da Silva Figueiredo Sé MJ, Ribeiro APD, Dos Santos-Pinto LAM Are hypomineralized primary molars and canines associated with molar-incisor hypomineralization?. Pediatr Dent. 2017; 39:445-449
Schmalfuss A, Stenhagen KR, Tveit AB Canines are affected in 16-year-olds with molar–incisor hypomineralisation (MIH): an epidemiological study based on the Tromsø study: ‘Fit Futures’. Eur Arch Paediatr Dent. 2016; 17:107-113 https://doi.org/10.1007/s40368-015-0216-6
Kotsanos N, Kaklamanos E, Arapostathis K. Treatment management of first permanent molars in children with molar-incisor hypomineralisation. Eur J Paediatr Dent. 2005; 64:179-184
Albadri S, Zaitoun H, McDonnell ST, Davidson LE. Extraction of first permanent molar teeth: results from three dental hospitals. Br Dent J. 2007; 203:408-409 https://doi.org/10.1038/bdj.2007.679
Marshman Z, Rodd HD. The psychosocial impacts of developmental enamel defects in children and young people.Berlin: Springer; 2015
Balmer R, Toumba J, Godson J, Duggal M. The prevalence of molar incisor hypomineralisation in Northern England and its relationship to socioeconomic status and water fluoridation. Int J Paediatr Dent. 2012; 22:250-257 https://doi.org/10.1111/j.1365-263X.2011.01189.x
Bruce N.Chichester: Research Studies Press Limited; 1980
Alaluusua S. Aetiology of Molar-Incisor Hypomineralization: A systematic review. Eur Arch Paediatr Dent. 2010; 11:53-58 https://doi.org/10.1007/BF03262713
Manton DJ, Crombie FA, Silva MJ. The pathogenesis and aetiology of MIH: more questions than answers.Cham: Springer; 2020
Teixeira R, Andrade NS, Queiroz LCC Exploring the association between genetic and environmental factors and molar incisor hypomineralization: evidence from a twin study. Int J Paediatr Dent. 2018; 28:198-206 https://doi.org/10.1111/ipd.12327
Lygidakis NA, Dimou G, Marinou D. Molar-incisor-hypomineralization (MIH). A retrospective clinical study in Greek children. II. Possible medical aetiological factors. Eur Arch Paediatr Dent. 2008; 9:207-217 https://doi.org/10.1007/BF03262637
Silva MJ, Kilpatrick N, Crombie F What's new in molar incisor hypomineralization?. Dent Update. 2017; 44:100-106
Mathu-Muju K, Wright JT. Diagnosis and treatment of molar incisor hypomineralization. Compend Contin Educ Dent. 2006; 27:604-610
Ghanim A, Silva MJ, Elfrink MEC Molar incisor hypomineralisation (MIH) training manual for clinical field surveys and practice. Eur Arch Paediatr Dent. 2017; 18:225-242 https://doi.org/10.1007/s40368-017-0293-9
Denis M, Atlan A, Vennat E White defects on enamel: diagnosis and anatomopathology: two essential factors for proper treatment (part 1). Int Orthod. 2013; 11:139-165 https://doi.org/10.1016/j.ortho.2013.02.014
Jälevik B, Klingberg G. Treatment outcomes and dental anxiety in 18-year-olds with MIH, comparisons with healthy controls – a longitudinal study. Int J Paediatr Dent. 2012; 22:85-91 https://doi.org/10.1111/j.1365-263X.2011.01161.x
West N, Seong J, Davies M. Management of dentine hypersensitivity: efficacy of professionally and self-administered agents. J Clin Periodontol. 2015; 42:S256-S302 https://doi.org/10.1111/jcpe.12336
Contractor IA, Girish M, Indira M. Silver diamine fluoride: extending the spectrum of preventive dentistry, a literature review. Pediatr Dent J. 2021; 31:17-24
Lygidakis NA, Dimou G, Stamataki E. Retention of fissure sealants using two different methods of application in teeth with hypomineralised molars (MIH): a 4 year clinical study. Eur Arch Paediatr Dent. 2009; 10:223-226 https://doi.org/10.1007/BF03262686
Mahoney EK, Rohanizadeh R, Ismail FS Mechanical properties and microstructure of hypomineralised enamel of permanent teeth. Biomaterials. 2004; 25:5091-5100 https://doi.org/10.1016/j.biomaterials.2004.02.044
William V, Burrow MF, Palamara JE, Messer LB. Microshear bond strength of resin composite teeth affected by molar hypomineralization using 2 adhesive systems. Pediatr Dent. 2006; 28:233-241
Chay PL, Manton DJ, Palamara JE. The effect of resin infiltration and oxidative pre-treatmenton microshear bond strength of resin composite to hypomineralised enamel. Int J Paediatr Dent. 2014; 24:252-267 https://doi.org/10.1111/ipd.12069
Jälevik B, Klingberg GA. Dental treatment, dental fear and behaviour management problems in children with severe enamel hypomineralization of their permanent first molars. Int J Paediatr Dent. 2002; 12:24-32
Einwag J. Effect of entirely preformed stainless steel crowns on periodontal health in primary, mixed dentitions. ASDC J Dent Child. 1984; 51:356-359
Hasmun N, Lawson J, Vettore MV Change in oral health-related quality of life following minimally invasive aesthetic treatment for children with molar incisor hypomineralisation: a prospective study. Dentistry J. 2018; 6 https://doi.org/10.3390/dj6040061
da Cunha Coelho ASE, Mata PCM, Lino CA Dental hypomineralization treatment: a systematic review. J Esthet Restor Dent. 2019; 31:26-39 https://doi.org/10.1111/jerd.12420
Monteiro J, Ashley PF, Parekh S. Vital bleaching for children with dental anomalies: EAPD members' survey. Eur Arch Paediatr Dent. 2020; 21:565-571 https://doi.org/10.1007/s40368-019-00494-w
Greenwall-Cohen J, Greenwall L, Haywood V, Harley K. Tooth whitening for the under-18-year-old patient. Br Dent J. 2018; 225:19-26 https://doi.org/10.1038/sj.bdj.2018.527
Ceci M, Rattalino D, Viola M Resin infiltrant for non-cavitated caries lesions: evaluation of color stability. J Clin Exp Dent. 2017; 9:e231-e237 https://doi.org/10.4317/jced.53110
Williams JK, Gowans AJ. Hypomineralised first permanent molars and the orthodontist. Eur J Paediatr Dent. 2003; 4:129-132
Wu M, Chen L, Bawole E Is there sufficient evidence to support an optimum time for the extraction of first permanent molars?. Eur Arch Paediatr Dent. 2017; 18:155-161 https://doi.org/10.1007/s40368-017-0283-y
Cobourne MT, Williams A, Harrison M. National clinical guidelines for the extraction of first permanent molars in children. Br Dent J. 2014; 217:643-648 https://doi.org/10.1038/sj.bdj.2014.1053
AlQahtani SJ, Hector MP, Liversidge HM. Brief communication: the London atlas of human tooth development and eruption. Am J Phys Anthropol. 2010; 142:481-490 https://doi.org/10.1002/ajpa.21258
Jung YH, Cho BH. Radiographic evaluation of third molar development in 6-to 24-year-olds. Imaging Sci Dent. 2014; 44:185-191 https://doi.org/10.5624/isd.2014.44.3.185
Walshaw EG, Noble F, Conville R Molar incisor hypomineralisation and dental anomalies: a random or real association?. Int J Paediatr Dent. 2020; 30:342-348 https://doi.org/10.1111/ipd.12601
Molar–incisor hypomineralization: paediatric and orthodontic considerations Laura Ewbank Carly Dixon Hesham Ali Siobhan Barry Ovais H Malik Dental Update 2024 49:11, 707-709.
Authors
LauraEwbank
BChD, MSc (Orth), MFDS RCS (Ed), MOrth RCS (Eng)
Post CCST in Orthodontics, University of Manchester Dental Hospital and Royal Blackburn Hospital
Consultant in Orthodontics, University of Manchester Dental Hospital, Higher Cambridge Street, Manchester, M15 6FH, Salford Royal NHS Foundation Trust, Stott Lane, Manchester and Northenden House Orthodontics, Sale Road, Manchester, M23 0DF
This article provides an overview of the paediatric and orthodontic considerations when treating patients with molar–incisor hypomineralization (MIH). Effective management of MIH often requires input and care provision from both paediatric and orthodontic specialties, resulting in collaborative care between these two specialties with a combined treatment plan and regular communication in order to provide the gold standard of care.
CPD/Clinical Relevance: The GDP should be aware of the clinical features of MIH and when to refer to secondary care.
Article
Molar–incisor hypomineralization (MIH) can be defined as ‘demarcated, qualitative developmental defects of systemic origin of the enamel of one or more first permanent molars with or without the involvement of incisors’.1 On occasion, it has also been found to affect second primary molars and primary canines as well as permanent canine cusp tips.2,3
MIH places a high treatment burden on the patient. Evidence shows that children with hypomineralized molars are approximately 10 times more likely to have undergone restorative treatment than the children in control groups.4 Research has also shown that MIH is the second most common reason for extracting first permanent molars (FPM) in children.5 As well as these clinical implications, it is also well known that MIH can have a psychosocial impact on children.6
A UK study of 3233 children found the prevalence of MIH to be 15.9%.7 This means that patients with MIH will regularly be seen in general practice and specialist settings. There are multiple treatment modalities available when treating MIH, including prevention, restorations (both direct and indirect) and extractions. In the NHS, a multidisciplinary approach to care provision has been promoted since 1979, originally by the Royal Commission of the NHS.8 Owing to the complex nature of MIH, effective management often requires input and care provision from multiple specialties and therefore it is important for general dental practitioners (GDPs) to recognize when to refer to secondary care. In this article, we focus on the paediatric and orthodontic considerations for MIH. Collaborative care between these two specialties, with a combined treatment plan and regular communication, provides the patient with the highest treatment level.
Aetiology
The aetiology of MIH remains relatively unclear with multiple studies unable to achieve a consensus on the cause other than that it is likely to be multifactorial.9 Some suggest that childhood illnesses and genetic factors are involved, but further high-quality longitudinal research is required to confirm this.10 A recent cross-sectional study evaluating MIH prevalence between monozygotic and dizygotic twins demonstrated greater concordance of MIH in monozygotic twins.11
Amelogenesis begins between the 28th week in utero and up to 10 days after birth, and it is suggested that any disturbances, pre-, peri- or postnatal, may interrupt ameloblast function resulting in enamel hypoplasia or hypomineralization.12 Medications such as amoxicillin, erythromycin and chemotherapy have also been suggested to affect dental development.13 With this in mind, clinicians should aim to undertake a thorough pre-, peri- and postnatal medical history of a patient with suspected MIH to help to understand the potential cause for all concerned (Table 1).
Question
Further information
Was your child born full term?
Early, late or on time?
Where was your child born?
To evaluate area's water fluoridation if fluorosis is a differential diagnosis
Were there any complications with delivery?
Requirement for neonatal intensive care?Length of hospital stay?
Were there any significant illnesses in the first 2 years of life?
Significant temperaturesChicken poxEar infectionsChest infectionsMultiple courses of antibiotics
Does anyone else in the family have any dental problems?
To evaluate a genetic predisposition for diagnosis such as amelogenesis imperfecta.
Sharp demarcation between clinically affected and unaffected enamel;
Loss of enamel (post-eruptive enamel breakdown);
Tooth sensitivity;
Calculus associated with affected teeth
Atypical caries pattern;
Hypomineralized second primary molars;
If incisors are involved, their defects do not usually involve enamel loss unless the incisal edge is affected.
Figure 1. A 9-year-old twin patient with areas of hypomineralization and signs of post-eruptive breakdown distally in LL6.Figure 2. Twin sibling with areas of hypomineralization and extensive post-eruptive breakdown LL6.Figure 3. Demarcated cream and white lesions on incisal thirds of maxillary central incisors.
Severity
Clinical observations
Mild
Demarcated enamel opacities located at non-stress bearing areas of first permanent molarsNo caries associated with the affected enamelNo hypersensitivityIncisor involvement mild if present
Moderate
Demarcated enamel opacities present on molars and incisorsPost eruptive breakdown limited to one or two surfaces without cuspal involvementAtypical restorations can be requiredNormal dental hypersensitivity
Severe
Post eruptive breakdown, crown destruction or caries associated with affected enamel on molars and incisorsHistory of dental hypersensitivityAesthetic concerns
When diagnosing MIH, it is important to consider the following differential diagnoses of developmental enamel defects.17,18
Amelogenesis imperfecta
A heterogeneous group of genetic conditions characterized by generalized developmental defects of the enamel, affecting its quality and quantity. The enamel can be hypoplastic, show hypomaturation (including hypomaturation–hypoplastic with tauradontism) and be hypocalcified.
Enamel hypoplasia
These quantitative defects have reduced enamel thickness, such as pits and grooves. There can also be areas of missing enamel.
Fluorosis
These are diffuse opacities caused by fluoride ingestion during enamel development.
White spot lesions
These represent an early clinical sign of dental caries. They mainly occur in areas of enamel where plaque has accumulated, such as the gingival margin of the tooth.
Traumatic hypomineralization
This is a potential sequala of periodontal trauma, such as concussion, subluxation, luxation, intrusion, or extrusion to the primary tooth.
Paediatric considerations
There are several considerations for the treatment planning and management of a paediatric patient with MIH, such as the patient's age, the number of teeth affected, the risk of caries, the severity of the presentation, any symptoms, oral hygiene, patient cooperation and impact on the child's quality of life. Therefore, treatment plans must be pragmatic and realistic, with the intention to avoid potential dental anxiety and a long-term high burden of care.19
Management of first permanent molars (FPM)
FPM can rapidly undergo post-eruptive breakdown. Children may present with sensitivity, discolouration concern or brown or ‘cheesy colour teeth’, and in some cases rapid caries progression. The management of FPMs requires a holistic approach involving close communication between the GDP, paediatric dentist and orthodontics.
Prevention
An intensive prevention plan in line with ‘Delivering Better Oral Health’ should be supported, ensuring 1450ppm fluoride toothpaste and topical fluoride applications at least twice per year.20 Routine oral hygiene and dietary advice from the GDP is essential for patients with MIH, who often present with calculus associated with their lower incisors and buccal surfaces of FPMs. For those with increased sensitivity, products containing casein phosphopeptide amorphous calcium phosphate (CPP-ACP, eg Tooth Mousse and MI Paste Plus, both GC Corporation, Tokyo, Japan) have anecdotally been shown to reduce tooth sensitivity. However, a systematic review concluded that the quality of the available evidence was too low and insufficient to be able to recommend the use of CPP-ACP.21
A novel management strategy for reducing dentine hypersensitivity and caries progression is the use of silver diamine fluoride (SDF).22 SDF is a solution composed of diamine-silver and fluoride ions, stabilized by ammonia. The antibacterial properties of silver and fluoride's remineralization properties work synergistically by blocking dentinal tubules to reduce sensitivity on FPM. However, further high-quality evidence is required to support its use in the management of MIH.23,24
If the patient has no sensitivity and minimal enamel hypomineralization, then resin-based fissure sealants to protect porous enamel are recommended, with the primary aim being to cover all affected enamel. To aid retention of hypomineralized molars, it is recommended to bond fissure sealants prior to placement. Fissure sealants should be regularly monitored and replaced as necessary.25
Direct and indirect restorations
The affected enamel of MIH has been demonstrated to show reduced hardness and elasticity, therefore if required, restorations such as composite and indirect metal restorations should be considered.26
For teeth that are partially erupted, an intermediate glass ionomer restoration can be used until complete eruption; this minimizes further post-eruptive breakdown, sensitivity and caries progression. If extraction is indicated, temporization of poor prognosis molars supports the patient until the appropriate time to carry this out.
In cases where there are small hypomineralization defects with post-eruptive breakdown on a single surface, direct composite resin restorations may be used. Consideration should be given to remove any overhangs or unsupported areas of affected MIH during cavity preparation to prevent suboptimal bonding.27 Additional adjuncts, such as sodium hypochlorite under rubber dam may increase bond strength if used before treatment: hypochlorite breaks down proteins that reduce the bond strength of the compromised enamel.28
Teeth that present with MIH are often susceptible to thermal and mechanical stimuli, with noted difficulties in achieving profound anesthesia for restorative procedures.29 To reduce anxiety towards treatment, the use of behavioural management and pharmacological approaches, such as inhalation sedation, may aid compliance.
Pre-formed metal crowns
If extractions are not indicated immediately, or if a FPM is to be retained for orthodontic management, then clinical options such as pre-formed metal crowns (PMC) may be provided. PMC offer a quick, affordable and less technique-sensitive option compared to cast restorations. However, clinicians must take care to ensure the margins are smooth to prevent gingival inflammation, and local anaesthetic may be indicated for patient compliance. PMC can be provided in one clinical appointment, enabling patients to maintain a tooth's functional activity while minimizing further post-eruptive breakdown and reducing sensitivity. It is important to note that PMC should be avoided in patients who have a nickel allergy. If a PMC is provided, then families must be aware of the additional clinical management required as their child develops and the subsequent provision of a definitive restoration in adolescence to prevent periodontal complications.30 For those patients who may not require orthodontic treatment, or those in late adolescence, indirect cast restorations, such as non-precious metal, gold or aesthetic-coloured direct onlays are an option in the cooperative child.9
Management of the anterior dentition
Management of demarcated lesions in the anterior dentition can be of significant concern to some patients and parents, with a psychological impact and an effect on quality of life from an early age.31 The treatment options are dependent on the child's age, cooperation, level of psychological impact, stage of developing dentition and malocclusion.
In mild cases with small, demarcated white spot lesions, treatment may not be indicated, and the lesion can be described to a patient as a ‘freckle’ on their tooth. Routine monitoring is indicated. However, it is essential to listen to the child's concerns and the impact the demarcated lesion may have on the child's overall wellbeing.
Patients with more extensive lesions, may wish to discuss minimally invasive intervention options where the aim of treatment is to improve appearance aesthetics and reduce sensitivity. In all cases, pre- and post-operative photographs should be taken with baseline sensibility testing. When discussing treatment options with patients and parents, it is often important to explain that a combination of conservative approaches may be required to achieve the desired result.
Microabrasion
Microabrasion is a conservative, non-invasive technique, which can be carried out to improve the appearance of superficial brown, cream and white demarcated lesions. Treatment involves a mixture/slurry of pumice and 36% phosphoric acid, or pre-mixed products such as Opalustre (6.6% hydrochloric acid and silica carbide abrasive; Ultradent Products Inc, South Jordan, UT, USA). The technique involves removing a superficial layer of enamel (25–200 nm of enamel) creating a dense, prism-free enamel surface layer. The method usually provides a significant improvement for brown opacities (Figure 4).
Figure 4.
(a) Before and (b) after microabrasion of the maxillary central incisors.
Tooth whitening
Tooth whitening is a minimally invasive treatment, with few side effects, which effectively improves aesthetics for most patients with enamel and dentine discolouration.32 It can be used in combination with microabrasion.
At present, tooth whitening under 18 years of age is a contentious issue due to EU Directive 2011/84/EU. Due to indemnity concerns, several dental institutions within the UK are currently unable to undertake paediatric tooth whitening. However, recent literature shows that there is an increasing discussion for the use of tooth whitening treatment in the paediatric population.33 This article highlights the role of tooth whitening as a minimally invasive management option for MIH.
For at-home whitening, a close-fitting non-reservoir tray should be constructed of 0.35-mm soft acrylic to minimize the amount of bleaching material. A 10% carbamide peroxide concentration is usually recommended for a minimum 2 hours per day, or overnight for maximum effect.34 Pre-operative desensitization using toothpaste containing potassium nitrate can be prescribed from 2 weeks prior to bleaching and during treatment.
Resin infiltration
Resin infiltration, such as with Icon Caries Infiltration (DMG, Hamburg), which is a TEGDMA-resin infiltration system uses the increased porosity of the enamel opacities to fill the lesion and change the refractive index to that of sound enamel, producing optical improvements. Resin infiltration can be used alone, or in combination with microabrasion, or following tooth whitening (Figure 5). Clinicians should note that teeth are often more susceptible to stain post operatively.35
Figure 5.
(a) Before and (b) after treatment with resin infiltration on the maxillary left incisor..
Direct and indirect restorations
If the enamel defects are larger, then indirect composite resin restorations or composite resin veneers may be required (Figure 6). In order to achieve the desired effects to mask the brown opacities, careful removal of the hypomineralized enamel may be required, to increase the bonding capacity for such restorations. Porcelain veneers are contraindicated in patients under the age of 18 years, due to immature gingival margins and large pulp chambers.
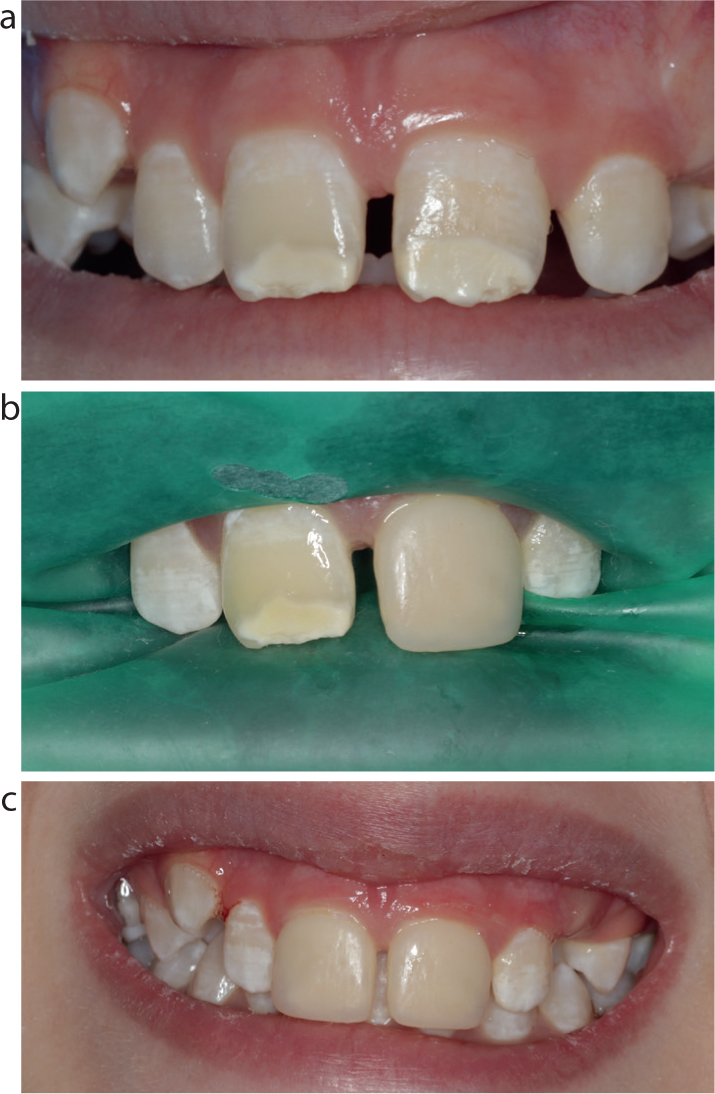
Figure 6.
(a–c) Photos showing maxillary central incisors treated with direct composite resin veneers. Composite resin used: Filket Supreme XTE (3M ESPE).
Orthodontic considerations
It is advisable to refer patients with poor prognosis FPMs for an orthodontic assessment, particularly if the patient has a malocclusion present and extraction of the molars is being considered. If timed correctly, the FPMs can be extracted as part of an orthodontic treatment plan and the patient can be left with no or reduced residual spaces. When a patient is referred in the permanent dentition with poor prognosis FPMs, it may be prudent to consider extraction of these teeth as part of an orthodontic treatment plan. Extractions of FPMs are not routinely carried out in orthodontics owing to the mechanical challenges of closing the larger extraction spaces; however, extraction and space closure will eliminate the lifelong restorative burden for the patient.
Treatment considerations
Initially a comprehensive set of orthodontic records will be taken, including clinical photographs (Figure 7), study models and radiographs. Following this, a number of factors must be considered before deciding on an orthodontic treatment plan.
Figure 7.
(a–e) Orthodontic intra-oral photos showing MIH on the FPMs and incisors. This patient was 14 years old and had a Class I malocclusion with mild crowding.
What is the stage of development of the second permanent molar?
Ideally an orthopantomogram (OPT) should be taken to look at the developing second molars. To allow for the highest chance of spontaneous mesial drift of the lower second molars and subsequent space closure, extraction of the lower FPMs should ideally be carried out before eruption of the lower second permanent molar, which usually falls between 8 and 10 years of age.36 It has been recommended previously that the optimal time for extraction of the FPM is when there is calcification visible in the root bifurcation of the lower second permanent molar. However, a recent systematic review reported that there was no strong evidence to support this claim.37 In the upper arch, the extraction timing is less critical because the unerupted second molar will usually achieve a good position following extraction of the upper FPMs.38
What is the stage of development of the third molar?
It is preferable that, if extracting an FPM, there is presence of a developing third molar, usually present from approximately 8.5 years of age.39 Unfortunately, third molar development is not always visible on an OPT when extraction decisions have to be made.38,40 In cases where there is no radiographic evidence of a developing third molar, and the patient is under 13 years old, then a decision may have to be made about extractions without this information.
Are there any other dental anomalies present?
Undertaking an OPT provides an opportunity to review whether any other dental anomalies are present. A study looking at the prevalence of other dental anomalies associated with MIH found that congenitally missing second premolars were often seen in patients with MIH.41 An association between MIH and diminuitive lateral incisors has also been found.42
Are balancing and/or compensating extractions required?
Balancing and compensating extractions aim to establish occlusal harmony and arch symmetry within the developing dentition.
Generally, when a lower FPM is extracted, then a compensating extraction of the opposing upper FPM can be considered. If the upper molar is unopposed for a significant length of time, then it may overerupt. It is not recommended to carry out a compensating extraction of a lower FPM if an upper FPM is extracted. This is because there is far less chance of the lower permanent tooth overerupting. Owing to the limited evidence supporting balancing extractions, they are not generally recommended when an FPM is extracted.38
What is the patient's presenting malocclusion?
Depending on the patient's presenting malocclusion, retention or extraction of the FPMs may be preferable (Table 3). As a general rule of thumb, if a patient presents in primary care with poor prognosis FPMs, the initial aims of the GDP should be to alleviate pain, temporize, or extract the teeth if they are symptomatic. If possible, the tooth should be retained and if necessary, the patient referred for a specialist orthodontic opinion.
Class I
Plan
Mild crowding
Extract affected FPMs at optimal age for second permanent molars to erupt into good functional position. Usually 8–10 years old
Do not carry out balancing extractions in either arch
If the lower FPM is to be lost, consider compensating extraction of the upper FPM if this tooth is likely to be unopposed for a significant length of time
If the upper FPM is to be lost, do not carry out a compensating extraction
Moderate crowding
Crowding in the buccal segment:
Extract affected FPMs at optimal age for second permanent molars to erupt into good functional position. This will allow for some relief in crowding
If there is buccal segment crowding bilaterally, consider a balancing extraction of the contralateral FPM
A compensating extraction of the upper FPM can be considered to relieve buccal segment crowding
Crowding in the labial segment:
FPM extraction at optimal time; warn patients about possible need for premolar extractions later
Extract FPMs once the second permanent molars have erupted
To summarize, orthodontic assessment is usually advisable when considering FPM extractions, particularly if there are any orthodontic concerns. The underlying malocclusion plays an important role in deciding whether extractions are indicated or if they would be better avoided. Of course, there will be occasions when there is no option and extraction of one or more of the FPMs is unavoidable. If this is the case, and the patient is of the right age and dental development, then consideration should be made to extract the molars at the appropriate time, as outlined above.
Conclusion
If left unmanaged, MIH can cause patients lifelong problems, including pain, discomfort, functional issues, cosmetic concerns and psychosocial issues. Therefore, clinicians must recognize the condition at an early stage and commence its management, referring to secondary care when appropriate. In a secondary care setting for the more complex MIH cases, the patient will benefit from excellent communication and teamwork between the paediatric and orthodontic team.