
References
Immediate management of avulsion injuries in children
From Volume 44, Issue 8, September 2017 | Pages 713-723
Article

Avulsion, whereby a tooth is completely displaced from the socket, is one of the most severe dental injuries.1 The pulp is severed from the neurovascular supply apically and the periodontal ligament is ruptured or torn.2 As soon as the tooth is avulsed the pulp and periodontal ligament begin to undergo ischaemia, with damage also sustained to the surrounding tissues, including cementum, alveolar bone and gingiva.3 Expedient management of avulsion injuries is required as the prognosis of the tooth diminishes with each minute the tooth is out of the socket. As such, an avulsion is a true dental emergency.
However, there is evidence that only 10% of children in the UK receive adequate emergency care following avulsion injuries.4 This can lead to unfavourable outcomes and premature loss of the tooth, which may negatively impact quality of life.5 The ultimate aim of treatment for an avulsed tooth is to achieve periodontal healing and consequently have a similar longevity to an adjacent uninjured tooth. Studies show that the majority of traumatic dental injuries occur during normal working hours and therefore many children will initially present to the primary care setting.6 Therefore, it is imperative that all dentists have sound knowledge of the emergency management of this injury.
Fortunately, avulsion injuries are a rare occurrence, comprising only 0.3–0.5% of all dental injuries.7 Nonetheless, the infrequent nature of these injuries can add to the challenge of their management. It is not surprising that many dentists report low levels of confidence in their ability to treat avulsion injuries.8 In a cohort of dentists in Yorkshire, only 39% had re-implanted and splinted a tooth which had been avulsed.7 There was also limited experience amongst those who had managed an avulsion injury, with most having only re-implanted one or two teeth.7 The aim of this paper is to discuss current guidelines and the practical management of avulsion injuries in the permanent dentition.
Telephone advice
Following an avulsion injury, one fifth of parents are reported to have sought initial telephone advice.6 Furthermore, parents who contacted other healthcare professionals first were advised to attend their dentist.6 As such, it is essential that protocols are in place within both primary and secondary care settings to enable clear and accurate first aid advice to be given by telephone, and an urgent dental review arranged. Appropriate telephone advice is shown in Table 1. During this phone call it is imperative to establish if the avulsed tooth is a primary or permanent tooth. This can be determined by the child's age and asking about the morphology of the tooth, including the tooth size and the presence of mammelons. Once it has been determined that the avulsed tooth is a permanent tooth, the caller should be encouraged to re-implant it immediately without touching the root of the tooth. If the tooth has been re-implanted the child should be asked to bite firmly on a handkerchief and arrangements made for them to attend a dental practitioner as soon as possible.
|
|
Immediate re-implantation is, in most situations, the treatment of choice as it minimizes the extra-oral dry time, however, those at the site may not feel able to perform this task. Where the tooth cannot be re-implanted at the scene, the caller should be advised to place the tooth in a suitable medium and that the child should be brought directly to the dental practice.9
There may be occasions when attending the dental practice immediately is not appropriate, for example, if the child has suffered any other injuries which require urgent medical attention. In instances such as these, the patient should be advised to seek medical attention immediately prior to attending the dental practice.9
Storage medium
The ideal storage medium is a solution which closely simulates the oral environment, which will preserve the periodontal ligament following avulsion.2 Cold milk remains the most convenient and available storage medium which has the potential to keep the periodontal ligament viable for a short period of time. Therefore, milk is generally the medium of choice until the tooth can be re-implanted.2
Other storage media which may be considered are saline, saliva or manufactured solutions such as Hank's balanced salt solution or Viaspan.2 Some guidelines advise that the tooth may be kept in the buccal sulcus until it is re-implanted, but this is not recommended for children due to the risk of swallowing the tooth. An alternative to this is to ask the child to spit saliva into a container and the tooth can subsequently be stored there.10
Assessment
On arrival at the dental practice, the child should be seen promptly. If the tooth has not yet been re-implanted, a member of staff should ensure that it is placed in a suitable storage medium immediately. A brief but comprehensive history and assessment is then required. This should include medical history, dental history and clinical and radiographic examination. A tetanus booster may be required if there has been any environmental contamination of the tooth. A clinical examination should include an extra- and intra-oral examination of hard and soft tissue. Paper-based structured history forms have been shown to be more effective at ensuring that all the appropriate information is recorded, with an example form present in the current UK guidance.9,10,11 This comprehensive assessment will aid in future treatment planning and if required for medico-legal reports.12
There are various factors to be considered during the assessment which may play a role in determining the prognosis of the avulsed tooth and the treatment necessary:
The clinician should consider the age of the child, the history of the injury and the injuries should be compared with the clinical findings to ensure that they are consistent. When there are inconsistencies and concern of non-accidental injury, then local safeguarding policies should be followed.13
Immediate management
The maturity of the avulsed tooth, the extra-alveolar dry time and total extra-alveolar time stored in an appropriate medium should be considered and the appropriate pathway followed.9 These are detailed in the following section and summarized in Figure 1.
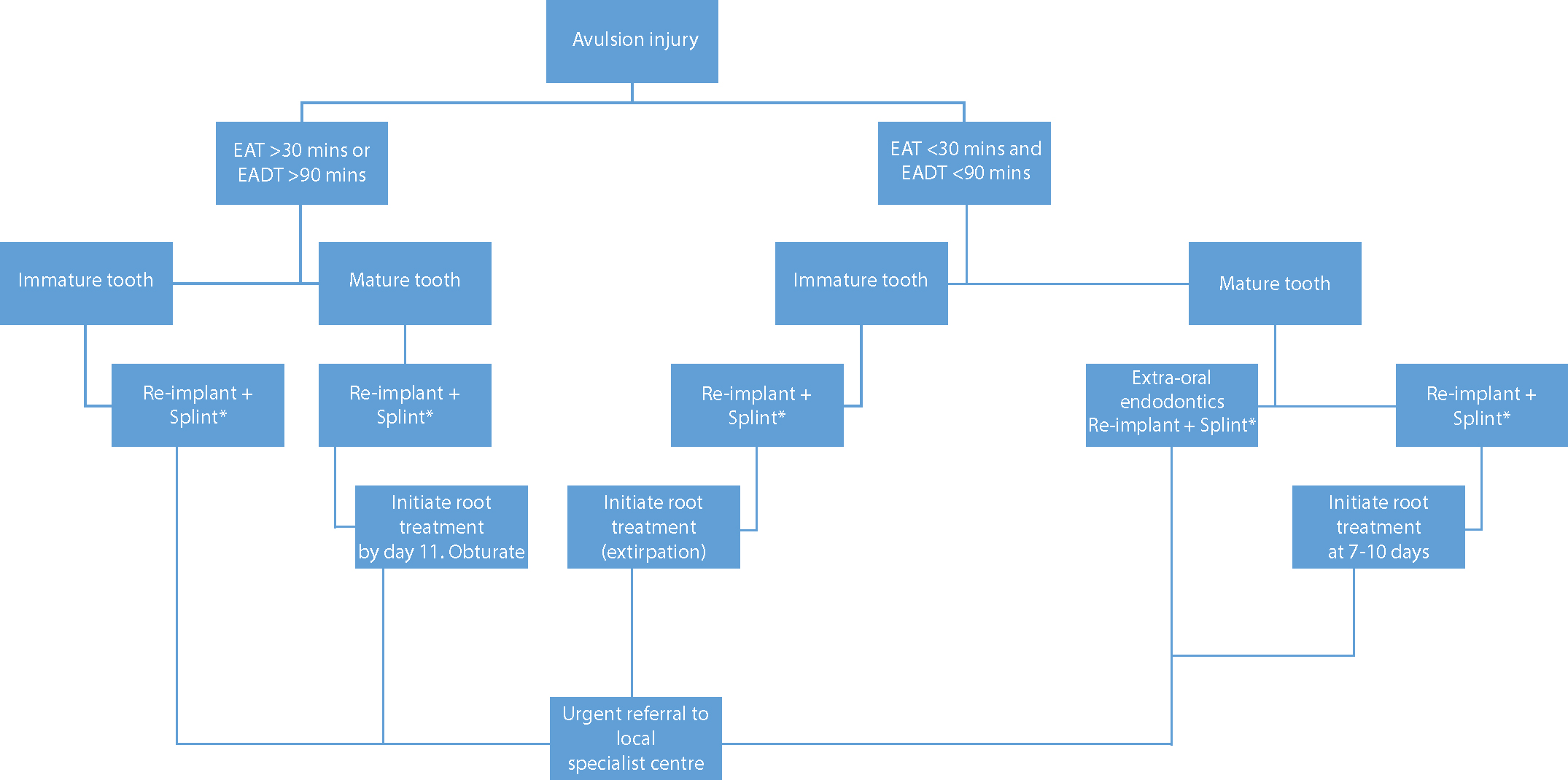
Extra-alveolar dry time less than 30 minutes and total extra-alveolar time less than 90 minutes
Re-implantation
To allow for accurate and comfortable re-implantation, local anaesthetic should be administered on both the buccal and palatal/lingual tissues. Any associated alveolar fractures can then also be reduced. If administration of local anaesthetic proves to be challenging, it may be possible to re-implant the tooth without local anaesthetic where there is minimal disruption to the socket.
Gentle irrigation with saline solution should be carried out to remove the clot within the socket, as this may prevent repositioning the tooth into its original position (Figure 2). Handle the tooth by the crown and not the root surface. If the root surface appears to be contaminated with debris, then it should be washed using physiological saline solution. Stubborn debris can be removed by gently dabbing with gauze soaked in saline, taking care not to cause any further damage to the periodontal membrane.9

The tooth should then be gently placed back in the socket. If the tooth will not re-implant fully then stop and re-assess, as there may be alveolar bone fractures which may prevent re-implantation. A blunt instrument, such as a flat plastic, can be placed in the socket to reposition any bony spicules, before attempting to re-implant the tooth once again.9
There are some circumstances where re-implantation may not be appropriate. These include:11
Endodontic treatment
For an immature tooth there is a chance of periodontal healing and pulpal regeneration. Therefore, endodontic treatment is not indicated and clinical and radiographic monitoring should be carried out. If there is later evidence of pulpal necrosis from clinical and radiographic findings, then extirpation of the pulp is indicated (Figure 3).

In a mature tooth, the tooth should ideally be extirpated prior to Day 7 post-injury, but definitely before Day 11. The canal should be instrumented and decontaminated with sodium hypochlorite. Non-setting calcium hydroxide should then be placed as an inter-visit medicament. The tooth can be obturated after 4 weeks if there is no evidence of infection or resorption.9 Previously, it was recommended that Ledermix® should be placed for up to two months before a period of non-setting calcium hydroxide prior to obturation. However as Ledermix® is currently commercially unavailable, alternatives such as Odontopaste may be used instead.
Extra-alveolar dry time greater than 30 minutes or greater than 90 minutes total extra-alveolar time
A tooth which has been avulsed under these circumstance has little opportunity for periodontal healing or pulpal regeneration and the prognosis of the tooth is considered poor. Therefore, in a mature tooth, root canal treatment can be carried out extra-orally prior to re-implantation or once re-implantation has occurred. Extra-oral endodontic treatment has the advantages of fewer treatment appointments and only attendance for clinical and radiographic review would be required (Figure 4). Furthermore, if the dentist considers that patient compliance to attend multiple appointments for treatment would be poor, extra-oral endodontics may be indicated.

When performing extra-oral endodontic treatment, the tooth should be held by the root with saline or milk soaked in gauze, which prevents further periodontal ligament damage. The pulp chamber is accessed and the necrotic pulp removed using a barbed brooch. The root length is established using direct vision and the tooth irrigated with sodium hypochlorite. The canal is then dried and obturated. If intra-oral endodontic treatment is carried out, then this is indicated at 7–10 days after re-implantation with the same methodology as a mature tooth with an extra-alveolar time less than 30 minutes and total extra-alveolar time of less than 90 minutes.
For the immature tooth the pulp should be extirpated once re-implanted (using the technique described previously) and the root canal disinfected with sodium hypochlorite. For management of the immature tooth, a prompt referral should be made to a specialist paediatric dentist.9
Splinting
Splinting is the standard of care for stabilizing a re-implanted or repositioned permanent tooth following trauma. This immobilizes the tooth in the correct anatomical position and prevents further trauma, allowing healing to occur. A flexible splint should be placed for 7–14 days. A flexible splint is one which attaches to one adjacent uninjured tooth either side of the injured tooth (Figure 5). This allows physiological movement of the teeth, aiding periodontal ligament healing, and should be in place for 7–14 days before it is removed. In instances where an avulsion injury has occurred along with alveolar bone fractures, the splinting time may be increased to allow bony healing.14

The ideal splint should have the following characteristics:15
The chosen splinting method is likely to depend on which materials are available, patient co-operation, and the setting in which the patient is seen. A composite and flexible wire splint is recommended by the British Society of Paediatric Dentistry.9
A composite-wire splint is a flexible orthodontic wire cut to the required length to fit the middle third of the labial surface of the injured tooth and one abutment tooth either side (Figure 6). The teeth are prepared with acid etch and a bonding agent; a small amount of composite is added. The wire is then placed over the composite, then further composite is added, moulded and smoothed before being light-cured.16 It is useful to use a dark shade of composite as it is easy to see and facilitates removal.

Another commonly used splint is the Medartis® MODUS Titanium Splint (TTS) and is secured to the teeth with composite. The splint is made of pure titanium and can be easily adapted to the contour of the dental arch with just the fingers. This flexibility allows physiological tooth mobility without applying orthodontic forces to other teeth.17
Passively placed orthodontic brackets and wire and resin composite materials can also be used for effectively splinting avulsed teeth. Once a splint is placed, advice should be given to the patient and parents to include recommendations for a soft diet for 7–10 days and care when biting. Good oral hygiene by toothbrushing, rinsing with chlorhexidine mouthwash or using chlorhexidine gel around the injured area is key. Advice on appropriate analgesia should be provided. Contact sports should be avoided to reduce the risk of a subsequent injury to the mouth. It may be desirable to arrange to review the patient after 48 hours to check the integrity of the splint, as it may debond where adequate moisture control was not obtained due the nature of the injuries. Following this, a further appointment will be required to remove the splint and extirpate the pulp, if appropriate.
Antibiotics
There is limited evidence in the use of systemic antibiotics to improve the outcome of periodontal or pulpal healing. However, if there is bacterial contamination, there are multiple hard and soft tissue injuries or a complicated medical history, the clinician should use his/her discretion and consider prescribing antibiotics.18 If antibiotics are indicated, a penicillin-based antibiotic should be prescribed for those under 12 years old and doxycycline for those over the age of 12.9
Follow-up
Clinical and radiographic examination should be undertaken after 4 weeks, 3 months, 6 months, 1 year and then yearly thereafter from the time of injury. Clinical tests should include:
Radiographic examination should determine if there is evidence of periapical pathology, ankylosis, resorption or lack of continued root growth.9
The follow-up is most commonly carried out within specialist centres. However, it is important that families understand the need to attend their general dental practitioner for routine care during the follow-up period.
Referral
UK national guidelines for management of avulsion injuries advocate early involvement of specialist inter-disciplinary teams. A telephone discussion or a formal referral should be made to the Specialist in Paediatric Dentistry, in the first instance. This ensures that short-, medium- and long-term treatment planning can be considered, with input from other specialists, if necessary, including orthodontists and oral surgeons.7,8,9,10
A ‘shared care’ treatment plan can then be established for the patient, combining the ease of access to the family GDP with the benefits of specialist care, ensuring that clear communication is maintained between the two.4
Long-term consequences
In an avulsed immature tooth, revascularization and periodontal healing is the most desirable healing response because root development continues.19 However, avulsion injuries carry one of the poorest long-term outcomes for dento-alveolar trauma, with 73–94% of re-implanted teeth being lost prematurely.20 Therefore, long term clinical and radiographic assessment is recommended. It is important to manage patient and parent expectations early on, with regard to possible sequelae and consequences of avulsion injuries and realistic long-term prognosis of the injury. This should include discussions concerning possible loss of the tooth in the long term and potential restorative or orthodontic options following this outcome.
In most circumstances, re-implantation of the tooth is the appropriate decision, even if the prognosis of the tooth is considered poor. Re-implanting the tooth allows sufficient time for all treatment options to be considered.9 The main treatment aim is therefore to try to preserve the tooth for as long as possible, symptom and infection free. This will preserve the alveolar bone for as long as possible, to enable restorative options such as a bridge or implant to be carried out in the future. At the initial visits, it is important that the child and parent are fully informed of the likelihood for premature tooth loss and the increased treatment burden for the patient. They should also be advised of the need for referral to a specialist centre.
Inflammatory root resorption
Inflammatory root resorption is initiated by periodontal ligament damage causing resorption of cementum and exposure of the underlying dentine on the root surface. It is then propagated by a necrotic pulp, which is why early extirpation of the pulp is recommended where there is no chance of pulpal revascularization (ie in a mature tooth). This is a progressive process and prompt treatment is advised by extirpating the tooth and placing an intra-canal dressing of non-setting calcium hydroxide until there is evidence of the process arresting (Figure 7).

Replacement resorption
Ankylosis or replacement resorption is a more common consequence and will lead to ankyloses and infraocclusion. Ankylosis is usually detected 2–12 months after the injury21 and clinically presents as a high pitched percussion tone in comparison to adjacent uninjured teeth. Radiographically, it presents as obliteration of the periodontal space and an uneven contour of the root surface (Figure 8). In a growing child, ankylosis can give rise to aesthetic concerns due to localized infra-occlusion. Ultimately, in a young child, the tooth will be lost in the medium term. Extraction of an ankylosed tooth will inevitably involve the loss of bone. Decoronation prevents this bone loss by removing the crown of the ankylosed and infra-occluded tooth and surgically burying the root in the alveolus. The space can then be restored with the use of an immediate removable appliance. An adhesive bridge can be considered once the permanent dentition has been established.22

Conclusions
Avulsion of a tooth is a dental emergency that requires prompt re-implantation and splinting of the tooth. It is imperative that all dentists are able to provide initial telephone advice and emergency management, including re-implantation and splinting. Early referral to a specialist team will allow short-, medium- and long-term treatment planning to be made due to the poor prognosis of these traumatized teeth as a result of irreversible damage to the periodontal ligament. Therefore, primary care dentists must be aware of their local specialist centre and how to refer appropriately.