Albandar JM, Kingman A. Gingival recession, gingival bleeding, and dental calculus in adults 30 years of age and older in the United States, 1988–1994. J Periodontol. 1999; 70:30-43 https://doi.org/10.1902/jop.1999.70.1.30
Toker H, Ozdemir H. Gingival recession: epidemiology and risk indicators in a university dental hospital in Turkey. Int J Dent Hyg. 2009; 7:115-120 https://doi.org/10.1111/j.1601-5037.2008.00348.x
Romandini M, Soldini MC, Montero E, Sanz M. Epidemiology of mid-buccal gingival recessions in NHANES according to the 2018 World Workshop Classification System. J Clin Periodontol. 2020; 47:1180-1190 https://doi.org/10.1111/jcpe.13353
Susin C, Haas AN, Oppermann RV Gingival recession: epidemiology and risk indicators in a representative urban Brazilian population. J Periodontol. 2004; 75:1377-1186 https://doi.org/10.1902/jop.2004.75.10.1377
Jepsen S, Caton JG, Albandar JM Periodontal manifestations of systemic diseases and developmental and acquired conditions: consensus report of workgroup 3 of the 2017 World Workshop on the Classification of Periodontal and Peri-Implant Diseases and Conditions. J Clin Periodontol. 2018; 45:S219-S229 https://doi.org/10.1111/jcpe.12951
Wagner TP, Costa RS, Rios FS Gingival recession and oral health-related quality of life: a population-based cross-sectional study in Brazil. Community Dent Oral Epidemiol. 2016; 44:390-399 https://doi.org/10.1111/cdoe.12226
Seong J, Bartlett D, Newcombe RG Prevalence of gingival recession and study of associated related factors in young UK adults. J Dent. 2018; 76:58-67 https://doi.org/10.1016/j.jdent.2018.06.005
Mythri S, Arunkumar SM, Hegde S Etiology and occurrence of gingival recession – an epidemiological study. J Indian Soc Periodontol. 2015; 19:671-675 https://doi.org/10.4103/0972-124X.156881
Löe H, Anerud A, Boysen H. The natural history of periodontal disease in man: prevalence, severity, and extent of gingival recession. J Periodontol. 1992; 63:489-495 https://doi.org/10.1902/jop.1992.63.6.489
Marini MG, Greghi SL, Passanezi E, Sant'ana AC. Gingival recession: prevalence, extension and severity in adults. J Appl Oral Sci. 2004; 12:250-255 https://doi.org/10.1590/s1678-77572004000300017
Sarfati A, Bourgeois D, Katsahian S Risk assessment for buccal gingival recession defects in an adult population. J Periodontol. 2010; 81:1419-1425 https://doi.org/10.1902/jop.2010.100102
Rios FS, Costa RS, Moura MS Estimates and multivariable risk assessment of gingival recession in the population of adults from Porto Alegre, Brazil. J Clin Periodontol. 2014; 41:1098-107 https://doi.org/10.1111/jcpe.12303
Rupprecht RD, Horning GM, Nicoll BK, Cohen ME. Prevalence of dehiscences and fenestrations in modern American skulls. J Periodontol. 2001; 72:722-729 https://doi.org/10.1902/jop.2001.72.6.722
Kajan ZD, Seyed Monir SE, Khosravifard N, Jahri D. Fenestration and dehiscence in the alveolar bone of anterior maxillary and mandibular teeth in cone-beam computed tomography of an Iranian population. Dent Res J (Isfahan). 2020; 17:380-387
Delli K, Livas C, Sculean A Facts and myths regarding the maxillary midline frenum and its treatment: a systematic review of the literature. Quintessence Int. 2013; 44:177-187 https://doi.org/10.3290/j.qi.a28925
Rasperini G, Acunzo R, Cannalire P, Farronato G. Influence of periodontal biotype on root surface exposure during orthodontic treatment: a preliminary study. Int J Periodontics Restorative Dent. 2015; 35:665-675 https://doi.org/10.11607/prd.2239
Kim DM, Neiva R. Periodontal soft tissue non-root coverage procedures: a systematic review from the AAP Regeneration Workshop. J Periodontol. 2015; 86:S56-72 https://doi.org/10.1902/jop.2015.130684
Richman C. Is gingival recession a consequence of an orthodontic tooth size and/or tooth position discrepancy? ‘A paradigm shift’. Compend Contin Educ Dent. 2011; 32:e73-79
Tepedino M, Franchi L, Fabbro O, Chimenti C. Post-orthodontic lower incisor inclination and gingival recession-a systematic review. Prog Orthod. 2018; 19 https://doi.org/10.1186/s40510-018-0212-6
Pernet F, Vento C, Pandis N, Kiliaridis S. Long-term evaluation of lower incisors gingival recessions after orthodontic treatment. Eur J Orthod. 2019; 41:559-564 https://doi.org/10.1093/ejo/cjy086
Pandis N, Vlahopoulos K, Madianos P, Eliades T. Long-term periodontal status of patients with mandibular lingual fixed retention. Eur J Orthod. 2007; 29:471-476 https://doi.org/10.1093/ejo/cjm042
Gebistorf M, Mijuskovic M, Pandis N Gingival recession in orthodontic patients 10 to 15 years posttreatment: a retrospective cohort study. Am J Orthod Dentofacial Orthop. 2018; 153:645-655 https://doi.org/10.1016/j.ajodo.2017.08.020
Koke U, Sander C, Heinecke A, Müller HP. A possible influence of gingival dimensions on attachment loss and gingival recession following placement of artificial crowns. Int J Periodontics Restorative Dent. 2003; 23:439-445
Orkin DA, Reddy J, Bradshaw D. The relationship of the position of crown margins to gingival health. J Prosthet Dent. 1987; 57:421-424 https://doi.org/10.1016/0022-3913(87)90006-0
Valderhaug J. Periodontal conditions and carious lesions following the insertion of fixed prostheses: a 10-year follow-up study. Int Dent J. 1980; 30:296-304
da Fonte Porto Carreiro A, de Carvalho Dias K, Correia Lopes AL Periodontal conditions of abutments and non-abutments in removable partial dentures over 7 years of use. J Prosthodont. 2017; 26:644-649 https://doi.org/10.1111/jopr.12449
Heasman PA, Holliday R, Bryant A, Preshaw PM. Evidence for the occurrence of gingival recession and non-carious cervical lesions as a consequence of traumatic toothbrushing. J Clin Periodontol. 2015; 42:S237-255 https://doi.org/10.1111/jcpe.12330
King EM, Brewer E, Brown P. A guide to oral piercings. BDJ Team. 2018; 5
Hennequin-Hoenderdos NL, Slot DE, Van der Weijden GA. The incidence of complications associated with lip and/or tongue piercings: a systematic review. Int J Dent Hyg. 2016; 14:62-73 https://doi.org/10.1111/idh.12118
O'Halloran A, MacCarthy D. Oral and peri-oral piercings: impact on the gingival tissues. J Ir Dent Assoc. 2021; 67:150-155
Vilchez-Perez MA, Fuster-Torres MA, Figueiredo R Periodontal health and lateral lower lip piercings: a split-mouth cross-sectional study. J Clin Periodontol. 2009; 36:558-563 https://doi.org/10.1111/j.1600-051X.2009.01431.x
Lucavechi T, Barbería E, Maroto M, Arenas M. Self-injurious behavior in a patient with mental retardation: review of the literature and a case report. Quintessence Int. 2007; 38:e393-398
Tatakis DN, Milledge JT. Severe gingival recession in trisomy 18 primary dentition. A clinicopathologic case report of self-inflicted injury associated with mental retardation. J Periodontol. 2000; 71:1181-1186 https://doi.org/10.1902/jop.2000.71.7.1181
Gándara-Rey JM, Diniz-Freitas M, Gandara-Vila P Lesions of the oral mucosa in cocaine users who apply the drug topically. Med Oral. 2002; 7:103-107
Kapila YL, Kashani H. Cocaine-associated rapid gingival recession and dental erosion. A case report. J Periodontol. 1997; 68:485-488 https://doi.org/10.1902/jop.1997.68.5.485
Baker DL, Seymour GJ. The possible pathogenesis of gingival recession. A histological study of induced recession in the rat. J Clin Periodontol. 1976; 3:208-219 https://doi.org/10.1111/j.1600-051x.1976.tb00040.x
da Fonseca MA, Murdoch-Kinch CA. Severe gingival recession and early loss of teeth in a child with chronic graft versus host disease: a case report. Spec Care Dentist. 2007; 27:59-63 https://doi.org/10.1111/j.1754-4505.2007.tb00329.x
Van der Veken D, De Haes P, Hauben E A rare cause of gingival recession: morphea with intra-oral involvement. Oral Surg Oral Med Oral Pathol Oral Radiol. 2015; 119:e257-264 https://doi.org/10.1016/j.oooo.2015.02.002
Fan J, Caton JG. Occlusal trauma and excessive occlusal forces: narrative review, case definitions, and diagnostic considerations. J Periodontol. 2018; 89:S214-S222 https://doi.org/10.1002/JPER.16-0581
Jati AS, Furquim LZ, Consolaro A. Gingival recession: its causes and types, and the importance of orthodontic treatment. Dental Press J Orthod. 2016; 21:18-29 https://doi.org/10.1590/2177-6709.21.3.018-029.oin
Miller PD. Miller classification of marginal tissue recession revisited after 35 years. Compend Contin Educ Dent. 2018; 39:514-520
Cairo F, Nieri M, Cincinelli S The interproximal clinical attachment level to classify gingival recessions and predict root coverage outcomes: an explorative and reliability study. J Clin Periodontol. 2011; 38:661-666 https://doi.org/10.1111/j.1600-051X.2011.01732.x
Chrysanthakopoulos NA. Gingival recession: prevalence and risk indicators among young greek adults. J Clin Exp Dent. 2014; 6:e243-249 https://doi.org/10.4317/jced.51354
Checchi L, Daprile G, Gatto MR, Pelliccioni GA. Gingival recession and toothbrushing in an Italian School of Dentistry: a pilot study. J Clin Periodontol. 1999; 26:276-280 https://doi.org/10.1034/j.1600-051x.1999.260502.x
Nguyen-Hieu T, Ha Thi BD, Do Thu H, Tran Giao H. Gingival recession associated with predisposing factors in young vietnamese: a pilot study. Oral Health Dent Manag. 2012; 11:134-144
Müller HP, Stadermann S, Heinecke A. Gingival recession in smokers and non-smokers with minimal periodontal disease. J Clin Periodontol. 2002; 29:129-136 https://doi.org/10.1034/j.1600-051x.2002.290207.x
Miller PD A classification of marginal tissue recession. Int J Periodontics Restorative Dent. 1985; 5:8-13
Mahajan A. Mahajan's modification of the Miller's classification for gingival recession. Dent Hypotheses. 2010; 1:45-49
Rotundo R, Mori M, Bonaccini D, Baldi C. Intra- and inter-rater agreement of a new classification system of gingival recession defects. Eur J Oral Implantol. 2011; 4:127-133
Kumar A, Masamatti SS. A new classification system for gingival and palatal recession. J Indian Soc Periodontol. 2013; 17:175-181 https://doi.org/10.4103/0972-124X.113065
Gingival recession affects more than half of the population and has a multifactorial aetiology. Despite this, the knowledge and awareness of the factors that predispose sites to recession remains limited, with most people associating it with poor oral hygiene. As patients retain their teeth for longer, the risk of recession is likely to grow, thus increasing the need to establish a greater understanding of this very common condition. This two-part series provides a contemporary overview of the condition with the first article discussing its prevalence, aetiology and classification, and the second covering the different management options.
CPD/Clinical Relevance: It is important to establish the aetiology of gingival recession to manage the condition effectively.
Article
Gingival recession affects more than 50% of the population, across all age groups, with almost all middle to older aged people exhibiting the condition.1–4 It has a multifactorial aetiology and is defined, in broad terms, as the migration of the gingival margin apical to the cemento-enamel junction (CEJ), with the distance between the two giving a measure of the recession. This definition was modified in 2017 by the World Workshop to ‘an apical shift of the gingival margin caused by different conditions/pathologies’ and can apply to any surface of the tooth.5 Gingival recession is often an incidental finding, rarely causes symptoms and can affect one or more teeth. Although considered a silent condition, it has been reported that gingival recession can negatively influence quality of life by causing physical pain and psychological discomfort.6 This is the first of two articles that address the prevalence and aetiology of gingival recession, along with the different classification systems used to define it.
Prevalence of gingival recession
The prevalence of gingival recession varies in different populations and is influenced by age, with the overall prevalence ranging from 58% to 99.7%.1–4,7,8 The reported differences in the variation across different populations are influenced by the geographic distribution of the population, variable socio-economic and educational status, as well as the way in which the recession is measured (Table 1).
Gender has been identified as a significant factor when considering gingival recession, with males more affected than females.1,9,10 Recession can develop at a very young age and can progressively worsen over time. The degree by which the recession progresses is population dependent, for example 100% of 40-year-old Sri Lankans were reported to have recession when compared to 90% of 50-year-old Norwegians.11
Almost any teeth present can be affected by gingival recession with it seen more frequently in the mandible when compared to the maxilla.10–12 The teeth most commonly affected are considered to be the mandibular incisors.8,10,11
The severity of gingival recession can be grouped into mild (up to 1 mm), moderate (1–3 mm) and severe (4 mm and over).12 The majority of the population has been shown to experience at least one mild site, with studies suggesting up to 30% experiencing moderate recession. Others have shown that 5.9–40.7% of the population experiences severe recession, with the variance being related to different countries.13,14 Buccal surfaces of the teeth are the most commonly affected, especially in young people, followed by the lingual and interproximal surfaces.11 Multiple factors can affect the initiation and development of the recession which are discussed below.
Aetiology
Gingival recession has a multifactorial aetiology with a predominance of factors that play a role in its development. A healthy mucogingival complex, as shown in Figure 1, is made up of free and attached gingivae, mucogingival junction and alveolar mucosa. It is essential to maintain the health of the attachment to the teeth. When this complex is disrupted, it can present as a closed disruption, through pocket formation, or through an open disruption, leading to cleft formation or recession.11 The factors that cause this can be categorized into either predisposing or precipitating risk factors (Table 2). Predisposing factors will usually place the gums at risk of developing recession and usually include anatomical factors, such as bone dehiscence, tooth malposition, thin gingival tissue biotype, high frenal attachments and a lack of keratinized tissue. Precipitating factors, on the other hand, increase the risk of the recession developing, and include traumatic tooth brushing, dental treatment (orthodontic and restorative), poor plaque control, piercings and self-inflicted trauma. While the precipitating factors will increase the chance of the recession developing, there would have to be underlying predisposing factors present for the recession to develop.
Figure 1. A healthy mucogingival complex made up of free and attached gingivae, mucogingival junction and alveolar mucosa.
Table 2. Predisposing and precipitating risk factors for gingival recession.
Predisposing factors
Precipitating factors
Anatomical
Tooth position
Lack of keratinized tissue
Gingival tissue biotype
Frenal pull
Bone dehiscence
Iatrogenic
Smoking
Tooth movement
Restorative factors
Plaque
Traumatic
Piercings
Toothbrush trauma
Self-inflicted injury
Pathogenic
Occlusal trauma
Periodontal disease
Mucosal isorders
Predisposing risk factors
Anatomical
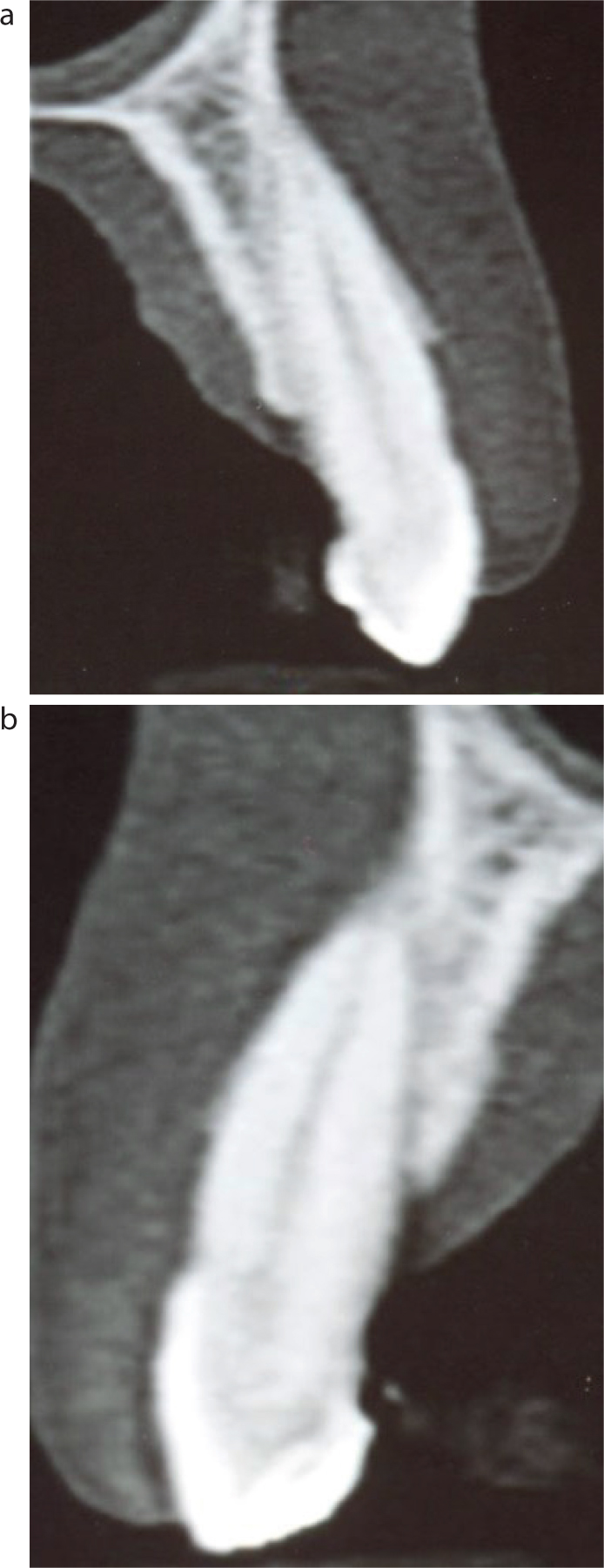
Bone dehiscence. A bone dehiscence is characterized by a missing buccal plate where the alveolar crestal margin is located apically. In contrast, a fenestration is where there is a window of missing bone on the buccal surface with the alveolar bone margins intact (Figures 2 and 3). Studies have shown up to 40% of adults will have a dehiscence, with the most commonly affected teeth being the canines, and up to 62% will have fenestrations.15 Dehiscences are also reported to affect the buccal aspects of the teeth, most frequently the coronal third of the tooth, which could explain why the buccal surfaces of the teeth are more commonly affected by recession (Figures 2 and 3).16
Figure 2. A dehiscence (upper left first premolar) and fenestration (upper left first molar) on a dry skull.Figure 3. (a,b) Radiographic demonstration of bony dehiscence.
Tooth position. Malocclusions and malalignment of teeth lead to an unfavourable position of the root in the alveolar bony housing. Usually in these patients, the alveolar bone at the crest is either void or thin, especially buccally, thus increasing the risk of gingival recession developing.9,17,18 The tooth position is also important because it influences the quality of the gingival tissue biotype (Figure 4).
Figure 4. Buccally positioned upper left canine with thin gingival tissue biotype and associated recession. There is a lack of keratinized tissue.
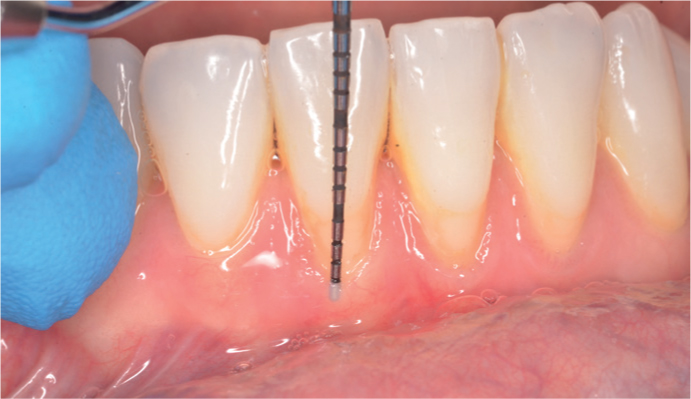
Gingival tissue biotype. The different biotypes of gingival tissues have been described using the anatomical characteristics of the mucogingival complex. This includes a description of the gingival tissue thickness and has been described in three categories – thin scalloped, thick flat and thick scalloped.19 The thin scalloped has a narrow zone of keratinized tissue with thin gingival tissue and thin alveolar bone. The thick flat biotype usually has a broad zone of keratinized tissue and thick alveolar bone, and the thick scalloped has a narrow zone of keratinized tissue with thick bone. The main variance in these two groups is the thickness of the underlying bone and the amount of keratinized tissue. Thin tissue has a bone thickness of approximately 0.3 mm and thick tissue that of 0.8 mm.20 Examples of the clinical appearance of thin and thick biotypes are shown in Figure 5. The thickness of the tissue is usually difficult to assess and is often measured by inserting a probe into the sulcus (Figure 6). If the probe is visible through the sulcus it is considered thin.
Figure 5. Patients with (a) thick and (b) thin gingival biotypes.Figure 6. Insertion of a periodontal probe into the gingival sulcus demonstrating shine through, and hence, a thin gingival biotype.
Lack of keratinized gingivae. Keratinized gingiva is the part of the oral mucosa that surrounds the teeth and extends from the free gingival margin to the mucogingival fold and is made up of the free and attached gingivae.21 The width of the keratinized tissue varies in the different biotypes and ranges from 2.8 mm to 5.4 mm in thin biotypes, and from 5.1 mm to 6.7 mm in the thick biotypes.20 While keratinized tissue is not essential, it has been reported that a minimum thickness of 2 mm is necessary to maintain periodontal health and without this, recession may occur (Figure 7).5
Figure 7. Thin gingival tissue biotype and lack of keratinized tissue buccal to the lower anteriors. The lower left central incisor also has gingival recession with the tooth being slightly rotated.
High frenal attachment. Frenal attachments are fibrous collagenous tissue folds that connect the lip to the alveolar process, and when positioned too close to the gingival margin, often affect a person's ability to maintain an optimal level of plaque control. This, along with the possible mechanical retraction of the gingival tissue, is thought to contribute to the development of recession (Figure 8). While the latter has been hypothesized, it is more likely that frenal presence impairs the ability to maintain oral hygiene leading to inflammation and subsequent recession.22,23
Figure 8. A high frenal attachment with no keratinized tissue contributing to gingival recession.
Precipitating factors
Iatrogenic
Orthodontic tooth movement. This does not inherently cause gingival recession as usually the induced tooth movement is undertaken within the boundaries of the alveolar complex. However, in cases with underlying predisposing anatomical factors, the recession occurs because the tooth movement induces changes in the bone morphology (Figure 9). Therefore, if there is a thin buccal plate, or dehiscence, along with thin gingival tissue biotype, high muscle attachment and a malpositioned tooth, the risk of gingival recession developing becomes greater.24–27 Others have reported that fixed orthodontic retainers may induce gingival recession post-treatment; however, it is more likely that this is related to the type of retainer (fixed or removable) and the plaque retention around this resulting in inflammation characteristic of periodontal disease.28,29 The effects of occlusal trauma caused by a deep overbite whereby the lower incisor teeth cause stripping of the gingival tissues palatal to the maxillary incisors can also induce recession with soreness often expressed by patients owing to the secondary inflammation of the gingival tissues.30
Figure 9. Presence of gingival recession affecting a number of lower anterior teeth following orthodontic tooth movement. The root position out of the alveolar housing is evident
Orthodontic tooth movement can, in some cases, assist in improving the severity of the gingival recession by moving the tooth into a more favourable position within the alveolar housing.31 Gebistorf et al demonstrated that patients with orthodontically treated malocclusion exhibited less gingival recession 10–15 years post-treatment when compared to those with an untreated malocclusion.31
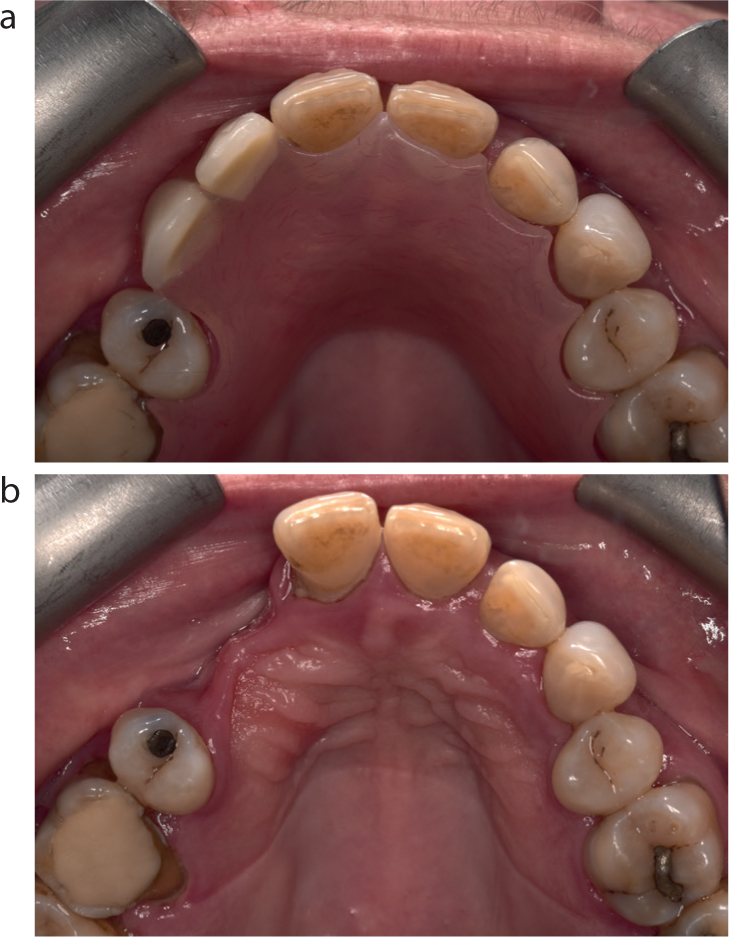
Restorative treatment. Restorative treatment, particularly in the presence of predisposing factors, such as overhangs and subgingival restoration margins, can lead to gingival recession by damaging the gingival complex both during and after treatment. This is seen particularly in patients with thin gingival tissue biotype when subgingival restorations encroach on the biological width.5,32 The gingival tissue biotype should therefore be assessed prior to any fixed prosthetic treatment, especially when subgingival margins are being considered. If the tissues are thin, then either supragingival or equigingival margins should be considered to minimize the risk of gingival recession.33,34 Poorly designed dentures, the so called ‘gum strippers’, also cause recession by trauma to the gingival tissues that is exacerbated in the presence of poor plaque control (Figure 10).35 Poorly designed denture clasps, especially gingivally approaching clasps, can also lead to recession over time on the abutment teeth. Thus, the need for well-designed dentures with attention to the gingival tissue biotype should not be underestimated.35
Figure 10. (a,b) A poorly designed denture in the presence of poor plaque control leading to recession on the palatal surface of the upper right central incisor. The presence of gingival inflammation is also evident around the other teeth.
Traumatic
Traumatic tooth brushing. This is often seen in patients who are overzealous with their brushing, with trauma associated with the incorrect use of oral hygiene aids. It is theorized that the repeated trauma physically injures the gingival tissues progressively, causing gingival recession over time. The direct relationship between traumatic homecare regimens and gingival recession is inconclusive. Although most short-term studies suggest an association between gingival trauma and abrasion, there are no long-term studies that support the notion of gingival recession developing following toothbrush trauma.5,36 If, however, there are underlying predisposing factors, then it seems logical that traumatic tooth brushing could contribute to the occurrence of gingival recession (Figure 11).
Figure 11. Gingival recession affecting the lower left premolars and molars because of toothbrush abrasion. The trauma on the gingival tissue is evident on the mesial of LL5.
Piercings. Tongue and lip piercings are the most common site for oral piercing, with 43% being placed in the tongue, and 33% in the lip.37 The incidence of gingival recession is reported to be 44% in people with tongue piercing and 50% in those with lip piercing, with the latter being at a four-times higher risk of recession than those without a piercing.38 Overall, 68–80% of lip piercings have been associated with gingival recession owing to the intra-oral position of the ‘stud’ of the piercing.39 This constantly traumatizes the labial mucosal tissues, with the severity of recession being dependent on the degree of keratinized tissue present, and the quality of the gingival tissue biotype.40 In comparison, tongue piercings have been associated with a higher prevalence of lingual recession, which ranged from 3% to 33%.39 This is thought to be related to the trauma caused by the ‘dumbbell’ during protrusion of the tongue.
Self-inflicted injury. These injuries are repetitive acts that cause physical damage to the gingivae usually in the form of scratching, rubbing or picking the gingivae using a fingernail or abrasive objects and are more common in children, especially females.41,42 The local application of cocaine to the gingival tissues has also been associated with localized gingival recession.43,45 These cases are difficult to manage owing to the complex underlying social and medical issues, and early intervention often helps minimize the risk of progression.
Pathogenic
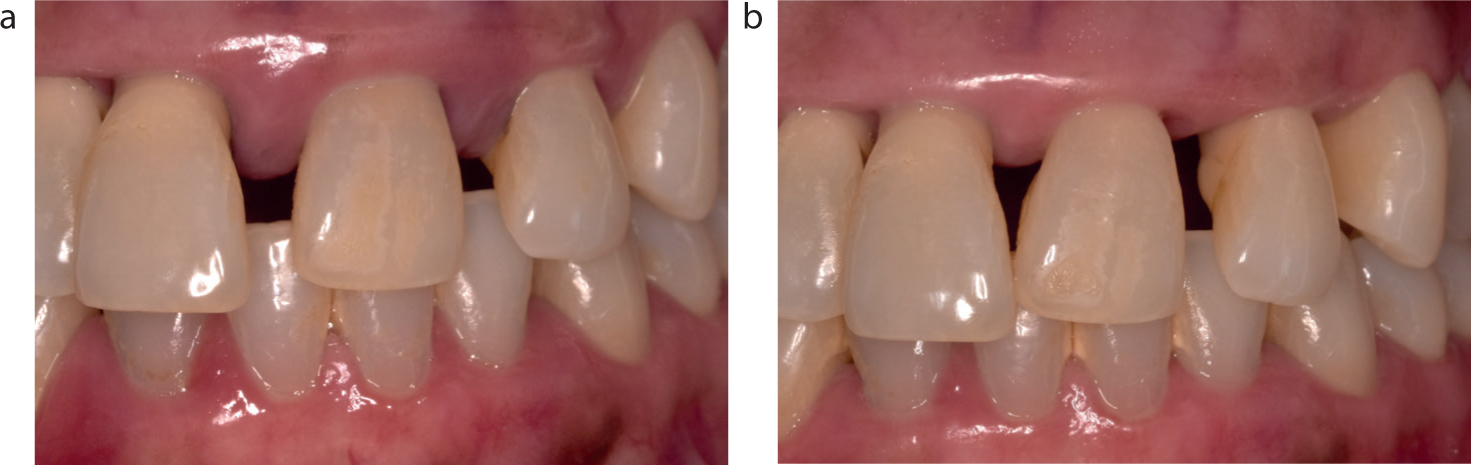
Periodontal disease. If left untreated, periodontal disease ultimately results in bone loss and gingival recession. The disease, once initiated and if not managed, results in the apical migration of the gingival tissues with pocket formation, the so called, closed destruction of the mucogingival complex.11 The pathogenesis of the disease results in bone resorption related to the inflammatory process affecting the alveolus, with the recession often being masked by the tissue inflammation and oedema (Figure 12). Untreated, the disease progresses, which results in gingival tissue recession. However, even if treatment is initiated, once the inflammation is eliminated, there is a retraction of the gingival tissues with root surface exposure as the gingival tissues adopt a healthier position. Surgical forms of treatment also lead to recession, the extent of which is dependent on the type of procedure being undertaken. While bacterial plaque is the causative factor of periodontal disease, risk factors for periodontal disease, such as smoking and diabetes, have also been associated with a higher risk of recession developing.23,45,46
Figure 12. (a,b) Patient with gingival recession masked by oedema before and after non-surgical periodontal therapy.
Oral mucosal disorders. These disorders are autoimmune and per se, will not cause the gingival recession; however, the condition affects the patient's ability to perform optimal plaque control, thereby generating an inflammatory reaction. Additionally, these patients may have thin quality gingival biotype, lack of keratinized tissue and underlying bone dehiscences, which, as discussed earlier, contribute to the condition. Specifically, gingival recession has been reported as a consequence of graft versus host disease and morphea.47,48
Occlusal trauma. Historical studies suggested that gingival recession may be induced by excessive occlusal force, although more recent evidence does not support this.49 If this were to contribute, the extent of the contribution would be dependent on the thickness of the buccal/cortical bone plate. In the presence of buccal dehiscences, the classical V-shaped defect may be seen in these cases, which anecdotally may often be associated with abfraction and recession.50
Classification of gingival recession
Classifications have been used to aide communication, but also as decision-making tools for the clinician when considering the best course of action when taking into account the multiple factors that may influence the outcome. The multifactorial aetiology of gingival recession can make the management of the condition challenging; however, with careful consideration of the aetiological factors, the outcome to treatment can be successful.
Table 3 shows the different classification systems used to describe gingival recession. Most are complicated to use, relying on defining the recession using objective criteria, including an assessment of gingival tissue thickness. Miller's classification system (1985, 2011, 2018) uses the extent of the recession, in relation to the mucogingival fold, in conjunction with presence of hard and soft tissue interdentally (see Table 4).51,52
Comparing mid buccal attachment loss to the interproximal attachment loss and whether this is greater or lesser. This directly correlates to whether root coverage is achievable
The 2017 World Workshop uses the Cairo classification of 2011
Table 4. Miller's classification (2018).
Class I Marginal tissue recession, which does not extend to the mucogingival junction (MGJ)There is no periodontal loss (bone or soft tissue) in the interdental area 100% root coverage can be anticipated
Class II Marginal tissue recession, which extends to or beyond the MGJThere is no periodontal loss (bone or soft tissue) in the interdental area 100% root coverage can be anticipated
Class III Marginal tissue recession, which extends to or beyond the MGJBone or soft tissue loss in the interdental area is present or there is a malpositioning of the teeth (including extrusion)100% coverage difficult with partial root coverage anticipated. The amount of root coverage can be determined pre-surgically using a periodontal probe
Class IV Marginal tissue recession, which extends to or beyond the MGJThe bone or soft tissue loss in the interdental area and/or malpositioning of teeth is so severe, root coverage cannot be anticipated
Until 2018 when the World Workshop introduced the new classification, this was the most commonly used classification for gingival recession. The new classification combines Miller's Class I and II into a single category, and uses the interdental clinical attachment loss as the descriptor, measuring the attachment loss to the apical limit (Table 5). While aimed at making the classification simpler, it does not take into consideration the extent of keratinized tissue present, which could influence the choice of treatment.
Table 5. World Workshop Classification for Gingival Recession (2018). The probe is used to demonstrate the difference in attachment loss buccally compared to interproximally.
Recession type 1 (RT1) Gingival recession with no loss of interproximal attachmentInterproximal CEJ is clinically not detectable at both mesial and distal aspects of the tooth
Recession type 2 (RT2) Gingival recession associated with loss of interproximal attachmentThe amount of interproximal attachment loss (measured from the interproximal CEJ to the depth of the interproximal sulcus/pocket) is less than or equal to the buccal attachment loss (measured from the buccal CEJ to the apical end of the buccal sulcus/pocket)
Recession type 3 (RT3) Gingival recession associated with loss of interproximal attachmentThe amount of interproximal attachment loss (measured from the interproximal CEJ to the apical end of the sulcus/pocket) is higher than the buccal attachment loss (measured from the buccal CEJ to the apical end of the buccal sulcus/pocket)
More recently, Cortellini and Bissada20 undertook a systematic review that outlined the multifactorial issues that influence the diagnosis and management of gingival recession and outline a novel treatment-oriented classification that takes into consideration the gingival tissue biotype, the gingival recession severity and associated cervical lesions to assist the clinicians' decision-making process using a 4 x 5 matrix (Table 6). The classification is based on two groups:
Group 1: no recession Based on the assessment of the gingival tissue biotype, the gingival tissue thickness and width of the keratinized tissue either in single site or the whole mouth. This is then further divided into Case A, with thick gingival tissue biotype, and Case B, with thin gingival tissue biotype, and the modality of monitoring described.
Group 2: recession present Based on a treatment-oriented approach using the interdental clinical attachment level score described by Cairo et al (RT1-3).53 These are further quantified by measurements of the recession depth (distance from the cemento-enamel junction to the free gingival margin), gingival tissue thickness, keratinized tissue width (distance from the free gingival margin to the mucogingival fold) and root surface condition (i.e. abrasion present or not). Other factors such as tooth position, cervical wear, and adjacent recessions are also recorded. Depending on the assessment analysis, the management is divided into case C, where a conservative attitude is adopted, or case D where a treatment-orientated approach is adopted influenced by the patient's complaint.
Table 6. The 4 x 5 matrix proposed by Cortellini and Bissada.20
Gingival site
Tooth site
REC depth
GT
KTW
CEJ (A/B)
Step (+/-)
No recession
RT1
RT2
RT3
RT: recession type; REC depth: depth of the gingival recession; GT: gingival thickness; KTW: keratinized tissue width; CEJ: cemento-enamel junction (Class A: detectable CEJ; Class B: undetectable CEJ); Step: root surface concavity (Class +: presence of a cervical step >0.5 mm; Class -: absence of cervical step).
This classification is the first of its kind where an assessment of all the factors, predisposing and precipitating, are considered when making the decision of how best to manage the recession. However, its use in daily practice can be challenging and Miller's classification, along with the 2018 classification, remain the more popular ways of classifying gingival recession.
Conclusion
This article highlights the difficulties that clinicians often face when assessing gingival recession and provides an overview of its prevalence and multifactorial aetiology. The need to take these factors into consideration is highlighted, and the challenges with the different classification systems that have been used highlights the importance of using objective criteria, along with the different prognostic factors that may influence treatment outcome. The second article will focus on the management of gingival recession and the decision-making process to optimise treatment outcomes.