Glendor U. Epidemiology of traumatic dental injuries – a 12-year review of the literature. Dent Traumatol. 2008; 24:603-611
Kaste LM, Gift HC, Bhat M, Swango PA. Prevalence of incisor trauma in persons 6–50 years of age: United States, 1988–1991. J Dent Res. 1996; 75:696-705
Eilert-Petersson E, Andersson L, Sörensen S. Traumatic oral vs. non-oral injuries. An epidemiologic study during one year in a Swedish county. Swed Dent J. 1997; 21:55-68
Lindqvist KS, Brodin H. One-year economic consequences of accidents in a Swedish municipality. Accid Anal Prev. 1996; 28:209-219
Glendor U, Halling A, Bodin L, Andersson L, Karlsson G, Koucheki B. Direct and indirect time spent on care of dental trauma: a 2-year prospective study of children and adolescents. Endod Dent Traumatol. 2000; 16:16-23
Andreasen FM, Andreasen JO. Luxation injuries. In: Andreasen JO, Andreasen FM (eds). Copenhagen: Munksguard; 1993
Andreasen JO, Andreasen FM, Skeie A, Hansen E, Schwatrz O. Effect of treatment delay upon pulp and periodontal healing of traumatic dental injuries – a review article. Dent Traumatol. 2002; 18:116-128
Trope M. Root resorption due to dental trauma. Endod Topics. 2002; 1:79-100
Andreasen FM. Transient apical breakdown and its relation to colour and sensibility changes after luxation injuries to teeth. Endod Dent Traumatol. 1986; 2:9-19
Andreasen JO, Andreasen F. Root resorption following traumatic dental injuries. Proc Finn Dent Soc. 1992; 88:95-114
Darcey J, Qualtrough A. Resorption: part 1. Pathology, classification and aetiology. Br Dent J. 2013; 214:439-451
Darcey J, Qualtrough A. Resorption: part 2. Diagnosis and management. Br Dent J. 2013; 214:493-509
Heithersay GS. Clinical, radiographic and histopathological features of invasive cervical resorption. Quintessence Int. 30:27-37
Patel S, Kanagasingam S, Mannocci F. Cone beam computed tomography (CBCT) in endodontics. Dent Update. 37:373-379
Andreasen JO, Borum M, Jacobsen HL, Andreasen FM. Replantation of 400 avulsed permanent incisors. IV. Factors related to periodontal ligament healing. Endod Dent Traumatol. 1995; 11:76-89
Schjøtt M, Andreasen JO. Emdogain does not prevent progressive root resorption after replantation of avulsed teeth: a clinical study. Dent Traumatol. 2005; 21:46-50
Tan WL, Wong TL, Wong MC, Lang NP. A systematic review of post-extractional alveolar hard and soft tissue dimensional changes in humans. Clin Oral Implants Res. 2012; 23:1-21
Andersson L. The problem of dentoalveolar ankylosis and subsequent replacement resorption in the growing patient. Aust Endod J. 1999; 25::57-61
Gassner R, Bösch R, Tuli T, Emshoff R. Prevalence of dental trauma in 6000 patients with facial injuries. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 1999; 87:27-33
McDade AM, McNicol RD, Ward-Booth P, Chesworth J, Moos KF. The aetiology of maxillo-facial injuries, with special reference to the abuse of alcohol. Int J Oral Surg. 1982; 11:152-155
Dental injuries are a relatively common occurrence and need to be managed well in general dental practice in order to produce the most favourable outcome for patients. Dental practitioners should familiarize themselves with the guidelines provided by the International Association of Dental Traumatology discussed herein. These guidelines clearly state how dental injuries should be managed, including suggested review. Dentists should be aware of injuries that are most likely to require input from specialist services and relative risks of long-term complications and how to identify these. Early identification of such complications should prompt referral to specialist services.
CPD/Clinical Relevance: The ability to treat dental trauma in light of knowledge of long-term complications is of importance to the general dental practitioner.
Article
Prevalence data on dental trauma is variable between countries, this mainly being due to differences in the way information is gathered and injuries are reported. Despite this, the worldwide prevalence of dental trauma may be considered to be high. Approximately one-third of all adults have experienced traumatic dental injuries during their lifetimes.1 These injuries are more prevalent in the permanent dentition and most likely to affect the maxillary anterior teeth;2 this may have a negative impact on long-term quality of life for the patient involved. Traumatic dental injuries constitute around 5% of all body injuries in the 0–30 years age group per year.3 Compared to many other injuries managed in an out-patient setting, dental trauma has greater treatment costs, and time implications.4,5
Although the worldwide prevalence of dental trauma is high, practitioners may not treat dental trauma regularly, therefore, confidence in trauma management may be low. In this regard, the Glasgow Dental Hospital Trauma Service has set up a triage system for acute dental trauma referrals. Dental injuries are classified as ‘Simple’ or ‘Complex’ based upon the complexity of initial management and risk of complications. Simple trauma should be managed in primary care, with appropriate guidance. Complex dental trauma may require secondary care or specialist input (Table 1).
Classification
Simple
Complex
Injury
ConcussionSubluxationEnamel infractionEnamel-dentine crown fractureRoot fracture (apical 2/3 and without displacement)Avulsion
ExtrusionDisplaced or cervical 1/3 root fractureLateral luxationDento-alveolar fractureIntrusionImmature apex
A number of factors have been found to be strong predictors on the long-term outcome of dental injuries. These are:
The Dental Trauma Guide, from the International Association of Dental Traumatology (IADT) is an excellent resource which provides a comprehensive bank of evidence-based resources and guidelines on the management and review of dental trauma.8,9 The database is continuously updated to reflect the most up-to-date knowledge. The Dental Trauma Guide ‘risk calculator’ provides prognoses for teeth with traumatic dental injuries, based on the Copenhagen trauma database.8 The database includes 2191 traumatized permanent teeth from 1282 patients that were treated at the dental trauma unit at the University Hospital in Copenhagen (Denmark) between 1972 and 1991. The risk calculator allows dental practitioners to extract the prognosis and risk of adverse outcomes following injury easily, for any individual tooth. Prognosis is calculated after information relating to the injury type, stage of root formation, results of sensitivity testing and extra-alveolar dry time *(avulsion injury), is entered. Percentage risk of each potential adverse outcome is then displayed in a line graph. It is important to discuss with patients the risks associated with their traumatic injury and make them aware of the importance of regular review in line with IADT guidelines.9
Dental trauma can result in a number of long-term complications, including discoloration, loss of vitality and inflammatory root resorption. Unfavourable tooth positions and defects in hard and soft tissues may also result, complicating aesthetic management. This is either as a direct result of tooth loss or damage to the tooth, cementum and periodontal ligament. Intrusion is the greatest cause of unfavourable healing post-trauma, followed by avulsion, lateral luxation, extrusive luxation, subluxation and concussion injuries.10 Correct follow-up and early diagnosis is key to ensuring optimal outcomes for those patients affected.
Discoloration
Discoloration of teeth can be external or internal. External discoloration is due to an accumulation of staining media on the tooth surface or a developmental disturbance of enamel. Internal discolorations are due to absorption of pigmented particles into dentine and cementum. In traumatized teeth, most discoloration is internal and can be diagnosed by visual inspection during dental examination. They are often self-reported by patients and are highly indicative of an underlying problem such as canal obliteration (yellow) or pulp necrosis (grey).
Intrinsic colour is determined by the optical and light transmission properties of enamel and dentine. Laying down of tertiary dentine, as occurs in canal obliteration, causes reduced light transmission, resulting in yellow discoloration. Severe pulpal trauma may result in the rupture of pulpal blood vessels and leakage of blood into the tooth structure. This initially results in pink discoloration. When the pulp vitality is maintained this may be reversible, as the pulp becomes revasularized (2–3 months).11 If pulpal necrosis occurs, noxious by-products penetrate the dentine tubules and discolour the surrounding dentine grey. This may affect the whole tooth and worsen with time.
Pulp necrosis/apical periodontitis
In traumatic dental injuries where the neurovascular supply to the pulp has been totally severed, mechanisms for revascularization and re-innervation are present. In teeth where revascularization fails, the pulp tissue will undergo sterile necrosis, subsequent bacterial infection may then occur. After 3–4 weeks, these teeth will show radiographic indications of pulp necrosis with the development of an apical periodontitis, demonstrated by apical radiolucency on a radiograph. There are common diagnostic indicators of pulpal necrosis which should be examined at routine trauma follow-up, in line with IADT guidance.9
Diagnostic indicators for pulp necrosis are shown in Table 2.
Periapical radiolucency
Discoloration of the tooth crown (usually grey/brown)
Infection-related external root resorption
No response to pulp sensitivity test
Tenderness to percussion and palpation in the vestibule develops after an asymptomatic period
Presence of a fistula (sinus tract)
Resorption
Resorption lesions can be most simply classified as external or internal. There have been numerous attempts to classify resorption lesions in the literature, largely based upon the site and type of resorptive process, or the aetiology. The classification adhered to in this paper is that proposed by Andreasen and Andreasen, which is widely acknowledged and used.12
External inflammatory root resorption
External inflammatory resorption (EIR), as the name suggests, is root resorption that occurs on the outer surface of the root as a result of an inflammatory stimulus (Figure 1). Andreasen and Andreasen12 proposed a series of four events necessary for this to occur. Firstly, there must be trauma to the root surface, followed by external surface resorption. In many cases this is transient and is a consequence of localized and limited injury to the root surface or surrounding periodontium. It heals uneventfully and is subclinical in the majority of cases.12 However, a prolonged stimulus to the damaged root surface allows continuation of this process. Exposure of the resorptive lesion to the dentinal tubules on a tooth with an infected or necrotic pulp will mean that the process inevitably progresses. The age of the tooth must also be considered, with immature teeth more frequently affected. If undiagnosed, this process can completely resorb roots in a matter of months.13
Figure 1. External inflammatory root resorption with canal obliteration following trauma to UR1.
If resorption is due to stimulation from an infective process the stimulus should be halted and orthograde endodontics is the treatment of choice. Endodontic therapy undertaken to a high standard results in favourable outcomes in cases of EIR. It is wise to favour a multiple visit approach as it is known that chemo-mechanical disinfection may not eradicate all pathogens. An inter-appointment medicament of calcium hydroxide should be used, as it eradicates bacteria, may necrotize cells in the resorptive lacunae, neutralize the acidic environment of the lacunae and also stimulate repair. Long-term, placement of calcium hydroxide has a significantly negative effect upon fracture resistance of dentine and therefore such dressings should not be left in situ for over 30 days.14
External cervical root resorption
External cervical resorption (ECR) can be defined as a localized resorptive lesion of the cervical area of the root below the epithelial attachment (Figure 2). There is rarely pulpal involvement in a vital tooth unless the lesion is extensive. It is this feature that helps differentiate between ECR and EIR: in the latter pulpal necrosis or infection are prerequisites. As with all lesions, there may only be a small area of activity of the external surface of the root, but it can expand within the dentine, both coronally and apically, encircling the pulp. As the lesion progresses there can be extensive tooth structure loss, which in the most advanced cases can result in pathological crown-root fracture.
Figure 2. External cervical root resorption affecting teeth UR1 and UL1 following trauma (these teeth were unrestorable).
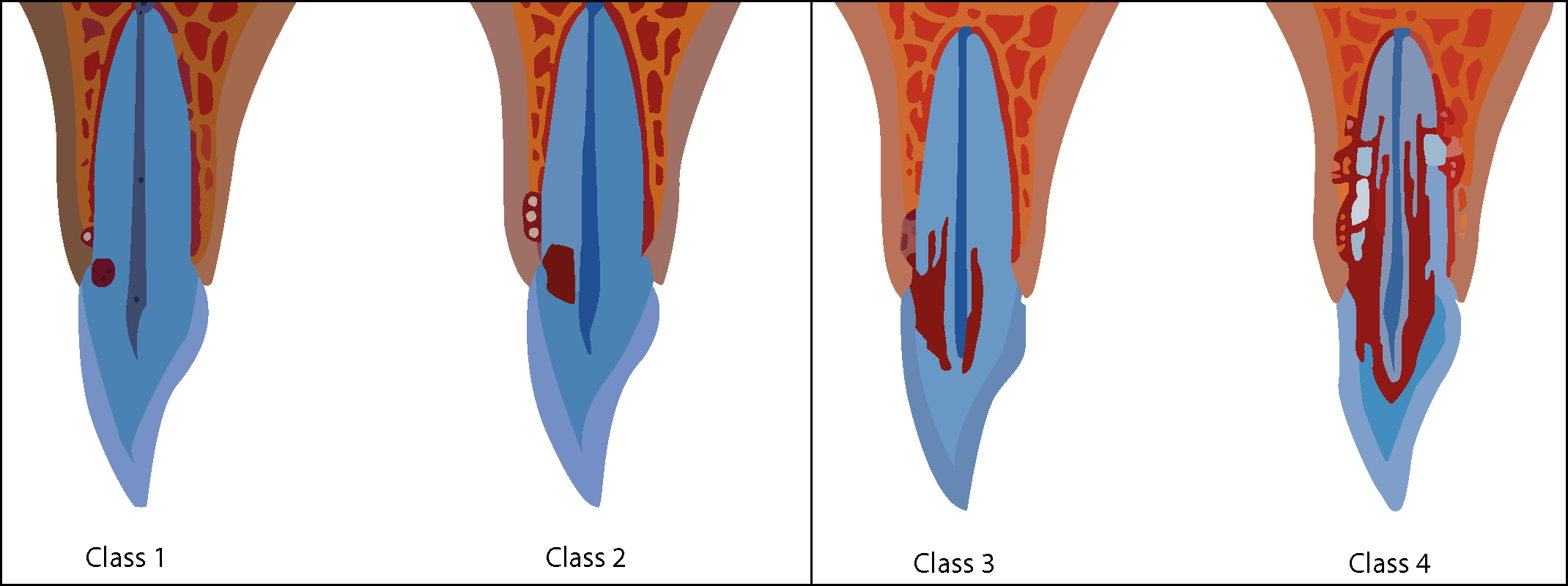
Progression of the resorptive defect, once the dentine has been penetrated, is variable and unpredictable. Heithersay has classified this type of resorption into four classes in order of severity (Figure 3).15
Figure 3. Heithersay's classification of external cervical root resorption.15
The focus of treatment is to access the resorptive lesion, remove resorptive tissue and restore the cavity. The site, extent and pulpal involvement of the cervical resorptive lesion will dictate the treatment protocol. Heithersay suggests that Class 1–3 lesions are restorable but Class 4 lesions rarely so.
Internal inflammatory root resorption
Internal inflammatory resorption (IIR) takes place within the root canal system and is more rare than external root resorption. The precise aetiological and pathological mechanism remains poorly understood. It is characterized by oval-shaped enlargement of the root canal space and typically expands in an apical and lateral direction (Figure 4). There may be chronic pulp inflammation and it is often analogous with EIR. External resorption, which is much more common, is often misdiagnosed as internal resorption.
Figure 4. Internal inflammatory root resorption characterized by ballooning of the pulp canal space.
The aim of treatment in internal resorption cases is to remove any stimulus and vital tissue that may be allowing the resorptive process to perpetuate. If the tooth is restorable, orthograde root canal treatment (RCT) is usually the treatment modality of choice. It is inappropriate to carry out RCT in these cases in a single-visit as, even with good chemo-mechanical principles, canal disinfection can be unpredictable and should be complemented with an inter-appointment dressing of calcium hydroxide.
Consideration must be given to obturation of both the canal apical to the resorptive cavity, the resorptive cavity and coronal canal. The apical portion may be obturated with cold lateral condensation, warm vertical compaction or continuous wave compaction. Flowable gutta percha and vertical condensation is then necessary for optimum three-dimensional obturation of the resorptive cavity itself (Figure 4).
Diagnosis of root resorption
Teeth affected by resorption lesions are often asymptomatic and may present as an incidental finding upon radiographic examination, so it is essential that the clinician should pay particular attention to aspects of the history that may play a role in the development of resorption. In the context of this paper, the most relevant history is that of dental trauma, although it should be noted that there are numerous other aetiological factors.14 The history should be complemented by thorough clinical examination.
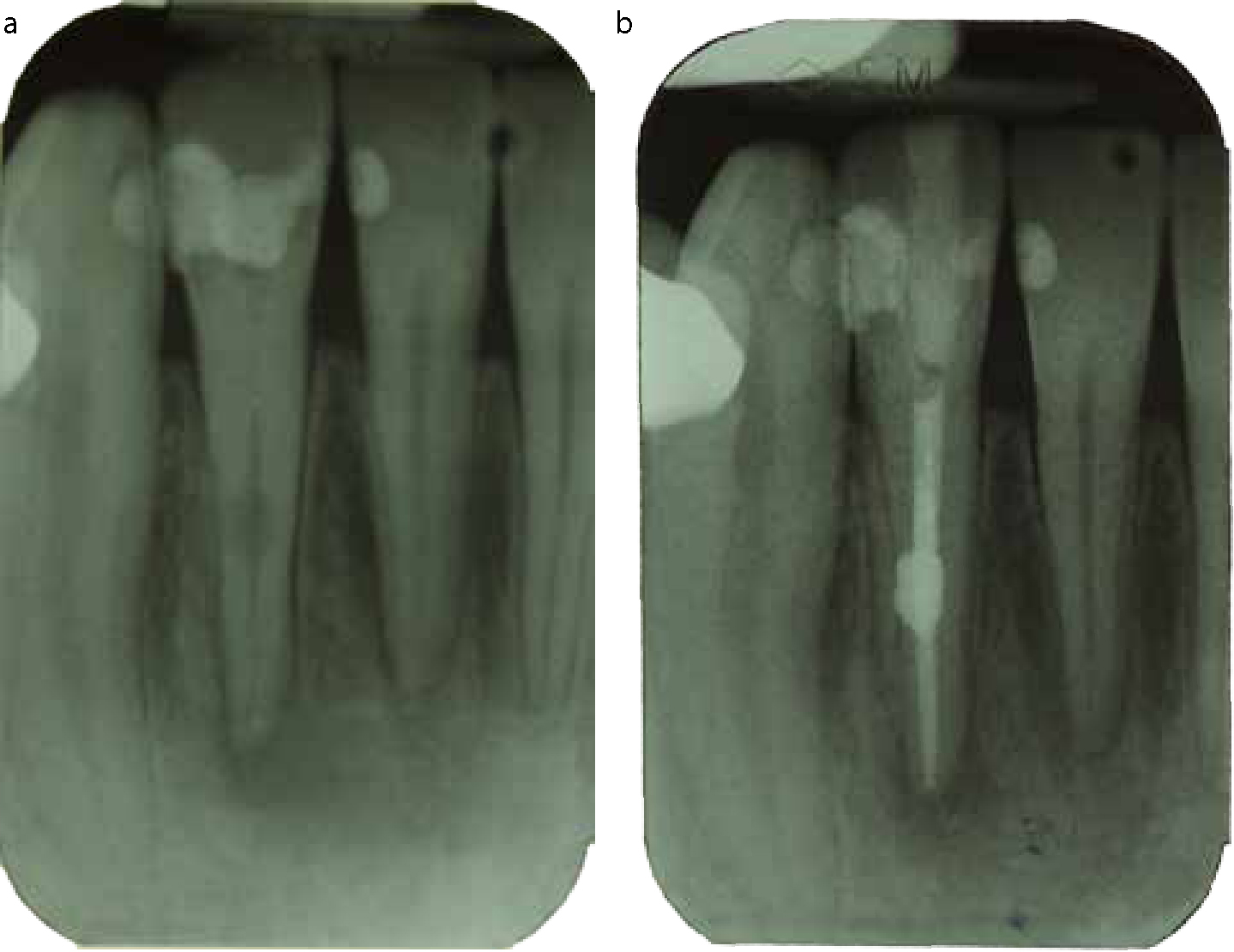
If resorption is suspected, one or more periapical radiographs should be taken. Intra-oral radiographs do not provide sufficient detail for the diagnosis of smaller lesions. Parallax radiographs should be considered as this technique will yield further information about the location and type of lesion (Figure 5). Using the principle of parallax, the shift of an external lesion can be detected. Internal lesions, however, should remain in a similar position relative to the root canal.
Figure 5. Two periapical radiographs taken from different angulations allow demonstration of severe root resorption defect, which has resulted in apical third root fracture of tooth UR1.
Role of cone beam computed tomography
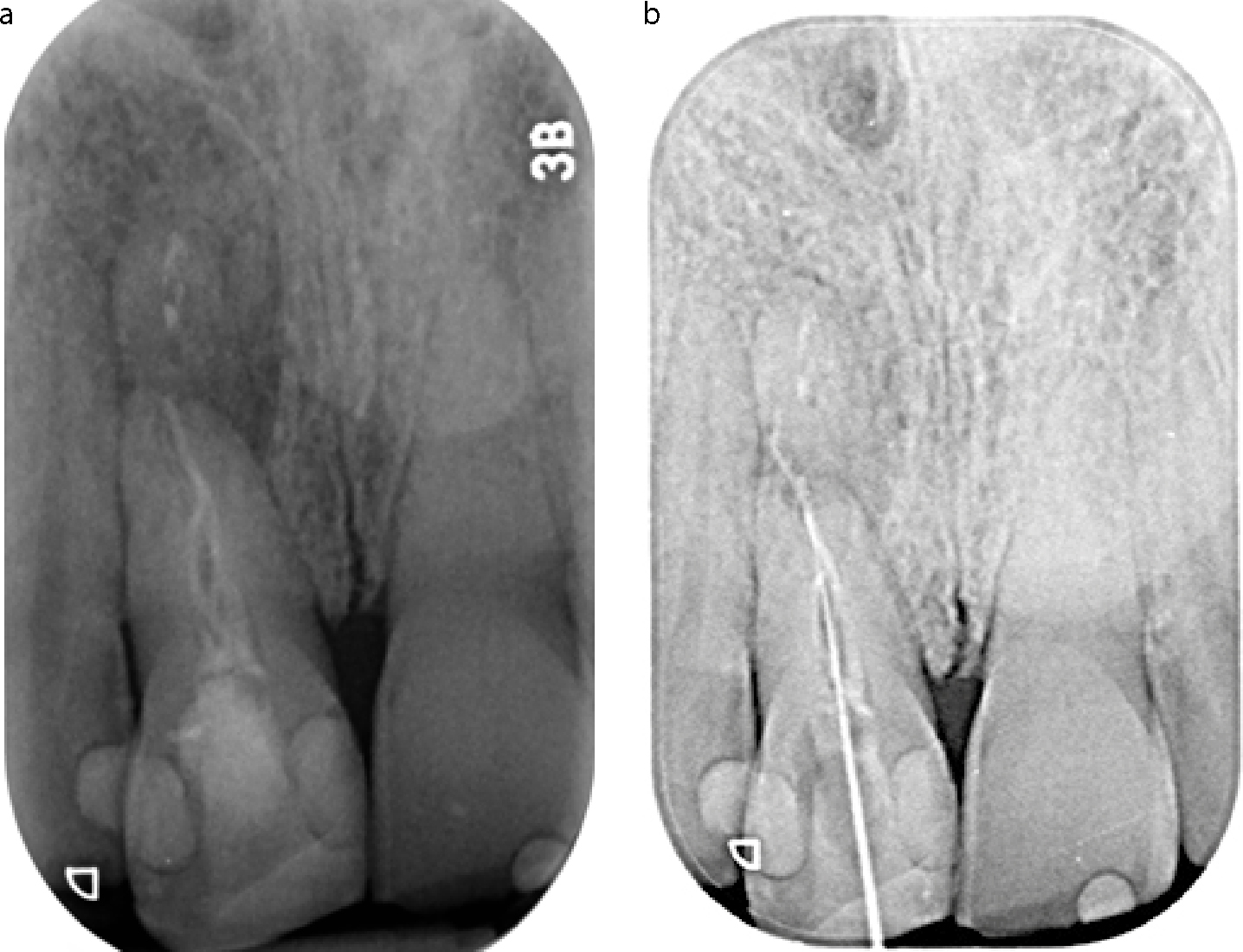
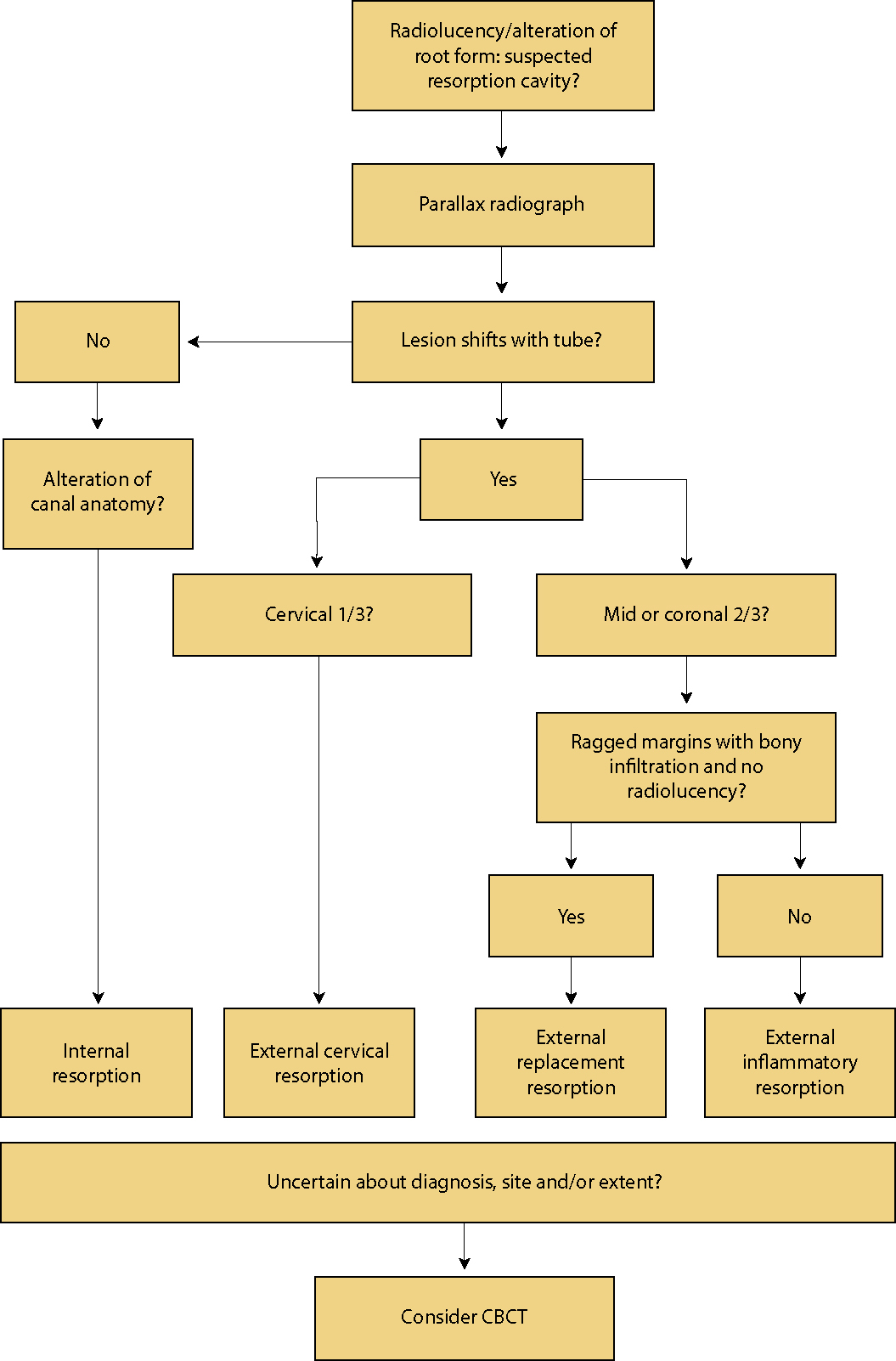
The limitations of dental radiography are widely recognized and a number of cases have demonstrated that cone beam computed tomography (CBCT) can enhance the diagnosis of resorptive lesions.16 The use of CBCT enables the precise determination of site, type and extent of the lesion and therefore CBCT can be of great value in the diagnosis, and ultimately the management, of resorption (Figure 6). As exposure to ionizing radiation must be kept to a minimum, referral for CBCT should only be made if it will be of significant assistance in diagnosis or management. Figure 7 presents a simple algorithm that may be used to help classify lesions radiographically and indicates when CBCT may be of value.14.
Figure 6.
(a) Small field of view CBCT demonstrating severe external root resorption affecting palatal aspect of UR1 (previously endodontically treated tooth displaying significant beam hardening artefact) and (b) internal root resorption perforating palatal root surface UL1.Figure 7. Algorithm to indicate requirement for CBCT.
External replacement resorption
External replacement resorption (ERR) or ankylosis is a common consequence of severe dental trauma.12 Following damage of the periodontal ligament (PDL) and cementum on the root surface, osteoclasts in direct contact with dentine progressively replace tooth substance with bone. Avulsed and re-implanted teeth with extended extra-alveolar dry time and closed apices are particularly susceptible to ERR.17 An ankylosed tooth may be diagnosed clinically within one month by its classic metallic percussion note; other clinical signs include colour change of the crown, no response to pulp tests and infraocclusion. Radiographs typically show a loss of PDL space and replacement of the root by normal trabeculated bone (Figure 8). However, as ERR is largely asymptomatic in the absence of infection, it is often observed as an incidental finding on a routine periapical radiograph. A small field of view cone beam CT scan may be helpful in determining the precise location and extent of the lesion, although there are limited in vitro studies on the use of CBCT for resorptive lesions. In terms of severe trauma like avulsion, extrusive and lateral luxations, a delay in initial treatment can negatively affect the long-term outcome. Preservation of PDL cells by storage in physiologic media or early repositioning and splinting will promote PDL repair. Covering the roots of avulsed teeth in enamel matrix derivative (Emdogain®) has been suggested as a method of encouraging periodontal regeneration and prevention of ankylosis. However, there is little evidence to demonstrate its effectiveness and currently no predictable method for arresting ERR.18
Figure 8. Replacement resorption of UR2 following lateral luxation injury. Note loss of periodontal ligament definition.
Altered tooth position
Teeth with luxation injuries and re-implanted teeth may be malpositioned. Simple restorative management for more minimal changes in tooth position may include addition of composite resin to improve the incisal edge position of intruded teeth. Similarly, in minimally extruded teeth, the removal of tooth tissue at the incisal edge may be necessary. For more significant alterations in apico-coronal tooth position, extra-coronal restorations may be indicated to improve aesthetics and occlusion. Intrusive injuries where the tooth is displaced into the fractured alveolar bone are usually impacted within the socket, with only a portion of the crown visible. Severely dislocated teeth may require surgical repositioning. By waiting for spontaneous eruption for permanent teeth with open apices or minor intrusions of fully formed teeth, if no movement occurs within a few weeks, orthodontic extrusion may be necessary. Such injuries carry a high risk of resorption, therefore orthograde root canal treatment is advised within one month. Splinting of repositioned teeth is essential and splinting times and follow-up are clearly outlined in the online Dental Trauma Guide.8 In cases where surgical or orthodontic repositioning are required, specialist referral is advised.
Soft tissue or bone deficiencies
Dental trauma may occur as part of a wider maxillofacial injury. The mechanism of injury and clinical presentation should alert the practitioner to the possibility of other injuries and a standardized clinical examination protocol in trauma cases is suggested.19 Laceration or loss of soft tissue and/or bone can accompany severe dental trauma (Figure 9). The alveolar process may be lost with the avulsed tooth or during repositioning of severely malpositioned teeth. Furthermore, early extraction will result in significant bony remodelling, with up to 63% reduction in ridge width and 22% reduction in ridge height within the first year.20 In young patients who have not yet completed growth, the bone and soft tissue deficit will become more pronounced as they mature.21 Similarly, the ankylosed re-implanted tooth that is not extracted in a timely manner may demonstrate a lack of development of the alveolus and associated gingival margin discrepancy. The extraction of these teeth may be traumatic and result in significant bone loss. The placement of implants in this clinical situation is complex. Significant pre-implant bone augmentation may be required. Bone is commonly harvested from the iliac crest or as a block graft from the mandible to replace hard tissues. An adjunctive connective tissue graft may also be necessary to increase the volume of keratinized mucosa and soft tissue profile (Figure 10). Unfortunately, in some cases where the vertical and horizontal tissue loss is so great, implant treatment may result in poor aesthetics or may not be possible at all and other prosthetic alternatives must be sought.
Figure 9. Severe intrusion injury resulting in soft tissue deficiency. (a) Patient at presentation. Distal labial luxation of UL1, complete intrusion of UL2, partial intrusion of UL3. (b) Immediately following repositioning and splinting. (c) At one month review. Gingval margin discrepancy evident in UL1, UL2. Composite additions recommended to correct incisal level. Patient did not want orthodontic repositioning.Figure 10. Previous trauma resulting in failure of tooth UR1 with significant hard and soft tissue defect development. (a, b) Clinical photographs demonstrating defects and drifting and over eruption of UR1. (c, d) Patient following extraction of UR1 and simultaneous connective tissue graft and frenectomy to allow subsequent tented membrane bone graft and implant placement. (e, f) Patient following tented membrane grafting procedure to correct hard tissue defect pre-implant placement.
Follow-up
Eighty-one percent of dental trauma occurs before the age of 30 years.22 Many facial injuries are alcohol-related23 and psychopathology has been reported among a large proportion of trauma patients.24 Patients may move for work, education or relationships and change or lapse in their dental registration. It is imperative that the importance of regular clinical and radiographic review is reinforced following dental trauma. Patients should be encouraged to take ownership for their continued dental care. Should patients not be made aware of the long-term risks, complications and importance of regular clinical and radiographic review, it is quite possible that early signs or symptoms of complications may be overlooked. Unless specifically requested, copies of patient records are not routinely transferred between dental practices in the UK. As discussed, serial radiographs are imperative to the identification of developing pathological change following trauma. If patients transfer their registration to a new dental practice, they should be advised to inform the treating practitioner, so that any previous radiographs may be requested for comparison.
Conclusion
Dental practitioners should familiarize themselves with the guidelines provided by the IADT as discussed herein. These guidelines clearly state how dental injuries should be managed, including suggested review. Dentists should be aware of which injuries are most likely to require input from specialist services. They should be aware of the relative risks of long-term complications following injury and how to identify signs or symptoms of these. Early identification of such complications should prompt referral to specialist services for management at an early stage.