Bauss O, Rohling J, Schwestka-Polly R Prevalence of traumatic injuries to the permanent incisors in candidates for orthodontic treatment. Dent Traumatol. 2004; 20:61-66
Andreasen FM Pulpal healing after luxation injuries and root fracture in the permanent dentition. Endod Dent Traumatol. 1989; 5:111-131
Flores MT, Andersson L, Andreasen JO, Bakland LK, Malmgren B, Barnett F Guidelines for the management of traumatic dental injuries. 1. Fractures and luxations of permanent teeth. Dent Traumatol. 2007; 23:66-71
Andreasen JO, Andreasen FM, Mejare I, Cvek M Healing of 400 intra-alveolar root fractures. 2. Effect of treatment factors such as treatment delay, repositioning, splinting type and period and antibiotics. Dental Traumatol. 2004; 20:203-211
Andreasen JO, Andreasen FM, Mejare I, Cvek M Healing of 400 intra-alveolar root fractures. 1. Effect of pre-injury and injury factors such as sex, age, stage of root development, fracture type, location of fracture and severity of dislocation. Dent Traumatol. 2004; 20:192-202
Welbury R, Kinirons MJ, Day P, Humphreys K, Gregg TA Outcomes for root-fractured permanent incisors: a retrospective study. Paediatr Dent. 2002; 24:98-102
Andreasen JO, HjØrting-Hansen E Intra-alveolar root fractures: radiographic and histologic study of 50 cases. J Oral Surg. 1967; 25:414-426
Kindelan SA, Day PF, Kindelan JD, Spencer JR, Duggal MS Dental trauma: an overview of its influence on the management of orthodontic treatment. Part 1. J Orthod. 2008; 35:68-78
Heling I, Slutzky-Goldberg I, Lustmann J, Ehrlich Y, Becker A Bone-like tissue growth in the root canal of immature permanent teeth after traumatic injuries. Endod Dent Traumatol. 2000; 16:298-303
A case series: the orthodontic management of central incisors with horizontal root fractures Louise C Kneafsey Samantha J Hodges Dental Update 2024 43:7, 707-709.
Senior Specialist Registrar Orthodontics, Orthodontic Unit, Division of Craniofacial and Development Sciences, Eastman Dental Hospital/Institute, 256 Gray's Inn Road, London WC1X 8LD, UK
This case series illustrates the successful orthodontic management of previously root-fractured central incisors. Orthodontic treatment was carried out to correct the underlying malocclusion, remove traumatic occlusal forces and to provide a suitable occlusion for future restorative treatment should the root-fractured teeth be lost in the future.
CPD/Clinical Relevance: Dental trauma occurs commonly; having affected 10% of orthodontic patients. All practitioners should be able to discuss the possibility of orthodontic treatment with patients who have had previous trauma to their front teeth.
Article
The percentage of the population presenting for orthodontic treatment with previous dental trauma has been reported to be as high as 10.3%.1 Root fractures in the permanent dentition account for 0.5–7% of all dental trauma2 and usually occur as a result of direct horizontal impact to the tooth or jaws.
Root fractures are most commonly seen in males in the 11–20 years age group and predominantly affect the middle third of the root of the upper incisors.2,3 Commonly, the root-fractured tooth presents with slight extrusion because the direction of impact tends to force the coronal fragment palatally, and the pulp can be stretched or severed. Pulp necrosis occurs in 20–44% of cases.2
Root fractures can be classified according to:
The direction in which they occur (horizontal or vertical);
The number of fracture lines (simple or multiple);
The location of the root affected (cervical, middle third or apical).
Horizontal root fractures are more likely in the permanent dentition when teeth have closed apices.2 The International Association of Dental Traumatology (IADT) recommends splinting teeth with a root fracture for 4 weeks with a flexible splint, unless the root fracture is near the cervical area of the tooth when it may benefit from a longer period of splinting (up to 4 months).4 Horizontal fractures in the middle third of the root have a better prognosis than vertical fractures.
Root fracture healing
There are different types of fracture healing dependent upon the stage of root formation, patient's age, tooth mobility and location of the root fracture.5,6 The apical fragment remains vital in the majority of cases, even if the coronal part becomes non-vital. Andreasen postulates that, as the distance between the fragments increases, the chance of pulp necrosis increases.3 This is also discussed by Welbury et al in their retrospective study.7 The ideal repair process involves the pulpal tissues and results in the formation of hard tissue between the two fragments creating a functional unit with normal mobility and pulpal vitality. However, most commonly, healing begins in the periodontal ligament with interposition of connective tissue between the fragments.6
Andreasen and Hjørting-Hansen8 have classified root fracture healing into 4 groups:
Type 1 with hard calcified tissue;
Type 2 with interposition of hard and soft tissue (connective and calcified tissue);
Type 3 with interposition of soft tissue;
Type 4 no healing.
Orthodontic management depends on the type of healing at the root fracture site. If the fracture has healed with a hard tissue callus (Type 1 healing), the tooth may be treated in the same way as a previously traumatized but non-fractured tooth with no expectation of separation of the fragments. Orthodontic movement of a root-fractured tooth, which has healed with the interposition of connective tissue, can lead to further separation of the fragments; the orthodontic treatment of these teeth must be evaluated with respect to the length of the coronal fragment and should be looked upon as a tooth with a short root.
The hard tissue union of fractured root fragments cannot be diagnosed clinically earlier than three months after injury and may take several years to be completed.5 Root resorption can usually be detected within the first year after injury and precedes fracture healing and obliteration of the apical and/or coronal portions of the root canals. This includes external surface resorption, internal surface resorption and internal tunnelling resorption. Resorption processes are all self-limiting, usually resolving within 1–2 years after the injury, and require no interceptive treatment.6
Orthodontic management
Orthodontic treatment of root-fractured incisors is not without complications. However, patients may still benefit from orthodontic treatment for the following reasons:
Correction of the underlying malocclusion to improve function, aesthetics and associated psychosocial factors.
Relief of traumatic occlusion: the traumatic forces may continue to separate the root fragments causing further mobility or root resorption.
To facilitate future restoration and/or replacement of root-fractured poor prognosis teeth or absent teeth. A preexisting malocclusion may compromise prosthodontic replacement if root-fractured teeth are lost, for example crowding can cause insufficient space for a replacement tooth or a deep bite may limit the interocclusal space. Alternatively, the malocclusion may be secondary to the root fracture. For example, displacement of the coronal fragment of the root-fractured tooth can result in tipping of the adjacent teeth, with space loss and insufficient space for a replacement tooth.
Andreasen suggests that teeth with fractures in the apical third of the root generally have enough periodontal support to allow orthodontic movement. Teeth with a fracture located in the middle third of the root represent a hazard to tooth integrity because of the risk of further shortening of the already short coronal fragment, which would result in very little periodontal support.2 However, with informed consent and careful orthodontic management, orthodontic treatment of teeth with a mid-third root fracture can successfully enable patients to have their malocclusion corrected. This will help ensure that any future prosthodontic work should not be compromised by a malocclusion.
The recommended post injury ‘observation period’ for root-fractured teeth before undertaking orthodontic treatment or continuing active orthodontic treatment depends upon the type of healing (Table 1).4,9
Type of Healing
Recommended Observation Period
Considerations for Orthodontic Treatment
Type 1
12 months
At least 12 months observation is advisable to determine the pulpal status
Type 2 & 3
12–24 months
The teeth must be treated as teeth with short roots (ie light forces)
Type 4
24 months
No orthodontic movement should be undertaken
If active orthodontic treatment is to be undertaken, informed consent must be gained and the patients and parents should be warned that root resorption and/or loss of vitality may occur during the active orthodontic phase. Continued close monitoring of the tooth throughout treatment is necessary and it is important that baseline levels of pulpal and root health have been recorded so that comparisons can be made during treatment. During tooth movement, light, short-acting forces (<70 gm) should be used and treatment objectives may be limited from the start of treatment or modified if the trauma occurs during treatment. Permanent mobility of the coronal fragment can be expected where the root length is less than 9 mm.9
We describe the comprehensive orthodontic management of three cases with previously root-fractured maxillary incisors. The patients had been managed in three separate units in the immediate postoperative period, and therefore the protocol for immediate management of the root fracture varies with each case. The cases were each referred for an orthodontic assessment at different times post trauma.
Case reports
Case 1
A 17-year-old male presented with a root fracture of his upper left central incisor as a result of an alleged assault one week previously. The upper left lateral and central incisors had been laterally luxated, which the patient had attempted to reposition himself. Additionally, the central incisor remained palatally displaced. The upper right central incisor and canine had enamel fractures. The upper left central incisor was Grade I mobile, slightly tender to percussion, and weakly positive to sensitivity testing. The remaining upper incisors were positive to sensitivity testing and asymptomatic. The patient previously had a 12-month course of non-extraction fixed appliance treatment when aged 13 years.
Radiographic examination revealed a simple horizontal mid-third root fracture of the upper left central incisor. There was sclerosis of the upper right central incisor root canal: this may have been due to previous trauma. The upper left central and lateral incisors were repositioned under local anaesthetic and a 0.0175'' twistflex wire was bonded palatally from upper canine to canine.
The patient was reviewed regularly and the splint removed after 4 weeks. During this time the upper incisors remained positive to sensitivity testing, did not discolour or become ankylosed. Regular radiographic examination showed the persistence of the root fracture. At 12 months review, radiographs suggested a radiolucent area over the fracture site, which was postulated to be root remodelling or internal resorption, possibly associated with the traumatic occlusion (Figure 1a).
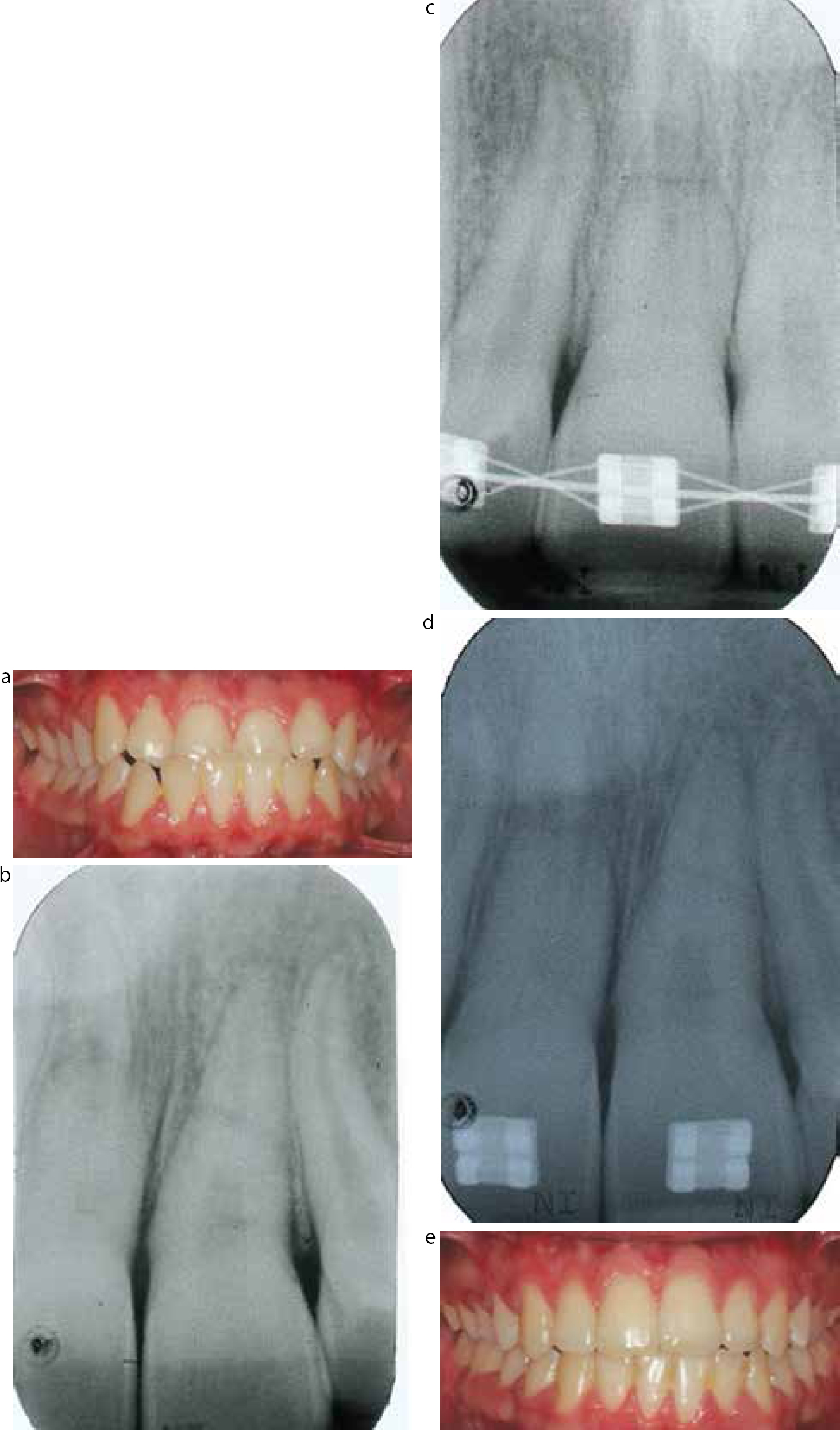
Figure 1. Case 1: (a) Peri-apical radiograph of the upper central incisors at initial orthodontic referral, 12 months post trauma. (b) Pre-treatment intra-oral anterior view. (c) Peri-apical radiograph of the upper left central incisor 3 months into fixed orthodontic treatment. (d) Peri-apical radiograph of the upper left central incisor pre-debond. (e) Post-treatment intra-oral anterior view.
At this stage the patient was referred for a further orthodontic assessment. He presented with a Class III malocclusion with mild crowding. In maximum intercuspation the upper left central incisor came into traumatic contact with the lower left lateral incisor and canine (Figure 1b). The upper left central incisor was Grade 1 mobile, non-tender to percussion and weakly positive to sensitivity testing.
Orthodontic treatment was planned with the extraction of the lower left central incisor in conjunction with upper and lower fixed orthodontic appliances to align and retrocline the lower labial segment. Alignment of the upper left central incisor required only minimal tooth movement to remove the traumatic occlusion. The patient was fully informed of the increased risk of root resorption to the upper incisors, especially the upper left central incisor.
Orthodontic treatment began 30 months post root fracture. At three months into orthodontic treatment, radiographic examination revealed that the radiolucency over the fracture site was more apparent (Figure 1c). It was postulated that this occurred as the root fragments were differently aligned, and that there was less superimposition of the root fragment with the remainder of the tooth. There did not appear to be further resorption, nevertheless it was decided that further movement of the upper left central incisor should be limited.
The upper left central incisor remained weakly positive to sensitivity testing and a pre-debond radiographic examination showed the root fracture was the same as at the start of treatment (Figure 1d). The fixed appliances were removed after 11 months and bonded retainers were fitted to the upper and lower labial segments in addition to removable retainers (Figure 1e).
The upper left central incisor was Grade I mobile at debond; however, the bonded retainer masked this. This mobility may lead to increased failures of the bonded retainer, due to increased stress on the composite bond.
The patient has been reviewed for 2 years in retention. The upper left central incisor has been asymptomatic and there has been no deterioration in response to sensitivity testing. The bonded retainer is still in situ and the patient has been advised to continue to wear the retainers for the long-term to maintain alignment.
Case 2
A 12-year-old presented with palatally displaced upper central incisors, following a blow to the mouth whilst playing softball two hours previously. The upper right central incisor was tender to percussion, Grade 1 mobile and non-responsive to sensitivity testing. The upper left central incisor was not tender to percussion, non-mobile and positive to sensitivity testing.
Radiographic examination showed a horizontal apical-third root fracture of the upper right central incisor and a horizontal mid-third root fracture of the upper left central incisor.
The teeth were repositioned under local anaesthetic; a wire splint was placed across the upper incisors and the patient given a course of metronidazole (250 mg, three times daily for 5 days). The splint was removed after four weeks.
At four weeks post trauma, the upper incisors were positive to sensitivity testing and non-tender to percussion, however, the upper right central incisor showed slight grey discoloration and maintained Grade 1 mobility. Radiographic examination showed the persistence of the root fracture of the upper right central incisor, which had increased slightly in width, suggesting resorption of both the coronal and apical fragments at the fracture line, and a slight increase in the width of the periodontal ligament, but no periapical pathology. The root fracture of the upper left central incisor had healed, and there was no periapical pathology.
At 9 months post-trauma, the patient complained of the appearance of his reverse overjet and was referred for orthodontic treatment. He presented with a Class III malocclusion with moderate upper arch crowding and a well-aligned lower arch. He could achieve an edge-to-edge incisor relationship in retruded contact position but displaced forward into a 2 mm reverse overjet (Figure 2a). The upper right central incisor was asymptomatic, non-tender to percussion, Grade I mobile and was weakly responsive to sensitivity testing. Radiographic examination confirmed the root fracture of the upper left central incisor had healed and the upper right central incisor had a persistent mid-third root fracture (Figure 2b).
Figure 2. Case 2: (a) Pre-treatment intra-oral anterior view. (b) Peri-apical radiograph of the upper central incisors at initial orthodontic referral, 9 months post trauma. (c) Peri-apical radiograph of the upper central incisors 3 months into fixed orthodontic treatment. (d) Peri-apical radiograph of the upper central incisors pre-debond. (e) Post-treatment intra-oral anterior view.
Upper and lower fixed appliances were planned to correct the malocclusion and eliminate the premature contact and associated displacement. Orthodontic treatment began 18 months post trauma and light forces (<70 gm) were maintained throughout treatment. At three months into treatment, radiographs showed the upper left central incisor had no significant resorption; however, the coronal and apical fragments of the upper right central incisor had moved apart and there was evidence of increased resorption at the fracture line (Figure 2c). The orthodontic aims were revised to limit further movement of the upper central incisors whilst completing treatment.
Orthodontic appliances were removed after 24 months. Treatment was unfortunately prolonged by poor compliance (Figure 2d). A bonded retainer was placed in the upper labial segment in addition to upper and lower removable retainers. The upper incisors remained positive to sensitivity testing. There was some increased resorption of the apical and coronal fragments of the upper right central incisor and the upper left central incisor showed no significant root resorption (Figure 2e).
The patient has been reviewed for 2 years in retention. The upper central incisors have been asymptomatic and there has been no deterioration in response to sensitivity testing.
Case 3
The patient was referred for orthodontic treatment aged 11 years, 4 years after the original trauma. This resulted in avulsion of the upper right central incisor, extrusion of the upper left central incisor and avulsion of the upper deciduous lateral incisors. She presented with a Class II division 2 malocclusion, complicated by significantly retroclined upper incisors and moderate crowding of the lower arch. The upper right lateral incisor had been allowed to drift into the central incisor position and had been restored with composite resin to resemble the central incisor (Figure 3a). Both upper and lower centrelines were shifted to the right. The upper left central incisor was positive to sensitivity testing, non-mobile, non-tender to percussion and not discoloured. The radiographs confirmed the presence of a horizontal mid-third root fracture of the upper left central incisor that appeared to have healed with interposition of hard tissue (Figure 3b). The radiographs suggest that the injury displaced the coronal fragment, leaving the atypical tooth germ in situ. This was thought to be metaplasia type healing, as described by Heling et al in 2000.10
Figure 3. Case 3: (a) Pre-treatment anterior view of study models (as clinical view not available). (b) Peri-apical radiograph of the upper left central incisor at initial orthodontic referral, 4 years post trauma. (c) Peri-apical radiograph of the upper left central incisor following removable appliance treatment. (d) Peri-apical radiograph of the upper central incisors 3 months into fixed orthodontic treatment. (e) Peri-apical radiograph of the upper left central incisor at debond. (f) Post-treatment intra-oral anterior view.
Detailed discussion of the treatment options with the patient and parent (who was a general dentist) were undertaken, including the risks and benefits of the various approaches. Comprehensive orthodontic treatment was carried out which required significant tooth movement by proclining the upper incisors to a normal inclination, creating a Class II division 1 malocclusion with an increased overjet, followed by a functional appliance to produce a Class I occlusion. Correction of the centrelines and crowding necessitated the extraction of premolars in the upper left and both lower quadrants and upper and lower fixed appliances. Loss of vitality, root resorption, mobility and potential incisor tooth loss in addition to the proposed extraction were understood to be increased risks of orthodontic treatment. The additional risk of the extraction of a healthy premolar to allow correction of malocclusion, whilst maintaining the poor prognosis of the upper right central incisor, was discussed at length. Consideration was given to replacement of the upper right central incisor, although this would have required a premolar extraction in the same quadrant to provide the space. The option of alignment without correction of the Class II division 2 malocclusion was also considered but this would still have involved a significant amount of movement of the upper left central incisor, with the aforementioned risks. This would have resulted in a compromised appearance and occlusal environment, with regards to future prosthodontic treatment of the camouflaged upper right lateral as central incisor, and replacement of the upper left central incisor should this become necessary. An optimum aesthetic result was the primary concern of the patient and her parents; therefore, the extraction of a healthy premolar in a quadrant with a poor prognosis central incisor was planned.
This approach led to considerable movement of the upper left central incisor, both in proclining the tooth to a normal inclination and in its bodily movement to correct the centreline. Long cone periapical radiographs were taken after proclination of the upper left central incisor (Figure 3c), which did not show any significant changes in the area of the root fracture. Further periapical radiographs taken 3 months into fixed appliance treatment, and at debond, show separation of the root fragments as expected and the apical root fragment superimposed on the wide apex of the coronal fragment (Figures 3d and e). An upper bonded retainer was provided as well as upper and lower removable retainers (Figure 3f). The upper left central incisor remained vital and without excessive mobility throughout orthodontic treatment and 2-year follow up.
Discussion
A minimum period of observation following trauma before commencing orthodontic treatment has been recommended by the International Association of Dental Trauma (IADT) (Table 1). The cases we present commenced active orthodontic treatment 18–30 months post trauma.
Orthodontic management depends on the type of healing at the root fracture site. If the fracture has healed with a hard tissue callus (Type 1 healing), the tooth may be treated in the same way as a previously traumatized but non-fractured tooth with no expectation of separation of the fragments, see Case 2. Orthodontic movement of a root-fractured tooth which has healed with the interposition of connective tissue (see Cases 1 and 3) can lead to further separation of the fragments. The orthodontic treatment of these teeth must be evaluated with respect to the length of the coronal fragment and should be managed as a tooth with a short root. In each case, we radiographed the affected tooth at 3 months into treatment to assess the effect of orthodontic forces on separation and resorption of fragments.
In Cases 1 and 2, the orthodontic treatment was completed whilst staying in round archwires in the upper arch to limit further movement of the root fragments. In Case 3, the root fragments showed increased separation, as expected, with the proposed tooth movement but no excessive resorption. Comprehensive treatment was carried out progressing through a standard sequence of archwires to a full size 0.019 x 0.025” stainless steel wire in both arches.
With the current evidence it is not possible to say whether orthodontic movement of traumatized teeth increases the risk of pulpal necrosis above that of uninjured teeth undergoing orthodontic tooth movement. At follow-up, all the root-fractured teeth had maintained a positive response to sensitivity testing and were not compromised by mobility or poor aesthetics.
In the long term, a root-fractured tooth with Type 2 or 3 healing (non hard tissue union) is considered as a tooth with a short root. The emphasis during orthodontic retention would be on maintaining a healthy periodontium to ensure that the remaining root had maximum support. Bonded retainers were placed for retention but had the added benefit of splinting the root-fractured tooth and so reducing the mobility.
Conclusion
Orthodontic treatment of these three cases was carried out to correct the underlying malocclusion, reduce traumatic occlusal forces and to provide a suitable occlusion for future restorative treatment should the root-fractured teeth be lost in the future. The guidelines for recommended ‘observation’ period post injury were followed and the traumatized teeth were monitored during treatment, both clinically and radiographically. The horizontally root-fractured maxillary central incisors remained functional and asymptomatic during orthodontic treatment and at 2-year follow-up.