BOS website. FAQ for children and teens. (Accessed October 2014)
Van Beek GC, 2nd edn. Oxford: Wright; 1983
Management of the unerupted maxillary incisors, RCS Eng. 2010.
Garvey MT, Barry HJ, Blake M Supernumerary teeth – an overview of classification, diagnosis and management. J Can Dent Assoc. 1999; 65:612-616
Wiedel AP, Bondemark L Fixed versus removable orthodontic appliances to correct anterior crossbite in the mixed dentition – a randomized controlled trial. Eur J Orthod. 2015; 37:123-127
Orthodontic treatment for posterior crossbites.
Balmer R, Toumba J, Godson J, Duggal M The prevalence of molar incisor hypomineralisation in Northern England and its relationship to socioeconomic status and water fluoridation. Int J Paediatr Dent. 2012; 22:250-257
Gill DS, Lee RT, Tredwin CJ Treatment planning for the loss of first permanent molars. Dent Update. 2001; 28:304-308
A Guideline for the Extraction of First Permanent Molars in Children. RCS. 2009.
Faculty Working Party.
Mandell N, DiBiase A Is early Class III protraction facemask treatment effective? A multicentre, randomized, controlled trial: 15-month follow-up. J Orthod. 2010; 37:149-161
Is early class III protraction facemask treatment effective? A multicentre, randomized, controlled trial: 3-year follow-up. J Orthod. 2012; 39:176-185
Baccetti T, Franchi L, Ratner L, McNamara JA Treatment timing for twin-block therapy. Am J Orthod Dentofacial Orthop. 2000; 118:159-170
O'Brien K Early treatment for Class II division 1 malocclusion with the Twin-block appliance: a multi-center, randomized, controlled trial. Am J Orthod Dentofacial Orthop. 2009; 135:573-579
Thiruvenkatachari B, Harrison J, Worthington H, O'Brien K Early orthodontic treatment for Class II malocclusion reduces the chance on incisal trauma: results of a Cochrane systematic review. Am J Orthod Dentofacial Orthop. 2015; 148:47-59
Kurol J Infraocclusion of primary molars: an epidemiologic and familial study. Community Dent Oral Epidemiol. 1981; 9:94-102
O'Brien MLondon: HMSO; 1993
Noar J, Portnoy S Dental status of children in a primary and secondary school in rural Zambia. Int Dent J. 1991; 41:142-148
Many of the orthodontic patients in the UK are treated in early adolescence. This occurs when most of the permanent dentition has erupted and after the general dental practitioner (GDP) has had the opportunity to assess the patient using the index of orthodontic treatment need (IOTN). There are certain types of malocclusion that present before this age and would undoubtedly benefit from earlier referral.
CPD/Clinical Relevance: To describe the malocclusion and dental anomalies that benefit from ‘early’ orthodontic assessment and active intervention.
Article
The majority of orthodontic treatment performed in the UK is undertaken when children are in their early adolescence (12–14 years old).1 The reasons for this are both patient- and health service-related. Most of the permanent dentition is erupted by 12 years of age,2 which makes complete assessment of the clinical situation possible and allows the use of full upper and lower fixed appliances. Other treatment modalities, such as the use of functional appliances, hope to ‘harness’ the growth potential of the child, and improve a moderate to severe sagittal discrepancy. Children are usually actively growing as they reach the final stages of the mixed dentition. Finally, orthodontists in primary care are only paid once for providing treatment for a patient, which may act as a disincentive for earlier intervention. It is the authors' opinion that this has resulted in a system that generally intends that only ‘one bite of the cherry’ is offered for maximum clinical effect and therefore benefit to the patient.
GDPs have a pivotal responsibility as they are able to assess the developing dentition and identify specific clinical situations where earlier than normal interception would be of great clinical benefit. This article provides a guide to GDPs as to which particular malocclusions to look out for and to refer for early intervention when indicated.
The unerupted maxillary central incisor(s)
The maxillary central incisor usually erupts at around 7½ years of age. It is the second permanent adult tooth to present in the maxilla, after the 1st permanent molar, which erupts 12–18 months earlier. Suspicions should be raised if a central incisor fails to erupt within 6 months of its neighbour, and the deciduous tooth is stubbornly retained and shows little mobility.3 Alteration of the eruption sequence, such as the lateral incisor erupting ahead of the central, is another ‘tell-tale’ sign that something is amiss. Further investigation should always be undertaken in the form of a thorough clinical examination and radiographs of the immediate area, to locate the unerupted tooth. One of the most common causes of failure of eruption of upper centrals is the presence of supernumerary teeth.3 This is more likely to occur in males than females by a ratio of 2:1.4 Pairs of tuberculate supernumeraries can prevent eruption of both central incisors. Supernumerary teeth are estimated to be the cause of obstruction of the central incisors in 28–38% of cases.3 A thorough dental history should be sought, as an alternative reason for an unerupted central incisor could be dilaceration due to primary incisor trauma. This is most likely to be due to an intrusion injury sustained before 4 years of age.
Timely referral to a specialist orthodontist for full assessment and treatment of the clinical situation can prevent space loss and major centre-line shifts. These side-effects could complicate future treatment and prompt intervention will reduce the potential for any teasing or bullying due to the absence of front teeth. Successful management involves the services of an oral surgeon, firstly to remove the offending supernumerary teeth under general anaesthetic, and often to attach a gold chain. Clinicians sometimes choose to wait for the centrals to erupt spontaneously, and the guidelines on this subject suggest up to 78% of unerupted central incisors will erupt in an average time of 16 months.3 This, however, can leave the child without a front tooth for over a year and, if the tooth fails to erupt, then a second general anaesthetic would be needed to attach a gold chain. As with all clinical situations, a decision is made after diligent examination, taking into account the patient's and parent's wishes, on a case-by-case basis.
If spontaneous eruption of the incisor(s) occurs following the surgical intervention, the chains can be simply removed. If the teeth fail to erupt spontaneously, a simple 2x4 appliance can be used to bring the teeth into alignment using the gold chains. A 2x4 appliance usually consists of two bands/bonds on the maxillary first permanent molars, with brackets on the maxillary laterals and, eventually, both central incisors.
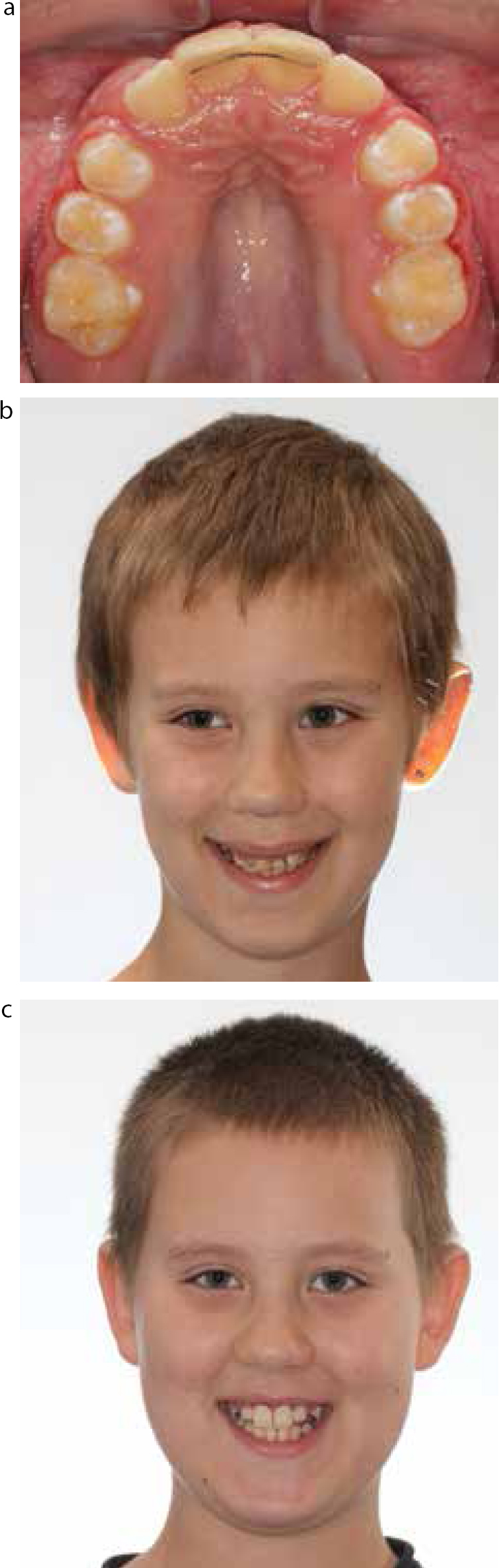
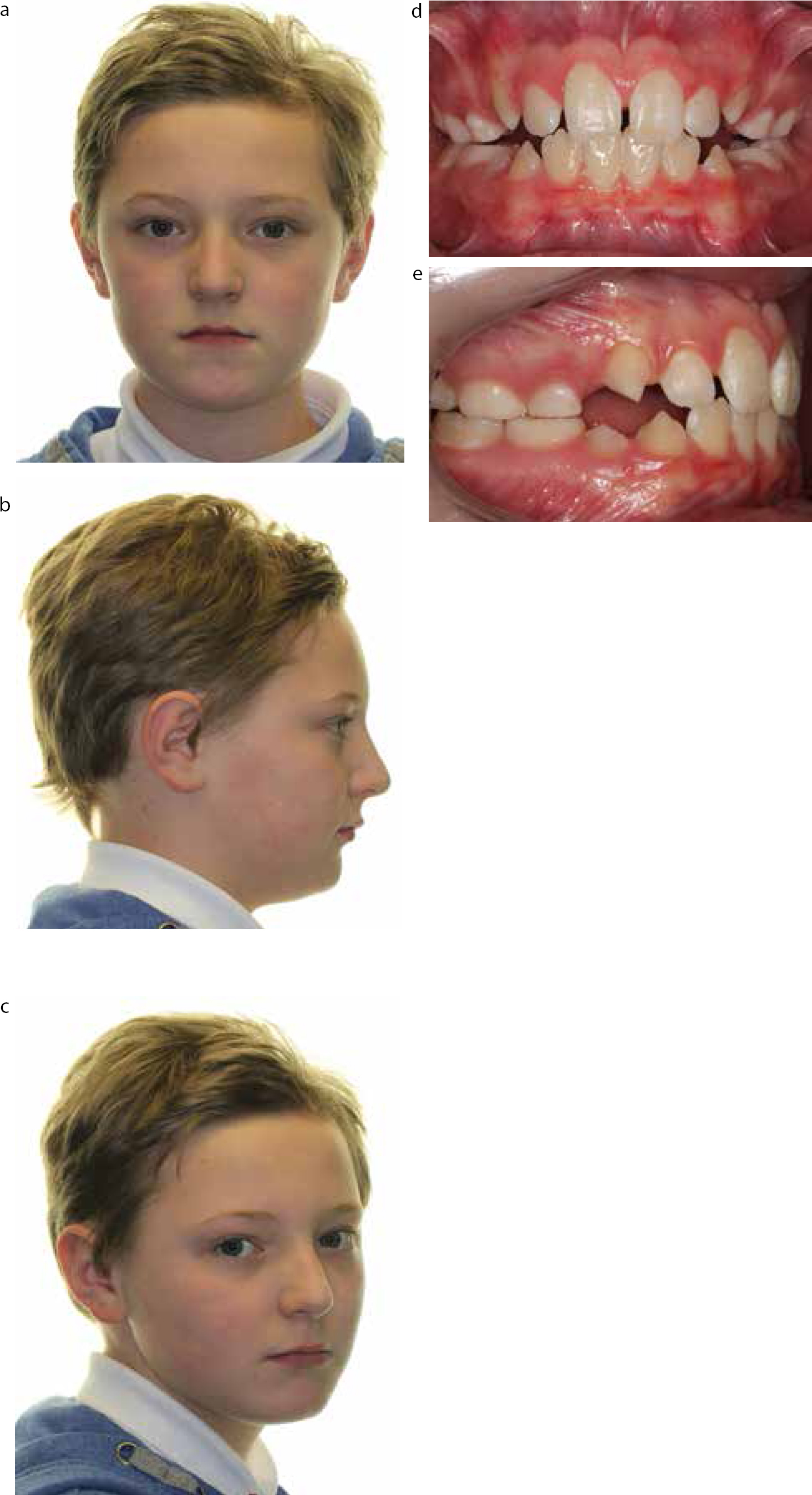
Figures 1–8 demonstrate treatment of the unerupted central incisors in an 8-year-old male patient. The unerupted central incisor(s) is/are usually associated with development of tuberculate supernumerary teeth. These form on the palatal aspect of the developing central incisors. The case demonstrates the multidisciplinary care needed to remove the offending supernumerary teeth and attach gold chains to both central incisor teeth. An unwanted side-effect of delayed eruption of the upper centrals is mesial migration of the lateral incisors. Therefore, the first stage of the brace treatment is to recreate space for the centrals. Next, traction is applied to the unerupted central using a superelastic archwire. Over 9 months, the central incisors are brought into the mouth and aligned in the arch. A bonded retainer is used to hold the centrals in their corrected position.
Figure 1. Initial presentation of patient with erupted laterals, retained As and unerupted maxillary central incisors.Figure 2. Initial OPT (2012) showing 2 tuberculate supernumerary teeth preventing eruption of the upper central incisors.Figure 3. Annotated OPT for surgeons, highlighting that extraction of both supernumerary teeth is required and that gold chains are to be placed on both permanent incisors.Figure 4. An upper fixed appliance is used to create space for the unerupted centrals.Figure 5. A nickel titanium (NiTi) 016 ‘piggy back’ archwire on an 016 stainless steel base archwire.Figure 6. Upper central incisors now erupted and being aligned with 016 NiTi wire.Figure 7. The upper centrals in place 9 months after the initial diagnosis.Figure 8.
(a) Bonded retainer guarantees alignment for as long as it stays in place. (b, c) Improved aesthetics and self-confidence following treatment.
It should always be explained to the patient and parents that this short course of treatment is purely to align the incisors. Definitive treatment will probably still be required to deal with other aspects of the malocclusion and this will be assessed when the full dentition has fully erupted.
GDP learning point:Maxillary central incisors should erupt within 6 months of each other around 7½ years of age. A disturbance in the chronological eruption sequence where the lateral erupts before the centrals is a classic sign that something is wrong.
Correction of crossbites
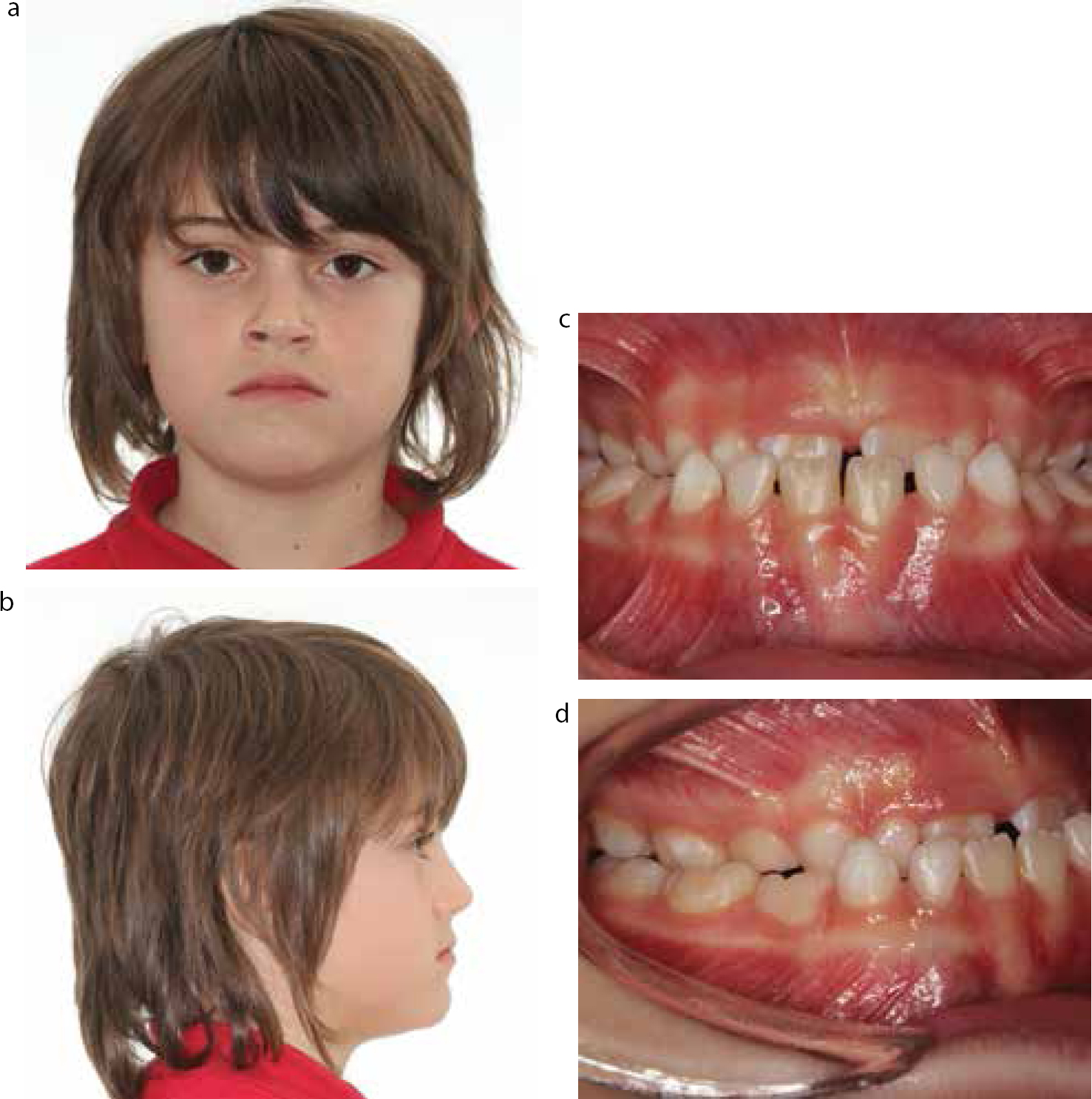
The maxillary central incisors typically erupt between 7 and 8 years of age. If a patient has a slight Class III tendency, or a premature contact with mandibular displacement, one or more of the upper central incisors can erupt into a crossbite relationship with their mandibular counterparts. This can also occur due to crowding or when there is prolonged primary tooth retention. Anterior crossbites that lead to a mandibular displacement during closure can cause protrusion of a lower incisor and result in gingival recession.
There are a number of ways of correcting this feature of the malocclusion. If co-operation is extremely good, a well made upper removal appliance (URA) incorporating T-springs can sometimes effectively correct the crossbite. If patient co-operation is at all in doubt, a 2x4 appliance can be more usefully employed to bring the offending incisor(s) over the bite efficiently in a matter of weeks. In either treatment modality, once a positive overbite has been established, the result should be self-retaining. A recent randomized clinical trial showed little difference in the success rate of fixed and removable appliances in correcting anterior crossbites. The fixed appliance arm of the trial, on average, completed treatment 1 month and 12 days sooner than the removable group.5 This was a statistically significant result and may suggest fixed appliances are superior to removable in terms of treatment efficiency.
Unilateral posterior crossbites with displacement should also be corrected, if at all possible, to prevent establishment of the occlusion in the displaced mandibular position. There is evidence in the literature that early treatment is successful in these cases.6 Bilateral crossbites, usually without displacement, are better accepted. Correct diagnosis of the aetiology and the consequences of the crossbite is best performed by a specialist orthodontist. Crossbites that are largely skeletal in nature are rarely amenable to complete correction by orthodontics alone.
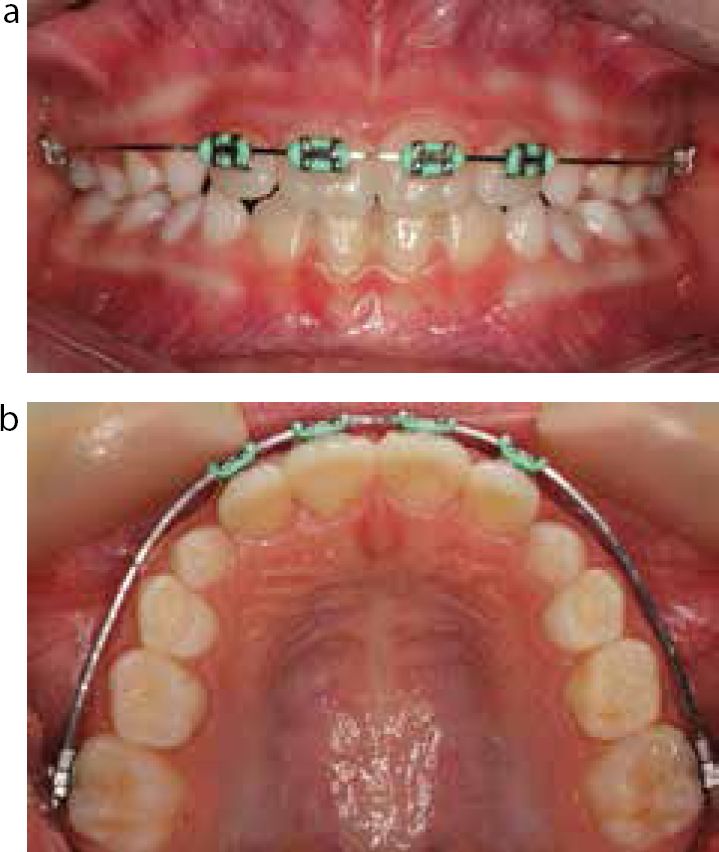
Figures 9 and 10 demonstrate the ease with which a sectional fixed appliance can achieve correction of an anterior crossbite in 4 months. In this almost 8-year-old girl, brackets were bonded to the 1st molars, the maxillary lateral incisors and central incisors. Once initial alignment was achieved using round nickel titanium archwires, rectangular archwires were used to correct the torque of the UR1. Once the incisor is over the bite, this occlusion should be stable and self-retaining.
Figure 9.
(a–c) 7 year 10 month old patient with anterior crossbite and evidence of hard tissue damage to the UR1.Figure 10.
(a, b) Correction of the anterior crossbite within 4 months using a 2x4 fixed appliance.
GDP learning point:Crossbites that are largely dental in aetiological nature can be corrected by removable and fixed appliances. The result can be self-retaining if the overbite is positive and complete to hard tissue. Crossbites that are skeletal in nature, bilateral crossbites and negative overjets without displacement are unlikely to benefit from early intervention using this treatment modality.
Management of poor prognosis 1st permanent molars
First permanent molars may be deemed to be of poor prognosis due to caries or molar-incisor hypomineralization (MIH). The former is thought to affect 16% of all children in the UK.7 In either case, the GDP should refer to an orthodontist for a full orthodontic assessment prior to even considering any extractions. The timing of any extractions is absolutely critical. The decision to retain or extract poor prognosis molars is dependent upon the malocclusion presented, the restorative state of the tooth and the dental age.8 This is a complex topic with the evidence for how to manage each malocclusion restricted largely to expert opinion and clinical judgement.9
In the maxilla, the second permanent molar will generally achieve a good occlusal position, without active treatment, if the first molar is extracted before its eruption.
Extraction timing is more critical in the mandible, where the second molar is liable to tip and rotate into the first molar space if the timing is incorrect. To achieve the maximum amount of space closure and favourable position of the second molar, the first must be extracted when calcification of the second molar bifurcation is seen radiographically. This can occur between 8–10 years of age.
The Royal College of Surgeons has produced guidelines to aid the GDP in assessment and referral decision-making.9
In Class I cases with minimal crowding where space is not required, extraction(s) of 1st permanent molars can be undertaken at the optimum time. Minimal crowding is defined in the guidance as 3 mm or less. In Class I cases with more severe crowding, extraction timing is dependent upon where the crowding is located. If the crowding is in the buccal segments, spontaneous relief may be achieved by extractions at the optimal time. If there is labial segment crowding, then it is worth considering holding onto the 1st permanent molars until the 2nd molars have erupted. The extraction spaces can then be utilized to relieve the anterior crowding, holding the 2nd molars in their initial erupted position using fixed appliances.
In Class II cases space is usually needed in the maxilla to reduce an increased overjet. This can be achieved by using the space from upper 1st molar extraction, once the 2nd molars have erupted or by the use of functional appliances. Each case should be considered unique, and decisions should be made on a case-by-case basis. If minimal crowding is present in the mandible, extraction of the lower 1st molars should take place at the optimal time described.
Lower 1st molar space closure is notoriously difficult and time consuming, therefore increases the risks of decay and demineralization during treatment. Any spontaneous space closure will reduce the strain on the anterior anchorage, which is usually of great benefit.
Class III cases are even more problematic to treat when the 1st permanent molars are of poor prognosis. As a general rule, extraction of maxillary molars should be avoided, until assessment by a specialist orthodontist.
A decision on compensating and balancing extractions can further complicate the decision-making process and is beyond the scope of this article, as this could be an article in its own right! A decision to perform either should be made after consultation with an appropriate specialist.
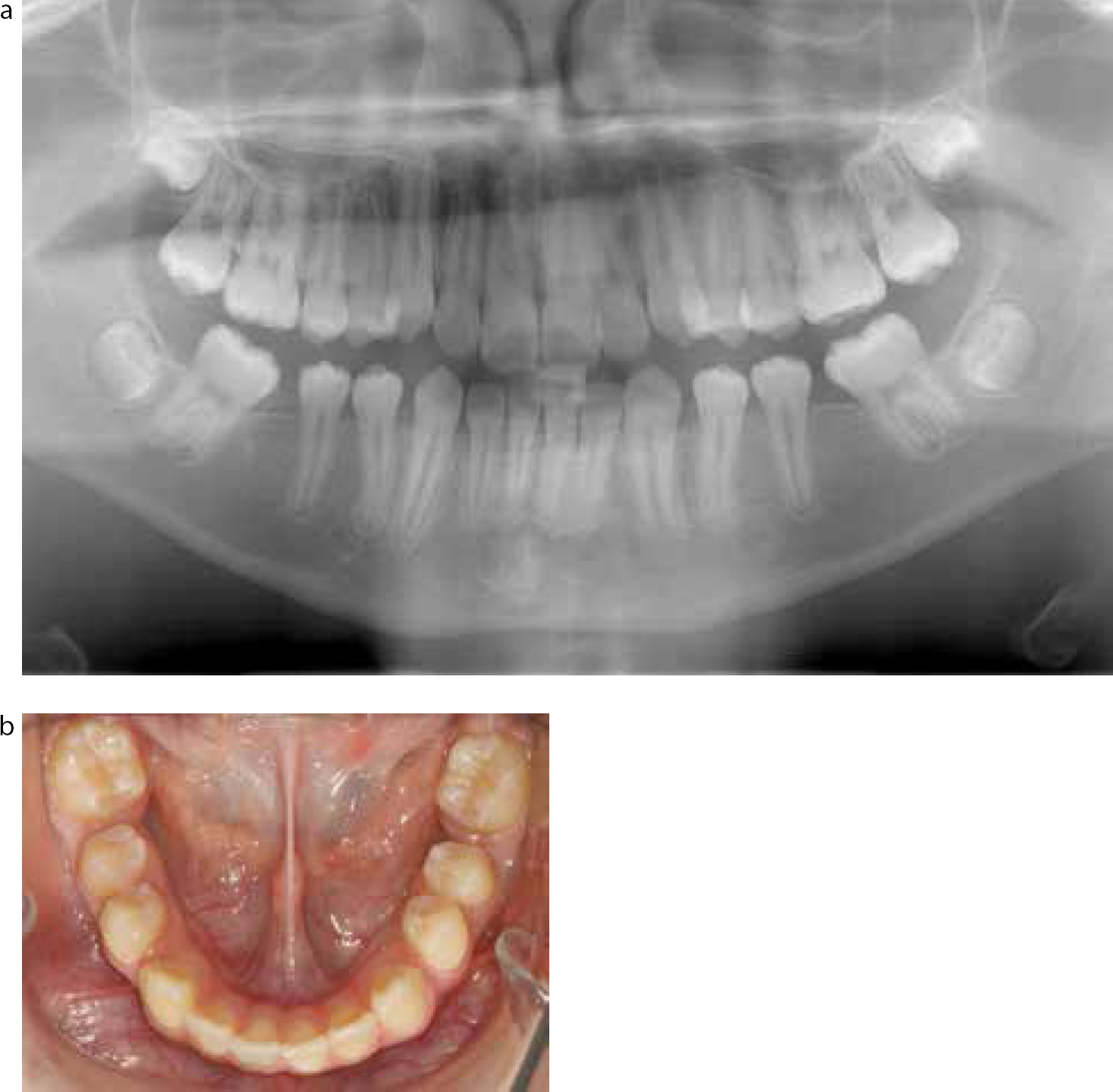
Figures 11 and 12 demonstrate how orthodontic treatment can be simplified by timely extraction of 1st permanent molars. Space closure after extraction of lower 1st molars is time consuming and can result in increased risks of demineralization and decay, as the brace needs to be kept on for longer. By timed extraction of the lower 1st molars, which were hypoplastic in this case, most of the space is closed by favourable eruption of the 2nd molars.
Figure 11. (OPT 2007) Hypomineralized 1st permanent molars due to MIH. Note calcification of the bifurcation of the lower 2nd molars indicating the ideal time for extraction of the lower 1st molars.Figure 12.
(a) (OPT 2010) Same patient 3 years later. Note almost all the lower 1st molar space has closed spontaneously. This will reduce the orthodontic treatment time. (b) Lower occlusal view showing almost complete space closure following timed extraction of hypoplastic lower first molars.
GDP learning point:If space is required for relief of crowding or correction of an overjet, the 1st permanent molars should be maintained until the 2nd molars have erupted. If there are minimal space requirements, then 1st molars should be extracted at the optimal time described. Treatment planning of these cases is complex and expert opinion should be sought, where possible, before performing extractions.
Early loss of deciduous teeth: prevention of centre-line shifts, overeruption of teeth and space loss
Sometimes, in the developing dentition, premature loss of deciduous teeth is inevitable due to caries or trauma. The GDP should be aware of the detrimental effect unilateral tooth loss can have on centre-lines. Early loss of primary incisors can result in anterior crowding. Balancing extractions of the contralateral deciduous canines and 1st deciduous molars should be considered before extracting unilaterally.10
Compensating upper extractions have been suggested when lower molars are extracted, supposedly to prevent problems associated with over eruption of upper molars. The evidence for this treatment approach is extremely weak and it is clearly stated in the RCS guidelines that further research is required in this area.10 Any case having one or more molars extracted for reasons of disease should have a comprehensive orthodontic assessment to decide upon other extractions required. GDPs should focus their efforts on improving a patient's oral hygiene and dietary regimen if these teeth have been lost due to caries. Overerupted teeth, if they do occur, can easily be dealt with later using sophisticated orthodontic techniques.
Early loss of primary teeth can compound the crowding situation and lead to severe displacement of adult teeth. If a deciduous tooth has to be lost early, the opinion of an orthodontist should be sought in order to determine whether a space maintainer should be used to hold space. The fabrication of a space maintainer is usually straightforward and may prevent impaction of teeth in the future. Figures 13–14 highlight the detrimental effects of early deciduous tooth loss. Figure 15 shows an example of a simple space maintainer that can be used to hold space for the adult dentition, and reduce the orthodontic burden on the patient.
Figure 13.
(a, b) Early loss of the URC has resulted in a marked upper centre-line shift to the right and exclusion of the UR3 from the arch.Figure 14. Early loss of the 2nd deciduous molars allowed first molars to drift mesially resulting in crowding in the 2nd premolar area. In this case they erupted palatally.Figure 15. Example of a space maintainer holding space for an erupting LR5.
GDP learning point:From an orthodontic perspective, it is desirable for GDPs to maintain the deciduous dentition until their normal exfoliation date to reduce the detrimental effects early loss causes.
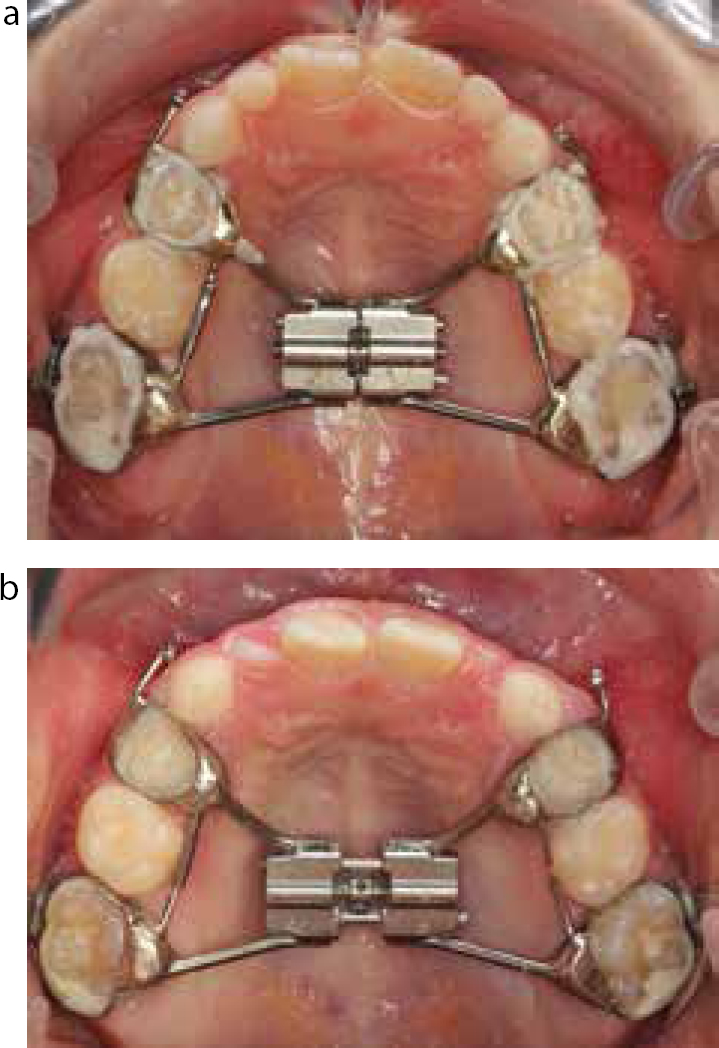
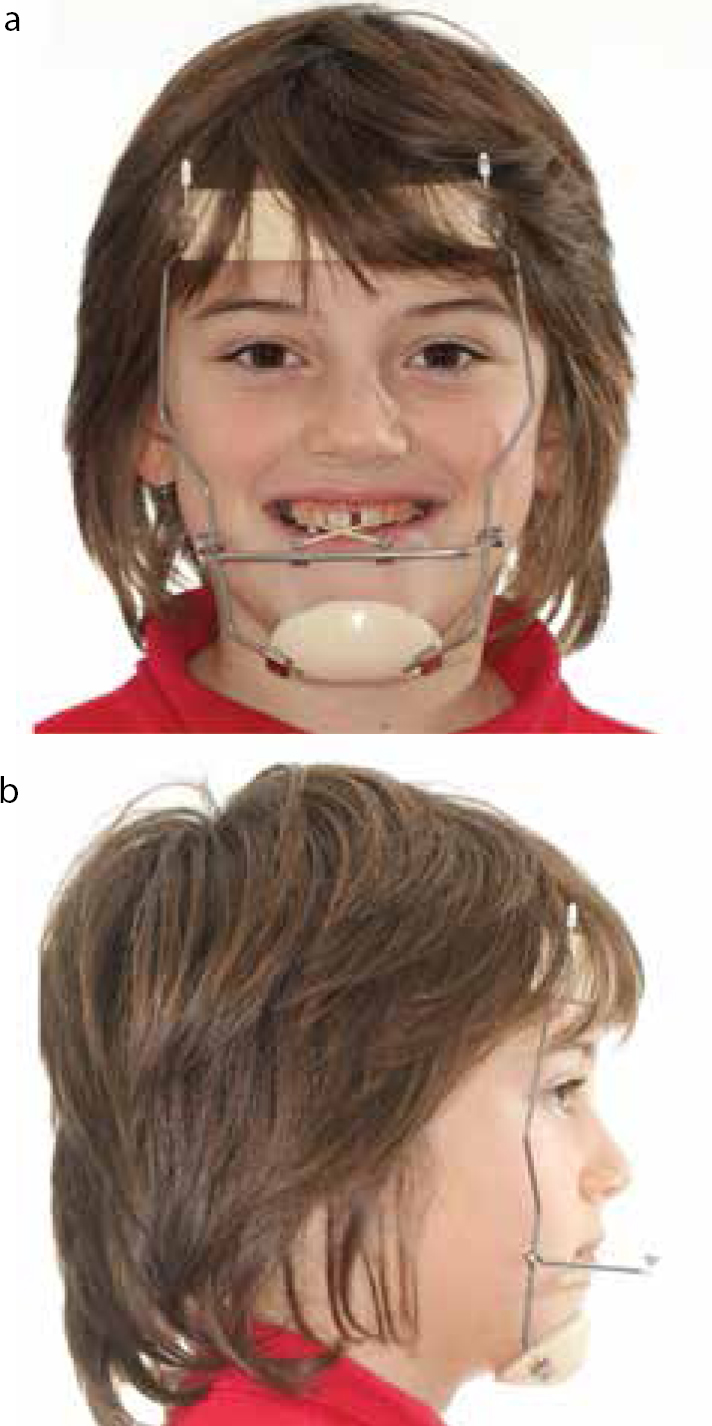
Early Class III correction
Recent randomized control trials have been undertaken in the UK11,12 that report successful early CIII correction, in 7–9 year-old children. This was achieved by using the protraction facemask and involved firstly fitting a rapid maxillary expander (RME) to disrupt the circum-maxillary sutures and widen the maxilla for around 10 days. After this, a facemask was fitted and an anterior force was applied to the maxilla with elastics, to correct the negative overjet. The strength of these elastics was gradually increased over a 6-week period until a force of 400 g each side is applied. Excellent compliance is required for this treatment to work and achieve a positive overjet. The facemask must be worn at least 14 hours a day to have any realistic chance of working. Overall treatment time is around one year to achieve a positive overjet.
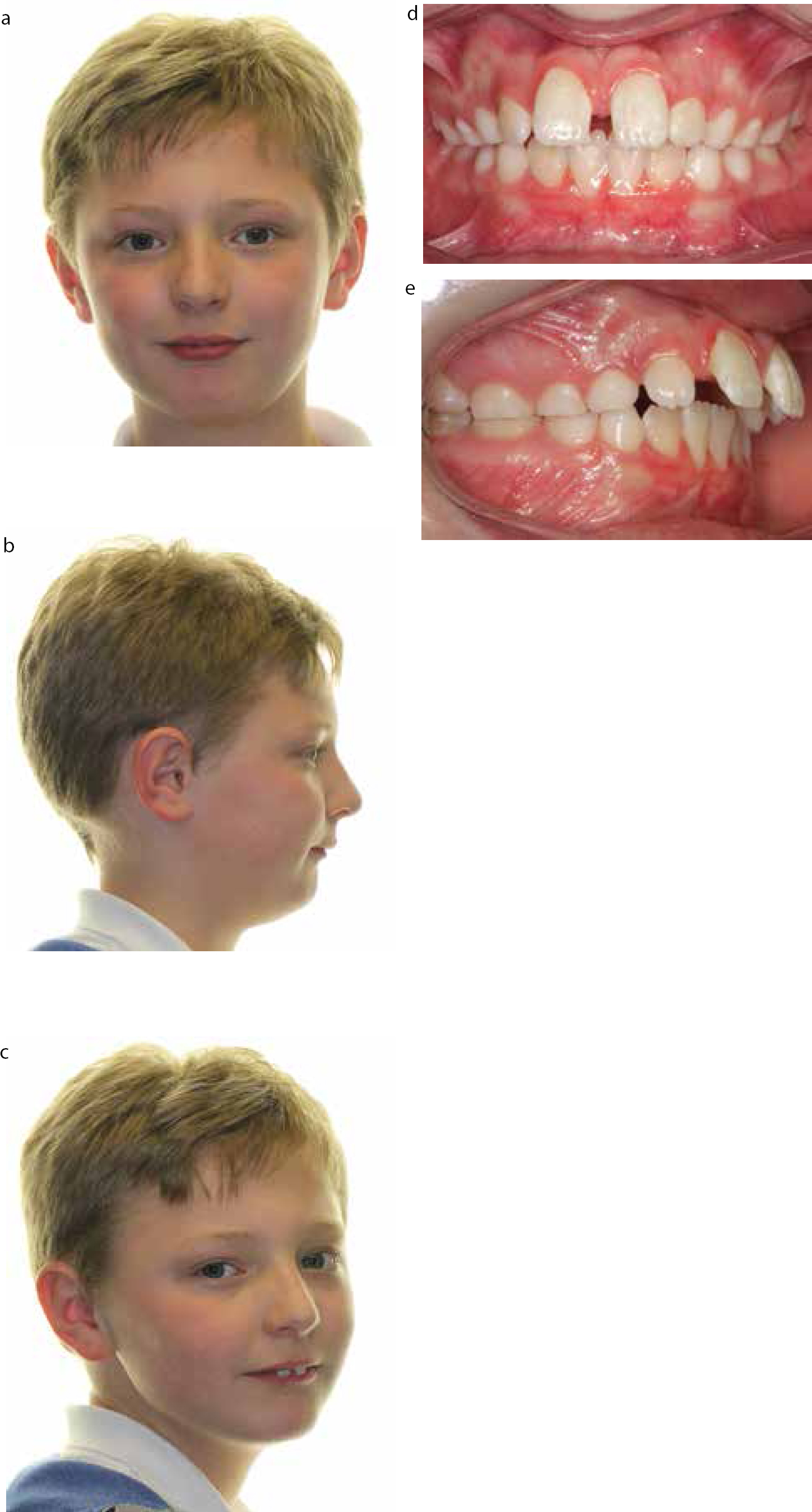
As demonstrated in the case shown (Figures 16–21), a -4 mm overjet can be reduced to a +2 mm overjet. After one year of treatment the appliance was removed. Cephalometrics confirmed the clinical impression that, facially, the patient had become less Class III in profile.
Figure 16.
(a–d) 8-year-old at initial presentation with Class III incisors and -4 mm overjet.Figure 17.
(a) Fitting of RME. (b) RME post expansion.Figure 18.
(a, b) Facemask appliance.Figure 19. Establishment of a positive overjet following 9 months of facemask treatment.Figure 20.
(a, b) Extra-oral views confirm cephalometric measurements that maxilla has been brought forwards by the facemask appliance.Figure 21.
(a, b) Intra-oral views at debond of the appliance.
Studies suggest that patients presenting with a hypoplastic maxilla, rather than a prognathic mandible, are most likely to benefit from this treatment. The authors state12 that this treatment has a 70% success rate 3 years after the appliance has been removed. It should be noted that the majority of the patients in this study have still not completed growth. It will be interesting to see in future publications if the facemask effects are maintained after the pubertal growth spurt.
GDP learning point:Interceptive treatment of Class III malocclusions using protraction facemask therapy is promising. However, no long-term follow-up trials have been published to show the gains earned before puberty are maintained or lessen the treatment burden.
Early Class II correction
Skeletal Class II correction is usually attempted during a child's pubertal growth spurt; around 12 in females and 14 in males.13 Theory would suggest that growth potential could be utilized to correct anteroposterior discrepancies by enhancing forward growth of the mandible. Deep overbites can be corrected by vertical growth at the condyle and by altering the post eruption movements of selected teeth.
Most orthodontists have not advised early Class II correction (before average aged growth spurt) due to the issues around relapse, stability and re-treatment. ‘Burnout’ of patient co-operation can also result. There is some evidence in the literature that early treatment should be considered if the malocclusion is causing psychological distress in a child due to his/her appearance.14 A recent update to the Cochrane review on this subject has also shown that there may be a 41% reduction in incisor trauma if treatment for an increased overjet is commenced early.15 It should be noted that the confidence interval for this benefit was wide, indicating a large number of patients that needed to be treated before one patient actually benefits from this treatment effect. Also, the majority of the ‘trauma’ that occurred in patients not treated early was minor, with only one patient out of 27 receiving trauma that had pulpal involvement.
The example case (Figures 22–24) shows that functional treatment in the mixed dentition is possible if co-operation is excellent. The patient presented aged 9 years old complaining about his dental appearance. His initial overjet was 10 mm This was a source of teasing at school. A Clarks Twin Block was fitted and worn full time for 10 months. The treatment reduced the overjet to 2 mm and reduced the severity of the Class II skeletal base. Although impressive, issues with pubertal growth and retention of the gains achieved mean that the outcome of this early treatment is uncertain. It should be noted that most of the changes in this case have been brought about through dento-alveolar tipping of teeth rather than enhanced skeletal growth.
Figure 22.
(a–e) Pre-treatment views of early CII correction patient.Figures 23.
(a–d) Twin block appliance in situ.Figure 24.
(a–e) Post-treatment views of early CII correction patient showing improved lip competence and average overjet.
GDP learning point:The advice to GDPs is that, if a child or parent complains of bullying or distress due to dental/facial appearance, then expert opinion should be sought as to the risks and benefits of early Class II correction.
Submerging teeth
Monitoring dental development is an important aspect of dental care for the GDP. Ankylosis and infraocclusion is estimated to occur in up to 9% of children.16 Normally, deciduous teeth naturally exfoliate as the permanent dentition erupts. Occasionally, deciduous teeth can become ankylosed and submerge during jaw development. Further investigation with appropriate radiographs is essential in these cases. The most common condition associated with submerging teeth is congenital hypodontia. Failure to detect this early can result in complete submergence of the deciduous teeth, making extraction of these teeth difficult. A surgical extraction can make preservation of alveolar bone for later implant placement difficult. In selected cases, elective extraction of deciduous teeth when there is no permanent successor may be appropriate, to allow for spontaneous space closure.
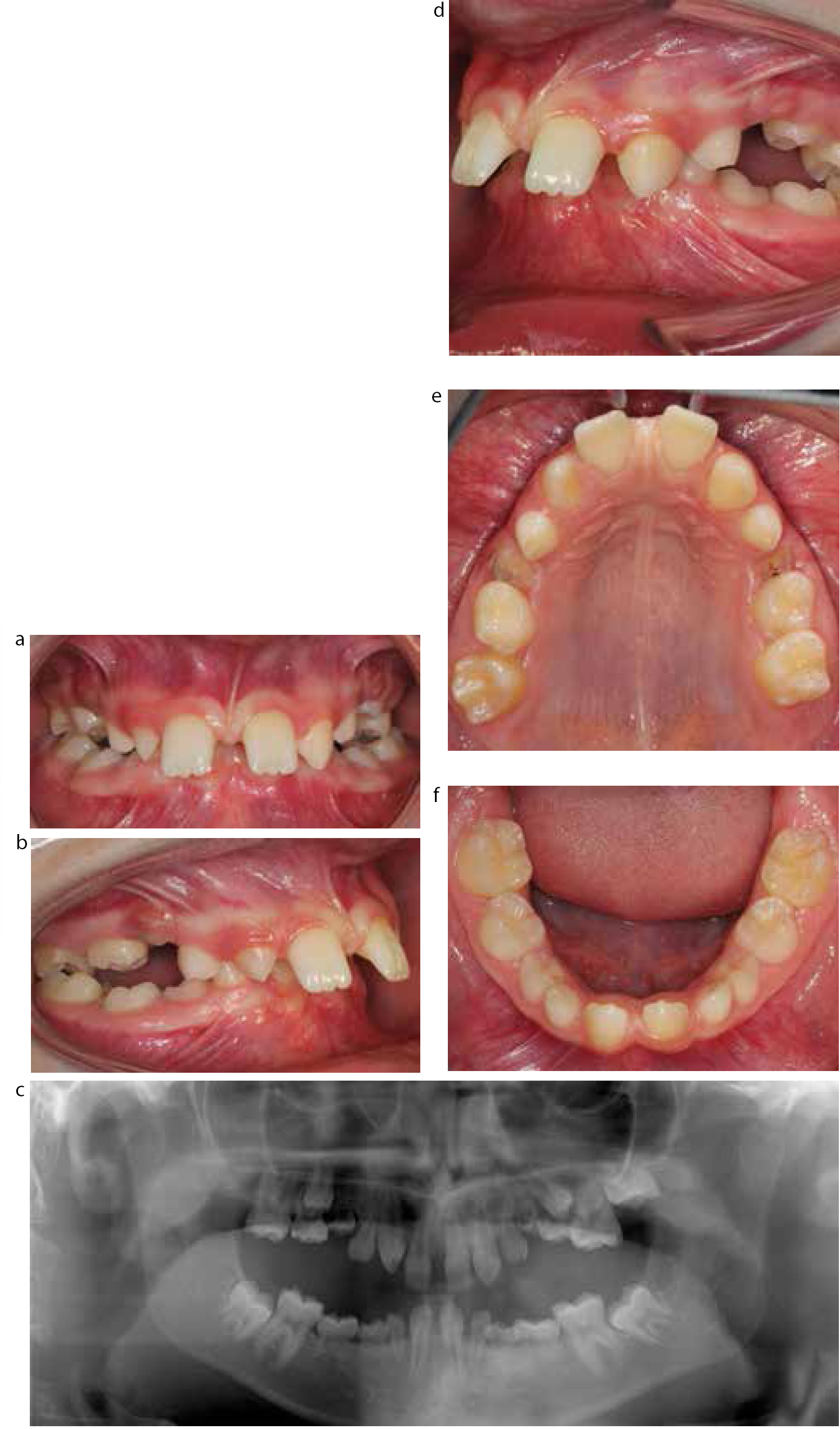
The detrimental effects of hypodontia, coupled with a submerging deciduous dentition, are seen in Figure 25. The patient presented aged 11 years old with a Class II division 1 incisal relationship on a moderate skeletal 2 base. This was complicated by the fact that the following teeth were congenitally absent; UL4,2, UR2,4,7, LL5,4,2,1, LR1,2,4,5. Development of the 3rd molars could not be seen.
Figures 25.
(a–f) Hypodontia case with associated submerging deciduous teeth: intra-oral views and OPT at initial presentation. In order to treat this case to perfection, many years of orthodontic treatment with restorative input will be required.
There were signs clinically and radiographically that the ULE, ULD, URD and both lower Es were submerging. Unfortunately, there had already been vertical bone loss, which may make future implant placement difficult. To date, the patient has been assessed by a consultant orthodontist and consultant restorative dentist. The initial plan is to remove the submerging deciduous teeth and monitor and maintain the remaining deciduous dentition. The marked Class II skeletal base was associated with an increased overjet of 14 mm. The first stage of treatment is to address this anteroposterior issue with a functional appliance. Hopefully, further fixed appliance treatment will be used later to redistribute the spaces due to the missing teeth. The spaces will eventually be restored with fixed prostheses.
GDP learning point:Regular clinical examination with appropriate radiographic examination is paramount to detect hypodontia. Monitor submergence carefully and refer early for advice and management.
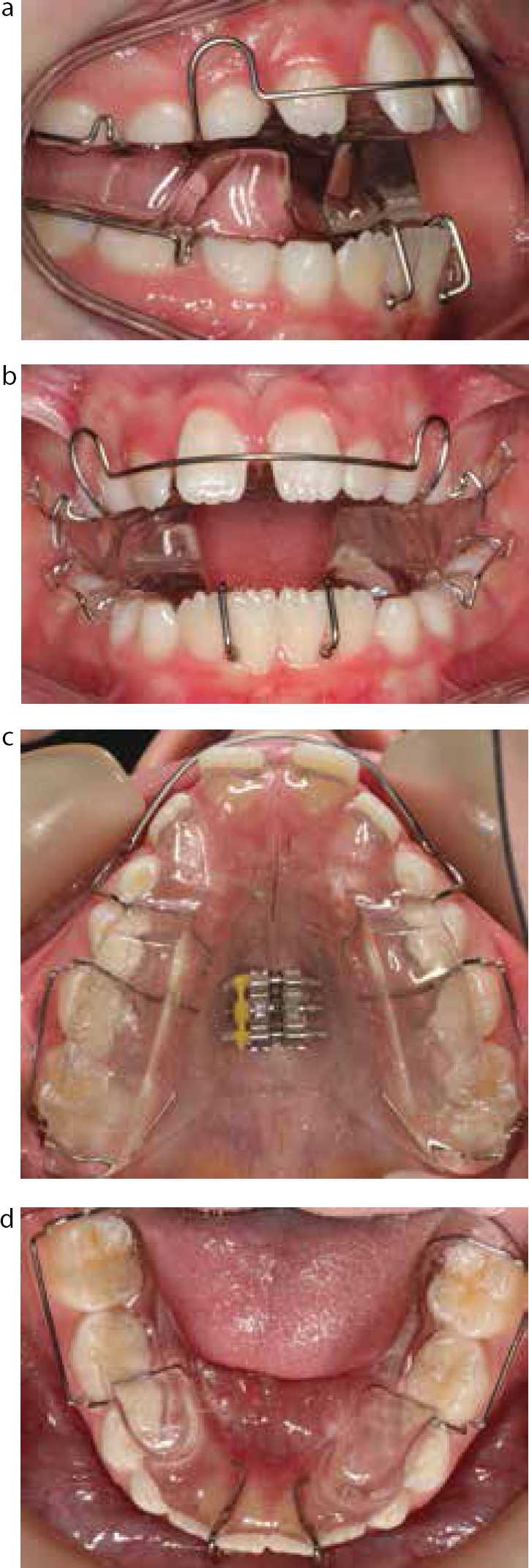
Anterior open bite
One of the most challenging malocclusions to treat in orthodontics are anterior open bites. The aetiology of anterior open bites can be skeletal, soft tissue, habit or a combination of these influences. Anterior open bites (AOB) present in 2–4% of children17 with an increased incidence in African and Afro-Caribbeans.18 Whilst anterior open bites that are purely skeletal in origin are probably only correctable through orthognathic surgery, the AOB that establishes due to a digit-sucking habit can be treated early. Obviously, cessation of the habit by willpower alone would be ideal but many children find this habit hard to break. After woollen gloves, plasters and stop ‘n’ grow nail pastes have been tried, orthodontics may be the only course of action. Classically, a malocclusion due to digit-sucking will present with the following features:
Reduced overbite: AOB may be asymmetrical, greater on the side the digit is used;
Unilateral posterior crossbite with a narrow upper arch;
The presentation can be highly variable and dependent upon the duration, intensity and frequency of the habit.
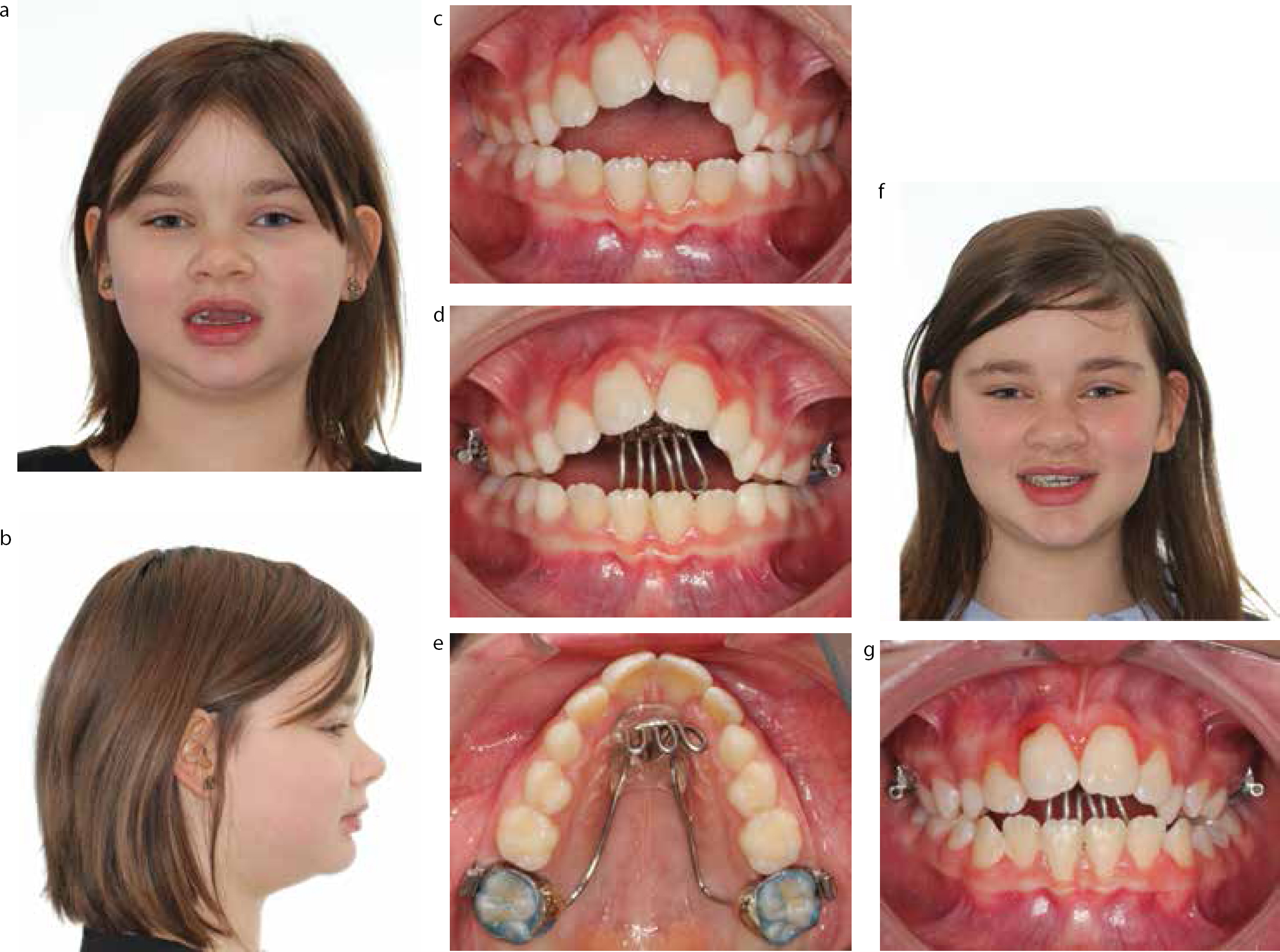
Use of a hayrake appliance to stop the digit entering physically can be a successful way of breaking the habit and reducing the AOB (Figure 26). The patient presented at 8 years old with a 9 mm AOB and Class II skeletal base. The patient's mother had exhausted all options at her disposal and was desperate for some treatment. The hayrake appliance was fitted and in situ for 9 months. It was effective at breaking the habit and reducing the AOB down to 3 mm. This has improved the girl's dental aesthetics partially. It is hoped that further treatment can be performed later to improve the malocclusion, if the oral hygiene becomes impeccable.
Figure 26.
(a–g) Anterior open bite case to demonstrate the effectiveness of breaking a thumb-sucking habit on the reduction of a severe anterior open bite.
GDP learning point:Recognize the clinical presentation of anterior open bite associated with digit-sucking. Provide support and advice on habit cessation. If this fails, consider referral to an orthodontist for treatment.
Conclusion
Vigilance of a caring GDP should allow intervention, which may prevent some of the problems highlighted in this article. Prompt diagnosis and early referral for treatment by the orthodontist will certainly reduce the burden of the malocclusion in the future with this special group of patients. This paper has highlighted clinical signs for the GDP to watch out for and, if in doubt, refer to an appropriate specialist.