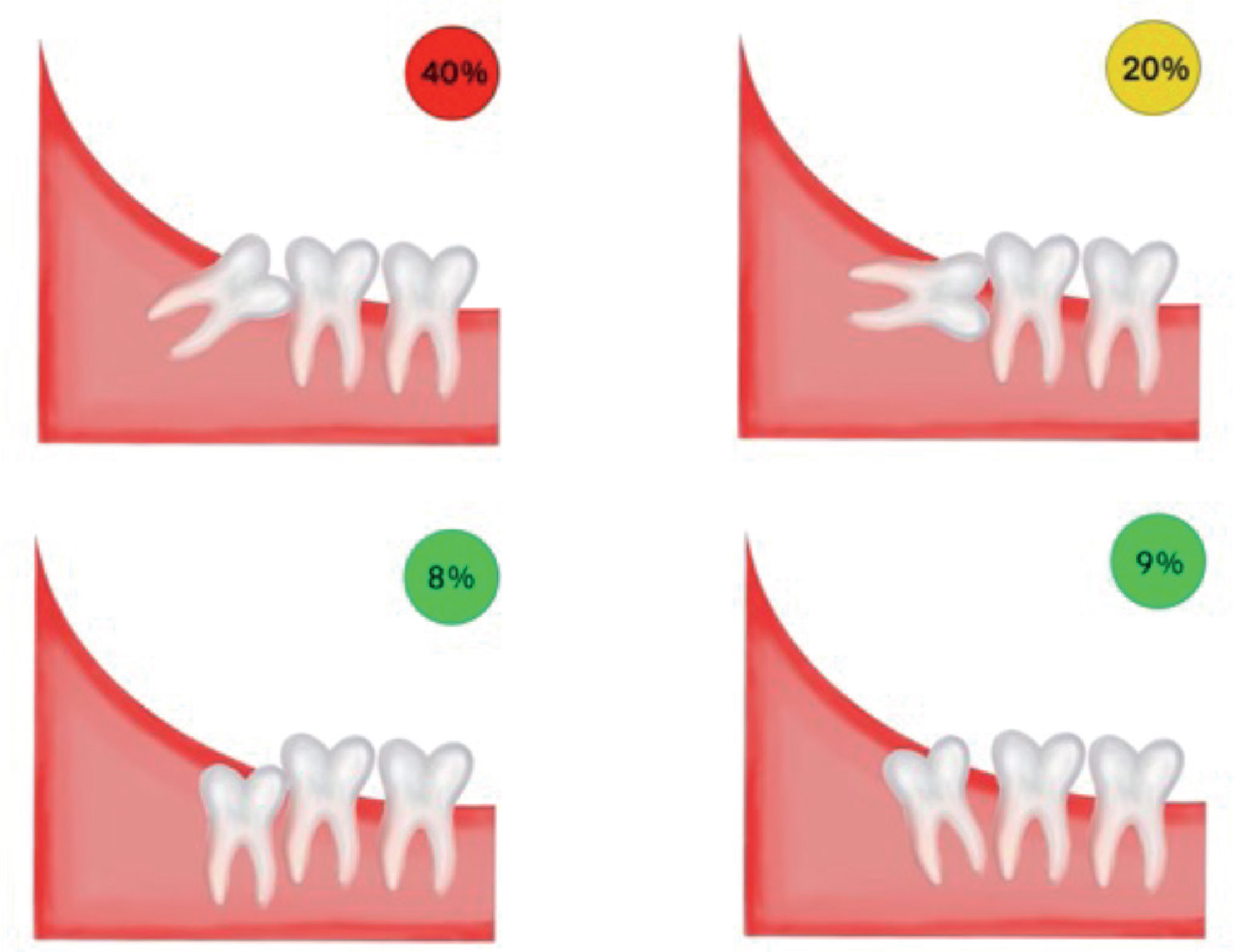
In this patient group the majority of third molar teeth, 76%, were mesio-angular impacted. A comparison of impaction angulation between cases resulting in the formation of distal caries and those which did not, found caries presence in: 40% of cases with mesio-angular impacted third molars; 20% of horizontally impacted third molars; 9% of disto-angular impacted third molars; and 8% of vertically impacted third molar teeth (Figure 1). Therefore, caries was present in approximately 60% of cases where the mandibular third molars were either mesio-angular or horizontally impacted. The correlation between angulation of impaction of the mandibular third molar teeth and the incidence of developing caries in the mandibular second molar is illustrated in Figure 1. Additionally, in 95% of the cases that resulted in caries development, the adjacent third molars were either touching or in close proximity to the ACJ of the second molar tooth. Again when comparing between cases, caries was present in 30% of cases where the adjacent third molars were either touching or in close proximity to the ACJ of the second molar tooth.
Figure 1. Illustration demonstrating incidence of distal caries in mandibular second molar teeth with various angulations of impaction of mandibular third molar teeth: 40% with mesio-angular, 20% with horizontal, 8% with vertical and 9% with disto-angular.
The close proximity of a partially erupted and impacted mandibular third molar tooth creates a breach of the mucogingival seal on the distal aspect of the mandibular second molar tooth. This exposes the distal aspect of the tooth to an environment in which adequate oral hygiene is at best a challenge, but in reality may be impossible to achieve. These compounding factors display an increased susceptibility to caries development on the distal aspect of mandibular second molar teeth.
This study highlighted a clear correlation between the incidence of caries on the distal surface of mandibular second molar teeth and the angulation of impaction, the proximity to the adjacent ACJ and the eruption status of the mandibular third molar. This is not unexpected and has previously been reported by Toedtling et al5 and McArdle and Renton.6 Another interesting finding of this study was the earlier presentation of female patients with distal caries in mandibular second molars. The female patients that presented were approximately 5 years younger than the male patients. This may be due to the fact that the incidence of mandibular third molar impaction is significantly higher in females compared to males,10 with this study appearing to corroborate these findings as over half the patients assessed were female (152 female and 72 male). Additionally, studies have shown a higher prevalence of caries rates, in general, in female patients when compared to males.11,12 As females have a higher incidence of impacted third molars and rates of caries, they may be more predisposed to distal caries in the mandibular second molar tooth and, therefore, may present earlier.
The Faculty of Dental Surgery and Royal College of Surgeons have also published guidance that details the indications for mandibular third molar removal.13 The publication highlights the importance of informing patients of the risks involved with retention of lower third molars, namely the periodontal detriment and the development of caries at the distal aspect of the adjacent lower second molars. Although it does not explicitly suggest that prophylactic removal is indicated, it does state that patient involvement is paramount in the decision-making process and that treatment options should be discussed along with the ‘material risk’ of each option. Furthermore, patients should be fully aware of the associated risks of delaying or declining surgery.
It is acknowledged that this study may have some limitations. Although 224 patients were included within this study, they had all been referred to secondary care for management, often due to more complex presentations. These referred patients have established pathology and, as such, may not be representative of the general population in which the true incidence may be lower.
The data collection was formulated using patient codes logged onto the hospital computer system following a new patient examination. All patients who had undergone an examination were assessed and those who had been referred for assessment of their mandibular third molar teeth were included within the study. It is possible, however, that some clinicians may have not appropriately logged the appointment, and as a result there may have been some patients who did fit the inclusion criteria for this study, but were not present in the data set. Therefore, the data analysed may not be an entirely accurate representation of patients referred to the University Dental Hospital of Manchester during the timeframe set in this study. However, the authors feel that given the search criteria and methods employed, this concern may be negligible.
DMF scoring was used as a marker for dental health; however, due to lack of full mouth radiographs in the majority of patients assessed, a DMF score was only available in 22% of cases. An additional limitation was that radiographs taken upon initial assessment focused on specific areas and not the whole dentition, and thus meant that accurate DMF scores could not be undertaken for many patients within the study. The average score of those assessed was 5.1, however, as only one-fifth of patients were analysed this may not be representative of the group as a whole. It is acknowledged that there are limitations to DMF scoring, with discrepancies in scoring reported.7 Alternative measures for markers of dental health are available however for consistency with other publications the DMF scoring system was used.
Throughout this study, radiographs were predominantly used for caries analysis. As clinical notes varied between clinicians, the use of assessment through radiography provided a clear baseline for data collection. Furthermore, care was taken to exclude radiographs displaying signs suggestive of cervical burnout. Radiographs, however, do not provide an accurate representation of the extent of caries present. A carious lesion may not be evident radiographically until approximately 35% of enamel demineralization has occurred.14 Furthermore, the majority of radiographs analysed were full or half mouth orthopantomographs (OPTs), which are useful for assessing proximity of a third molar tooth to the inferior dental canal; however, when compared to intra-oral radiographs, OPTs have a lower resolution and are more likely to show interproximal overlap. This in turn decreases the accuracy of distal caries diagnosis in mandibular second molar teeth. Within this study, the true incidence of distal caries in a second molar may be higher than the 24% shown, if caries was too early to be observed radiographically using this modality.
Conclusion
Guidance produced by NICE on the removal of mandibular third molar teeth1 aids practitioners and patients in making informed treatment decisions. This guidance does not support the prophylactic removal of mandibular third molar teeth. It is well known that the extraction of these teeth does not come without risks, most notably the risk of damage to the inferior dental and lingual nerves. However, patients with certain presentations, for example mesio-angular or horizontally impacted partially erupted third molars, in contact or intimately involved with the ACJ of the adjacent tooth, may benefit from prophylactic removal or coronectomy because it may prevent extensive restorations or the loss of second molar teeth.