Papapanou PN, Sanz M, Buduneli N Periodontitis: consensus report of workgroup 2 of the 2017 World Workshop on the Classification of Periodontal and Peri-implant Diseases and Conditions. J Clin Periodontol. 2018; 45:(S20)S162-S170 https://doi.org/10.1111/jcpe.12946
Dommisch H, Kuzmanova D, Jönsson D Effect of micronutrient malnutrition on periodontal disease and periodontal therapy. Periodontol 2000. 2018; 78:129-153 https://doi.org/10.1111/prd.12233
Brock GR, Chapple ILC. The potential impact of essential nutrients vitamins C and D upon periodontal disease pathogenesis and therapeutic outcomes. Curr Oral Health Rep. 2016; 3:337-346 https://doi.org/10.1007/s40496-016-0116-9
Stein SH, Livada R, Tipton DA. Re-evaluating the role of vitamin D in the periodontium. J Periodontal Res. 2014; 49:545-553 https://doi.org/10.1111/jre.12149
Amrein K, Scherkl M, Hoffmann M Vitamin D deficiency 2.0: an update on the current status worldwide. Eur J Clin Nutr. 2020; 74:1498-1513 https://doi.org/10.1038/s41430-020-0558-y
Bashutski JD, Eber RM, Kinney JS The impact of vitamin D status on periodontal surgery outcomes. J Dent Res. 2011; 90:1007-1012 https://doi.org/10.1177/0022034511407771
Nibali L, Di Iorio A, Tu YK, Vieira AR. Host genetics role in the pathogenesis of periodontal disease and caries. J Clin Periodontol. 2017; 44:(S18)S52-S78 https://doi.org/10.1111/jcpe.12639
Bikle DD. Vitamin D metabolism, mechanism of action, and clinical applications. Chem Biol. 2014; 21:319-329 https://doi.org/10.1038/jid.2014.371
Bjelakovic G, Gluud LL, Nikolova D Vitamin D supplementation for prevention of mortality in adults. Cochrane Database Syst Rev. 2014; (1) https://doi.org/10.1002/14651858.CD007470.pub3
Lechner J, Aschoff J, Rudi T. The vitamin D receptor and the etiology of RANTES/CCL-expressive fatty-degenerative osteolysis of the jawbone: an interface between osteoimmunology and bone metabolism. Int J Gen Med. 2018; 11:155-166 https://doi.org/10.2147/IJGM.S152873
Isola G, Alibrandi A, Rapisarda E Association of vitamin D in patients with periodontitis: a cross-sectional study. J Periodontal Res. 2020; 55:602-612 https://doi.org/10.1111/jre.12746
Jagelavičienė E, Vaitkevičienė I, Šilingaitė D The relationship between vitamin D and periodontal pathology. Medicina (Kaunas). 2018; 54 https://doi.org/10.3390/medicina54030045
Gombart AF. The vitamin D-antimicrobial peptide pathway and its role in protection against infection. Future Microbiol. 2009; 4:1151-1165 https://doi.org/10.2217/fmb.09.87
Dragonas P, El-Sioufi I, Bobetsis YA, Madianos PN. Association of vitamin D with periodontal disease: a narrative review. Oral Health Prev Dent. 2020; 18:103-114 https://doi.org/10.3290/j.ohpd.a44323
Cohen-Lahav M, Shany S, Tobvin D Vitamin D decreases NFκB activity by increasing IκBα levels. Nephrol Dial Transplant. 2006; 21:889-897 https://doi.org/10.1093/ndt/gfi254
Grant WB, Boucher BJ. Are Hill's criteria for causality satisfied for vitamin D and periodontal disease?. Dermatoendocrinol. 2010; 2:30-36 https://doi.org/10.4161/derm.2.1.12488
Timms PM, Mannan N, Hitman GA Circulating MMP9, vitamin D and variation in the TIMP-1 response with VDR genotype: mechanisms for inflammatory damage in chronic disorders?. QJM. 2002; 95:787-796 https://doi.org/10.1093/qjmed/95.12.787
Gruber R. Osteoimmunology: inflammatory osteolysis and regeneration of the alveolar bone. J Clin Periodontol. 2019; 46:52-69 https://doi.org/10.1111/jcpe.13056
Chapple ILC, Brock G, Eftimiadi C, Matthews JB. Glutathione in gingival crevicular fluid and its relation to local antioxidant capacity in periodontal health and disease. Mol Pathol. 2002; 55:367-373 https://doi.org/10.1136/MP.55.6.367
Wimalawansa SJ. Vitamin D deficiency: effects on oxidative stress, epigenetics, gene regulation, and aging. Biology (Basel). 2019; 8:1-15 https://doi.org/10.3390/biology8020030
Jain SK, Micinski D. Vitamin D upregulates glutamate cysteine ligase and glutathione reductase, and GSH formation, and decreases ROS and MCP-1 and IL-8 secretion in high-glucose exposed U937 monocytes. Biochem Biophys Res Commun. 2013; 437:7-11 https://doi.org/10.1016/J.BBRC.2013.06.004
Sepidarkish M, Farsi F, Akbari-Fakhrabadi M The effect of vitamin D supplementation on oxidative stress parameters: a systematic review and meta-analysis of clinical trials. Pharmacol Res. 2019; 139:141-152 https://doi.org/10.1016/J.PHRS.2018.11.011
Costantini E, Sinjari B, Piscopo F Evaluation of salivary cytokines and vitamin D levels in periodontopathic patients. Int J Mol Sci. 2020; 21 https://doi.org/10.3390/ijms21082669
Dietrich T, Joshipura KJ, Dawson-Hughes B, Bischoff-Ferrari HA. Association between serum concentrations of 25-hydroxyvitamin D3 and periodontal disease in the US population. Am J Clin Nutr. 2004; 80:108-113 https://doi.org/10.1093/ajcn/80.1.108
Jimenez M, Giovannucci E, Kaye EK Predicted vitamin D status and incidence of tooth loss and periodontitis. Public Health Nutr. 2014; 17:844-853 https://doi.org/10.1016/j.physbeh.2017.03.040
Antonoglou GN, Suominen AL, Knuuttila M Associations between serum 25-hydroxyvitamin D and periodontal pocketing and gingival bleeding: results of a study in a non-smoking population in Finland. J Periodontol. 2015; 86:755-765 https://doi.org/10.1902/jop.2015.140262
Abreu OJ, Tatakis DN, Elias-Boneta AR Low vitamin D status strongly associated with periodontitis in Puerto Rican adults. BMC Oral Health. 2016; 16:1-5 https://doi.org/10.1186/s12903-016-0288-7
Ho YP, Lin YC, Yang YH Association of vitamin D receptor gene polymorphisms and periodontitis in a Taiwanese Han population. J Dent Sci. 2017; 12:360-367 https://doi.org/10.1016/j.jds.2017.07.001
Deng H, Liu F, Pan Y BsmI, TaqI, ApaI, and FokI polymorphisms in the vitamin D receptor gene and periodontitis: a meta-analysis of 15 studies including 1338 cases and 1302 controls. J Clin Periodontol. 2011; 38:199-207 https://doi.org/10.1111/j.1600-051X.2010.01685.x
Guo HX, Pan J, Pan HB Correlation of vitamin D receptor gene (ApaI) polymorphism with periodontitis: a meta-analysis of Chinese population. Food Sci Nutr. 2019; 7:3607-3612 https://doi.org/10.1002/fsn3.1215
Chen L, Li H, Zhang P, Wang S. Association between vitamin D receptor polymorphisms and periodontitis: a meta-analysis. J Periodontol. 2012; 83:1095-1103 https://doi.org/10.1902/jop.2011.110518
Baldini A, Nota A, Fanti E Association between periodontal disease and interleukin-1β +3953 and vitamin D receptor Taq1 genetic polymorphisms in an Italian caucasian population. Ann Stomatol (Roma). 2013; 4:191-195 https://doi.org/10.11138/ads/2013.4.2.191
Ji XW, Wang Y, Cao C, Zhong LJ. Assessment of the link between vitamin D receptor TaqI gene polymorphism and periodontitis: a meta-analysis in a Chinese population. Genet Mol Res. 2016; 15:1-8 https://doi.org/10.4238/gmr.15048883
Meghil MM, Hutchens L, Raed A The influence of vitamin D supplementation on local and systemic inflammatory markers in periodontitis patients: a pilot study. Oral Dis. 2019; 25:1403-1413 https://doi.org/10.1111/odi.13097
Gao W, Tang H, Wang D Effect of short-term vitamin D supplementation after nonsurgical periodontal treatment: a randomized, double-masked, placebo-controlled clinical trial. J Periodontal Res. 2020; 55:354-362 https://doi.org/10.1111/jre.12719
Tonetti MS, Chapple ILC. Biological approaches to the development of novel periodontal therapies - Consensus of the Seventh European Workshop on Periodontology. J Clin Periodontol. 2011; 38:114-118 https://doi.org/10.1111/j.1600-051X.2010.01675.x
Sanz M, Herrera D, Kebschull M Treatment of stage I-III periodontitis – the EFP S3 level clinical practice guideline. J Clin Periodontol. 2020; 47:4-60 https://doi.org/10.1111/jcpe.13290
Laky M, Bertl K, Haririan H Serum levels of 25-hydroxyvitamin D are associated with periodontal disease. Clin Oral Investig. 2017; 21:1553-1558 https://doi.org/10.1007/s00784-016-1965-2
Dodington DW, Fritz PC, Sullivan PJ, Ward WE. Higher intakes of fruits and vegetables, β-carotene, vitamin C, α-tocopherol, EPA, and DHA are positively associated with periodontal healing after nonsurgical periodontal therapy in nonsmokers but not in smokers. J Nutr. 2015; 145:2512-2519 https://doi.org/10.3945/jn.115.211524
Lee HJ, Je D Il, Won SJ Association between vitamin D deficiency and periodontal status in current smokers. Community Dent Oral Epidemiol. 2015; 43:471-478 https://doi.org/10.1111/cdoe.12173
Antonoglou GN, Knuuttila M, Niemelä O Low serum level of 1,25(OH)2D is associated with chronic periodontitis. J Periodontal Res. 2015; 50:274-280 https://doi.org/10.1111/jre.12207
Millen A, Andrews C, LaMonte M Vitamin D status and five year changes in periodontal disease measures among postmenopausal women: The Buffalo OsteoPerio Study. J Periodontol. 2014; 85:1321-1332 https://doi.org/10.1016/j.gde.2016.03.011
Boggess KA, Espinola JA, Moss K Vitamin D status and periodontal disease among pregnant women. J Periodontol. 2011; 82:195-200 https://doi.org/10.1902/jop.2010.100384
Dietrich T, Nunn M, Dawson-Hughes B, Bischoff-Ferrari HA. Association between serum concentrations of 25-hydroxyvitamin D and gingival inflammation. Am J Clin Nutr. 2005; 82:575-580 https://doi.org/10.1093/ajcn/82.3.575
Perić M, Maiter D, Cavalier E The effects of 6-month vitamin D supplementation during the non-surgical treatment of periodontitis in vitamin-D-deficient patients: a randomized double-blind placebo-controlled study. Nutrients. 2020; 12:1-12 https://doi.org/10.3390/nu12102940
Woelber JP, Gärtner M, Breuninger L The influence of an anti-inflammatory diet on gingivitis. A randomized controlled trial. J Clin Periodontol. 2019; 46:481-490 https://doi.org/10.1111/jcpe.13094
Woelber JP, Bremer K, Vach K An oral health optimized diet can reduce gingival and periodontal inflammation in humans - a randomized controlled pilot study. BMC Oral Health. 2017; 17:1-8 https://doi.org/10.1186/s12903-016-0257-1
Perayil J, Menon K, Kurup S Influence of vitamin D and calcium supplementation in the management of periodontitis. J Clin Diagn Res. 2015; 9 https://doi.org/10.7860/JCDR/2015/12292.6091
Baumgartner S, Imfeld T, Schicht O The impact of the stone age diet on gingival conditions in the absence of oral hygiene. J Periodontol. 2009; 80:759-768 https://doi.org/10.1902/jop.2009.080376
Periodontitis results from dysbiotic periodontal microbiota eliciting an exaggerated host immune-inflammatory response within susceptible individuals. With traditional biofilm management only partially effective, it became apparent that the individual's host response played a pivotal role in the pathogenesis of periodontitis. Specific nutritional factors have been found to impact the host response. Understandably, this has contributed to the emerging shift in contemporary research towards biological approaches to novel periodontal therapies. Vitamin D deficiency, a global public health problem, has been linked to numerous inflammatory conditions including periodontitis. The effects of vitamin D are multifaceted, favouring periodontal health and consideration should be given to its application in clinical practice.
CPD/Clinical Relevance: The mechanisms and evidence implicating vitamin D as a host modulator of periodontitis are of relevance in periodontal therapy.
Article
Periodontitis is the comprehensive outcome of microbial dysbiosis eliciting an exaggerated host immune-inflammatory response within susceptible individuals, resulting in substantive attachment loss and alveolar bone resorption.1,2 Individual variability in the host response to periodontitis is modulated by a variety of risk factors: genetic (gene polymorphisms), environmental (stress, bacteria) and/or lifestyle (nutritional).3 Such factors can adversely affect the onset and progression of periodontitis. Recognition, investigation and subsequent modification of the risk factors, wherever possible, is integral in providing a holistic and precise approach to the management of periodontitis.
Vitamin D is a micronutrient required as part of a balanced diet. Investigations to establish the aetiology and concurrent management of rickets and scurvy led to its discovery in 1922.4 Traditionally, the role of vitamin D has been recognized in mineral and skeletal homeostasis. Yet compelling evidence supports the notion of serum vitamin D's ability to demonstrate antimicrobial and anti-inflammatory properties.5,6 Evidence has also emerged implicating it as a modulator of bone metabolism.5,7 With both, the immune response and bone metabolism, pathognomonic of periodontitis, it would be remiss of the field of periodontology not to further research the micronutrient as a host modulator and its deficiency as a risk factor of periodontitis.
With genetic risk factors elucidated in the aetiology of periodontitis and genomic effects of vitamin D mediated via the vitamin D receptor (VDR), VDR gene polymorphisms (DNA sequence variations) are currently under investigation for an association with periodontitis.8,9
Vitamin D overview
Vitamin D2 (ergocalciferol) and vitamin D3 (cholecalciferol) are the two major forms of vitamin D – a secosteroid.9 In this article, the term vitamin D will refer to both forms.
Biochemistry
Vitamin D is the product of photochemical reactions using sunlight containing UVB radiation. It can be obtained from two main sources: endogenous production via cutaneous synthesis (vitamin D3); and diet (vitamin D2 and D3). Factors affecting the rate of vitamin D3 formation include UVB radiation and melanin. The former is affected by the zenith angle of the sun, altitude, cloud cover and air pollution.9 Quantitatively, cutaneous synthesis is the most important source and dietary derived sources, listed in Table 1, tend to play supporting roles where inadequate cutaneous production is apparent.9,10 Rich dietary sources of vitamin D2 are limited, resulting in fortified foods. Natural food sources rich in vitamin D3 include egg, oily fish and animal products.9
Food
Mean vitamin D content per 100 g
μg
IU
Fish
Herring (grilled)
Salmon (farmed, grilled)
Mackerel (grilled)
Sardines (grilled)
Tuna (baked)
16.17.88.55.13.1
644312340204124
Eggs
Egg (whole, boiled)
Egg (yolk, boiled)
0.2/12812.6
128504
Meat
Liver (lamb, fried)
Liver (calf, fried)
Beef (rump steak, fried)
0.90.30.7
361228
Fortified foods
Bran flakes
Cornflakes
Rice cereal
Fat spreads
4.24.24.27.5
168168168300
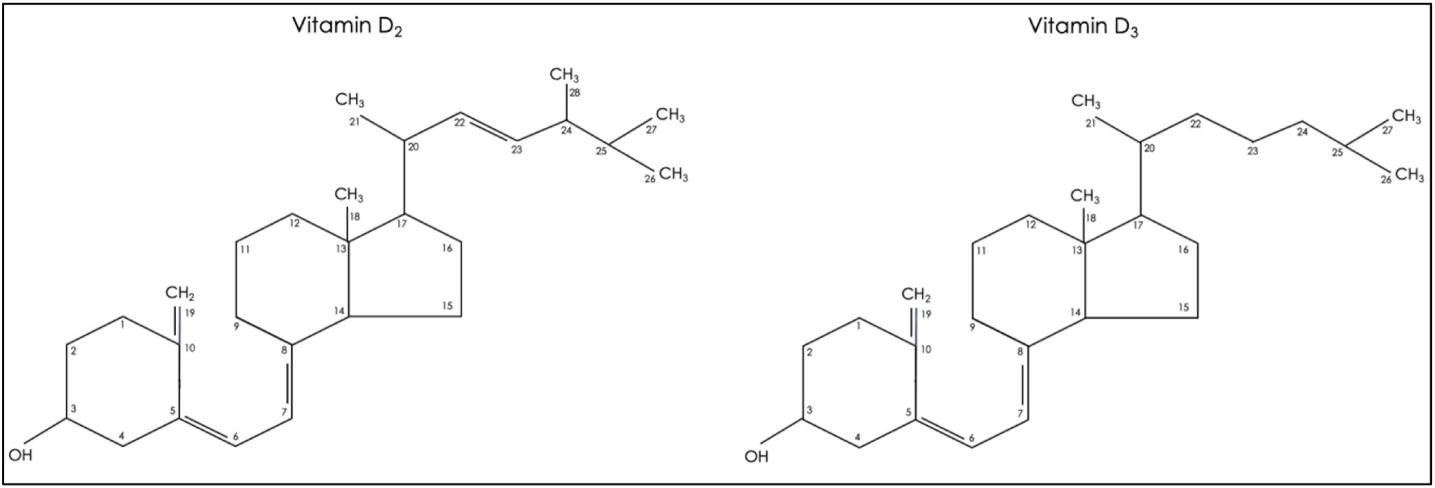
A double bond between carbon atoms 22 and 23 and a methyl (-CH3) side chain at carbon atom 24 gives vitamin D2 a molecular mass 3.1% greater than that of its analogue (Figure 1). This distinguishing factor results in its reduced affinity for vitamin D binding protein (VDP), an important molecule in the transport of vitamin D. Consequently, vitamin D2 has a faster clearance from the circulation, which limits its conversion to the active form.9,10 Therefore, vitamin D2 will not result in as high a serum level of the subsequent substrate forms of vitamin D as will comparable amounts of vitamin D3.10
Figure 1. Molecular structures of vitamin D2 and D3.
The biologically inert dietary and endogenous forms of vitamin D, bound to VDP, are transported to the liver to undergo two hydroxylation reactions for activation:9,10
25-hydroxylation:
vitamin D → 25-hydroxyvitamin D (25(OH)D);
– 25(OH)D binds to VDP and is transported to the kidney;
1α-hydroxylation:
25(OH)D → 1,25-dihydroxyvitamin D (1,25(OH)2D)
Despite 25(OH)D being biologically inactive, it is a recognized biomarker owing to its long half-life and ability to reflect the cumulative cutaneous and dietary supply of the micronutrient.9
Vitamin D deficiency
Vitamin D deficiency, a global public health concern, is estimated to affect 20% of the UK population.9 With the universal definition of vitamin D deficiency still under debate, there is considerable global variation in the threshold considered as deficient. Deficiency in the UK is defined as serum levels of 25(OH) D <25 nmol/l, but <50 nmol/l elsewhere.6,9
The micronutrient's deficiency has been connected to a number of health outcomes: cardiovascular disease, respiratory failure, sepsis, diabetes, adverse pregnancy and musculoskeletal health outcomes.6,9 Reduced all-cause mortality and cancer mortality, of 7% and 13%, respectively, were demonstrated in a meta-analysis where patients received vitamin D3 supplementation.11
Units of measurement and reference nutrient intake
As defined by World Health Organization (WHO), 1 international unit (IU) of vitamin D is equivalent to the activity, which is molecular mass dependent, of 0.025 μg crystalline vitamin D3. Despite this, the conversion continues to be generalized to both forms of vitamin D.9
Reference nutrient intake (RNI) is defined as the amount of required nutrient to meet the needs of 97.5% of the population. The Scientific Advisory Committee on Nutrition (SACN) recommends an RNI of 10 μg/day (400 IU/day) for individuals of the UK population over 4 years old, including pregnant, lactating and susceptible patient groups. ‘Safe intake,’ a precautionary approach, is proposed as 10 μg daily in children between 1 and 4 years of age and 8.5–10 μg daily in exclusively and part breastfed children from birth to 1 year of age.9
Mechanisms of action linking vitamin D and periodontitis
Genomic effects of vitamin D are exerted via the VDR. This receptor is responsible for the transcribing of over 1400 genes – the equivalent of 4% of all human genes.12 Genomic activity of vitamin D demonstrates antimicrobial and immunomodulatory, more specifically anti-inflammatory, mechanisms of action.13 Thus, theoretically VDR gene polymorphisms could have an impact on disease susceptibility and progression through altered gene expression and subsequent mechanisms of action.
Antimicrobial
LL-37 cathelicidin antimicrobial peptide (CAMP) prevents increased susceptibility to infection via chemotaxis, cytokine and chemokine production, and neutralization of bacterial endotoxins. Transcription of the CAMP gene is induced by 1,25(OH)2D.14 Furthermore, 1,25(OH)2D can induce the expression of β-defensins, which have been shown to exhibit antimicrobial activity on Porphyromonas gingivalis, Fusobacterium nucleatum and Aggregatibacter actinomycetemcomitans, pathogens well cited in cases of periodontitis.10,14,15,16,17, Its antimicrobial role can be further demonstrated in its role in autophagy, a homeostatic process involving the disposal of damaged cells to encourage new cell production. In addition, it can co-localize with microbial material within autophagosomes to degrade invading pathogens.18 These mechanisms may form part of the important first-line defence in VDR-bearing oral epithelial cells when under bacterial insult.
Anti-inflammatory
Vitamin D is a potent regulator, critical in innate and adaptive immunity.10 Enhancement of innate immunity via toll-like receptor (TLR) activation induces the expression of CAMP. On the contrary, it has the ability to downregulate the adaptive immunity via inhibitory mechanisms. This results in two key effects: reduced activation, differentiation and maturation of T cells; and suppressed production of vital cytokines including, but not limited to, the pro-inflammatory cytokines IL-2, IL-6 and IFN-γ.10,16
Protective mechanisms of vitamin D are further demonstrated with its inhibitory impact on tumour necrosis factor-α (TNF-α), a critical mediator with the ability to initiate a pro-inflammatory cascade at the site of infection. Transcriptional activation of the TNF-α gene is predominantly dependent on transcriptional factor nuclear factor-κB (NFκB), which becomes suppressed by 1,25(OH)2D.19
Matrix metalloproteinases (MMPs) are enzymes active in the degradation of collagen and are present in large amounts, particularly MMP-9, in periodontitis subjects.20 Evidence illustrates vitamin D supplementation (VDS) can result in reduced plasma concentration of MMP-9.21 Thus, suggesting vitamin D's capability to modulate another protective and anti-inflammatory mechanism in periodontitis.
Osteo-immunology is a relatively new concept that underpins the crosstalk between the immune system and bone metabolism.22 It has a role in not only pathological bone loss, but also offers molecular mechanisms for bone regeneration and could prove to be a useful principle to exploit in designing next-generation regenerative therapies.23 While there is limited research in the impact of vitamin D and osteo-immunology per se, its relevance to vitamin D can be assumed using the anti-inflammatory and immune mechanisms discussed earlier.
Oxidative stress
Reactive oxygen species (ROS) is a blanket term describing molecules that are free radicals or capable of producing them (oxidants). A shift to favour ROS results in oxidative stress. Oxidative stress is defined as ‘an imbalance between oxidants and antioxidants in favour of the oxidants, leading to a disruption of redox signalling and control and/or molecular damage.’24 It is a key mechanism involved in the destructive process seen in periodontitis.25
Adequate 25(OH)D levels may play a role in downregulating oxidative stress-related activities. One mechanism may involve vitamin D-dependent modulation of the expression of nuclear factor erythroid-2-related factor 2 (Nrf2). An inverse correlation between the intracellular level of Nrf2 and accumulation of mitochondrial ROS is evident, resulting in the subsequent upsurge of oxidative stress.26
Glutathione, in its reduced form (GSH) is an essential and potent antioxidant responsible for scavenging oxygen radicals, crucial for maintaining redox status. Diminished glutathione levels have been associated with periodontitis.25In vitro studies have demonstrated vitamin D acting via the glutathione redox pathways by upregulating glutathione reductase and glutamate cysteine ligase with subsequent increase of intracellular glutathione.27
Interestingly, a systematic review and meta-analysis investigating the effects of VDS on oxidative stress demonstrated improvements in specific parameters: an increase in total antioxidant capacity and GSH, as well as reductions in malondialdehyde (MDA), a product of lipid peroxidation where free radicals damage the structural integrity of cells.28
Association between vitamin D and periodontitis
An array of studies (Table 2), discuss the association between vitamin D and periodontitis. Supporting the notion of vitamin D's anti-inflammatory role, a longitudinal study found an inverse association between 25(OH)D and salivary cytokine production.29 Lower quintiles of 25(OH)D levels have revealed greater clinical attachment loss (AL) of 0.39 mm or 0.26 mm in men and women, respectively,30 while higher quintiles of serum 25(OH)D demonstrate a reduced incidence of periodontitis, reduced prevalence of teeth associated with deeper periodontal pockets and tooth loss.31,32 In addition, an increase in vitamin D increments reduced the odds of developing moderate and severe periodontitis and alveolar bone loss.33,34
Low serum 25(OH)D levels were significantly associated with PD. 48% of PD subjects found to have deficient 25(OH) D levels (<50 nmol/l) compared to 14% of HC
Statistically significant lower levels of 25(OH)D in PD subjects compared to HC. Patients with moderate/severe PD had a12% OR reduction with every unit (ng/ml) increase in serum 25(OH) D levels
A statistically significant product term is apparent between plaque, serum 25(OH)D and number of teeth with deep periodontal pockets (≥4 mm). There is a lower proportion of teeth with ≥4 mm pockets in subjects with good OH, in higher 25(OH)D quintiles, indicative of a protective property of serum 25(OH)D
No significant association between serum 25(OH)D levels and periodontitis. A significant inverse association between 1,25(OH)2D and PD was found and may be explained by the increased use of 1,25(OH)2D via immunomodulatory mechanisms in PD patients
Older male adults with no reported history of PD;42730
Prospective
Self-reported tooth loss and periodontitis
Predicted serum 25(OH)D
Statistically significant inverse association was observed between predicted serum 25(OH) D and tooth loss and also in periodontitis after covariate adjustments (BMI, ethnicity and physical activity)
Reduced 25(OH)D levels were observed in those who displayed greater percentage BOP. No statistically significant association between baseline serum 25(OH)D and PD progression
Total vitamin D intake was inversely associated with odds of moderate and severe PD and ABL. Every 100 IU increment in daily vitamin D intake was associated with reduced odds (OR=0.97) of severe PD
Statistically significant association between 25(OH)D insufficiency (using two different cutpoints <37.5 nmol/l and <50 nmol/l) and moderate to severe PD
A strong inverse association between 25(OH)D and the prevalence of BOP was observed. 30 nmol/l increase in serum 25(OH) D can result in 10% lower odds for BOP
Subjects ≥50 years old had a significant inverse association between serum 25(OH) D concentrations and PD. Subjects in the lowest 25(OH)D quintile displayed greater AL (M: 0.39; F: 0.26mm). No association found in subjects <50 years old
ABL: alveolar bone loss; AL: attachment loss; BOP: bleeding on probing; CAL: clinical attachment level; CPI: community periodontal index; FMBS: full mouth bleeding score; FMPS: full mouth plaque score; FFQ: food frequency questionnaire; GP: gingivitis parameters; HC: healthy controls; NSPT: non-surgical periodontal therapy; OH: oral hygiene; OR: odds ratio; PD: periodontitis; PP: periodontal parameters; PPD: periodontal pocket depth.
The interpretation of the research is complicated by varied definitions of vitamin D deficiency, biomarker and periodontal measurements, and methodological designs. Taken together, such variations in study designs contribute to the difficulty in performing a meta-analysis of studies. Nonetheless, numerous studies explored in Table 2 identified statistically significant associations between reduced vitamin D levels and poor periodontal parameters and increased vitamin D levels with favourable periodontal health. Such results are appealing for the management of periodontitis.
Association between VDR polymorphisms and periodontitis
Among putative genetic risk factors, the VDR gene is one of three genes that have emerged as having a strong level of evidence with periodontitis.8 Restriction fragment length polymorphisms (RFLPs) have been identified in TaqI (rs731236), ApaI (rs7975232), BsmI (rs1544410) and FokI (rs2228570).35,36
Table 3 presents some of the studies that have examined VDR polymorphisms and periodontitis. While some meta-analyses demonstrate ApaI may be associated with a reduced risk of periodontitis in a Chinese population, another found it could not be generalized to Caucasians.36,37,38 Protective associations to periodontitis with a TaqI variant is evident in some case-control studies.38,39 Yet, meta-analyses have shown that the TaqI polymorphism has no association to periodontitis.36,40 While two meta-analyses demonstrated FokI variants to be implicated in ‘aggressive’ periodontitis in subjects of Asian origin, another found no significant association in any genotype of FokI.35,36,38 Furthermore, conflicting findings between BsmI and periodontitis are evident.36,38
Statistically significant associations of tt genotype of TaqI polymorphism with reduced prevalence of t allele (71%) in PD subjects, compared to HC (92%), suggesting the t allele may play a protective role
Significant association detected between t allele of TaqI and CP in Asian but not in the European population. Mutant allele F of FokI appeared to be a risk factor of AP in Asians. No significant associations to PD in polymorphisms of ApaI and BsmI
Asians with CP had significantly lower frequency of bb genotype of BsmI; significantly higher frequency of AA genotype of ApaI; and weak significantly higher frequency of TT genotype of TaqI. No significant difference found in any genotype of FokI
The lack of concrete associations between VDR polymorphisms and periodontitis may be reflective of the different exposures among populations as phenotypic heterogeneity is the combined result of genetic, environmental and biological interactions. Such conflicting results have led to limited success in deciphering significant and reproducible VDR gene polymorphisms for susceptibility to periodontitis.
Effects of vitamin D supplementation on periodontitis and periodontal therapy
There are few interventional studies assessing VDS solely as an adjuvant to periodontal therapy, which makes it difficult to draw definitive conclusions. Nevertheless, those that are available show promising results. A double-blind randomized controlled trial (RCT) allocated adult patients with moderate to severe periodontitis to experimental groups that received daily 4000 IU oral VDS for 16 weeks, or a placebo. At week 8, both groups, underwent non-surgical periodontal therapy (NSPT) with the aim of eliciting a systemic inflammatory response. Although no significant effects on periodontal parameters were observed after 16 weeks, this RCT highlighted two pivotal outcomes of VDS in the experimental group: reduced cytotoxic T cells routinely involved in tissue damage; and increased induction of autophagy-related proteins. Therefore, it can be hypothesized that VDS can mediate and counteract the cytotoxic T cell response during periodontal therapy, which could otherwise increase periodontal tissue damage.41
Consistent with the studies listed in Table 4, Gao et al found improvements in periodontal health parameters in their double-blind RCT. The RCT involved moderate to severe periodontitis subjects who underwent 3 months of NSPT prior to assignment to one of two intervention groups (daily 1000 IU or 2000 IU vitamin D) or a placebo group. Dose-dependent and statistically significant increased reductions in AL and periodontal pocket depths (PPD) for moderate and deep periodontal pockets were evident among intervention groups.42 Although, differences between the intervention and placebo groups were statistically significant, they may not be clinically remarkable.
Europeans ≥30 years old with CP and serum 25(OH)D levels <30 ng/mL undergoing NSPT;27
RCT
EG: 25000 IU VDS weekly for 6 months
CG: Placebo
PP: FMBS, FMPS, PPD
Serum 25(OH)D
EG displayed greater decrease in number of sites with PPD ≥ 4mm compared to CG. However, the inter-group difference was non-significant at all time points. No statistically significant differences in inter-group comparisons for FMBS and FMPS
EG had reduced peripheral blood cytotoxic T cells (CD3, CD3+CD8+) and pro-inflammatory salivary cytokines but higher levels of autophagy-related proteins
Adults with gingivitis and Western diet conditions;30
RCT
EG: anti-inflammatory diet
CG: Western diet
PP: GI, PI, PPD, BOP, PISA
Serum 25(OH)D
EG demonstrated a significant increase in serum 25(OH)D and GI reduction compared to the CG, who had a significant increase in PPD. These effects could not be related to specific nutrients
Adults with gingivitis and carbohydrate-based diet;15
RCT
EG: anti-inflammatory diet
CG: resumed normal diet
PP: GI, PI, PPD, CAL, BOP, PISA
EG displayed a significant reduction in all inflammatory periodontal parameters to approximately half of their baseline values. No specific dietary component could be elucidated for its impact on inflammation
Daily calcium, VDS and self-administered teriparatide or placebo for 6 weeks
PP: PPD, CAL, BOP
Infrabony defect resolution
Serum 25(OH)D
Vitamin D sufficient subjects had greater CAL gain (0.92 mm vs 0.43 mm), PPD reduction (1.83 mm vs 0.43 mm) and infrabony defect resolution (2.05 mm vs 0.87 mm) compared to vitamin D deficient subjects. Teriparatide subjects had no significant improvements in CAL and PPD
Individuals who required periodontal surgery received daily calcium and vitamin D and either self-administered teriparatide (synthetic parathyroid hormone) or a placebo. Greater clinical attachment level (CAL) gain and PPD reduction were evident in the vitamin D sufficient subjects compared to deficient subjects. Teriparatide-treated vitamin D sufficient subjects showed greater infrabony defect resolution.7
Considering all three studies, it can be speculated that vitamin D can positively affect treatment outcomes of periodontal therapy – whether surgical or not. Enhancing vitamin D levels via supplementation or diet can demonstrate improved periodontal health outcomes. Although the sole effect of vitamin D in a deficient population cannot be explained in such studies, it can be hypothesized that synergistic mechanisms between vitamin D and other supplements and nutrients could have resulted in the host immunomodulatory changes evident to prevent onset or progression of periodontitis. Yet, studies examining serum 25(OH)D levels, a biologically inactive marker, allow for potential confounding because it is an indicator of supply rather than function. The same oral dose of vitamin D supplementation results in wide interindividual variability of 25(OH)D, some of which may be accounted for by polymorphisms of specific genes in the vitamin D metabolic pathway.43 Therefore, studies investigating a biologically active marker may be more apt.
Clinical guidelines
The European Federation of Periodontology (EFP) workshop from 2011 confirmed the inverse correlation between vitamin D and periodontitis, and discussed the potential for micronutritional approaches as novel periodontal therapies.44 Proceedings of the workshop recommended adequate daily intake of vitamin D, via changes in diet, lifestyle or supplements, for the prevention and treatment of periodontitis.16 Recent EFP treatment guidelines have analysed the research on the use of adjunctive agents, such as antioxidant micronutrients, in supportive periodontal care and were unable to comment on their effectiveness. Although, omega-3 polyunsaturated fatty acids were not currently recommended for use as an adjunct to subgingival instrumentation, there was no specific mention for the use of vitamin D.45
Conclusion
This article has explored the mechanisms and evidence underpinning vitamin D as a potential modifiable risk factor and host modulator for periodontitis. Further research may help to define, not only a causal relationship, but which periodontitis patients would benefit from a vitamin D screen, adding a further layer to the concept of ‘personalized medicine’.
Moreover, VDR gene polymorphisms appear to affect an individual's biological response, highlighting the potential importance of nutrigenetics. Thus, genomic approaches, more specifically genetic testing, may soon become a pragmatic approach to identify and manage at-risk individuals.
Periodontitis is a complex disease with many implications. Therefore, it is critical for dental professionals to continue to increase their understanding and awareness of nutritional deficiencies and periodontitis management. The dental team will continue to play an important role in identifying systemic issues in their patients, as well as working with appropriate medical professionals to correct them. Subsequently correcting the nutritional deficiency, although not a panacea, may be a safe, effective and inexpensive adjuvant therapy.