Kothari P, Murphy M, Thompson J. Horizontal root fracture – an unusual complication. Br Dent J. 2012; 176:349-350
Johnson NR, Gannon OM, Savage NW, Batstone MD. Frequency of odontogenic cysts and tumors: a systematic review. J Investig Clin Dent. 2012; 5:9-14
Nayyer NV, Macluskey M, Keys W. Odontogenic cysts – an overview. Dent Update. 2012; 42:548-555
Torres-Lagares D, Segura-Egea JJ, Rodríguez-Caballero A, Llamas-Carreras JM, Gutiérrez-Pérez JL. Treatment of a large maxillary cyst with marsupialization, decompression, surgical endodontic therapy and enucleation. J Can Dent Assoc. 2012; 77
Mitchell DA. An Introduction to Oral and Maxillofacial Surgery.New York: Oxford University Press; 2006
Ertem SY, Uckan S, Ozdemir H. An unusual presentation of an intraosseous epidermoid cyst of the anterior maxilla: a case report. J Med Case Rep. 2012; 8
Takiguchi M, Fujiwara T, Sobue S, Ooshima T. Radicular cyst associated with a primary molar following pulp therapy: a case report. Int J Paed Dent. 2012; 11:452-455
Hill FJ. Cystic lesions associated with primary teeth. Proc Br Paed Soc. 2012; 8:9-12
National Institute for Health and Care Excellence. Guidance on the Extraction of Wisdom Teeth. 2000. http://nice.org.uk/guidance/ta1 (cited January 2016)
Quality guidelines for endodontic treatment: consensus report of the European Society of Endodontology. Int Endod J. 2012; 39:921-930
Moore UJ. Principles of Oral and Maxillofacial Surgery, 6th edn. Chichester: Blackwell Publishing Ltd; 2011
This article aims to illustrate and discuss the risks of failing to treat a radicular cyst appropriately. Here we report a 23-year-old male patient who sustained dental trauma to his maxillary anterior teeth on more than one occasion. The changes involved with the patient's dentition and expansion of the radicular cyst across his maxilla, over the course of a decade, highlight the importance of early intervention and appropriate treatment.
CPD/Clinical Relevance: This case report aims to alert clinicians to the risks of radicular cyst expansion, and the link between dental trauma and radicular cyst formation
Article
Cystic development related to root fracture is an unusual dental occurrence.1 Radicular cysts account for approximately 54.6% of odontogenic cysts and tumours, and are the most common cystic lesion of the jaws.2 Sixty percent are reported in the maxilla, evidently linked to pulpal necrosis of anterior maxillary teeth due to the increased prevalence of both dental trauma and dens invaginatus.3 Often, radicular cysts develop slowly, painlessly and are detected via incidental or routine radiographic finding.4 The epithelial rests of Malassez (residual cells of the root sheath of Hertwig) in the periodontal ligament form the radicular cyst epithelial lining, with a number of theories proposed for the formation of epithelial cysts.5 The differential diagnosis of anterior maxillary cystic lesions of the jaw may include: radicular, residual or lateral peridodontal cyst, odontogenic keratocyst, globulomaxillary cyst, traumatic bone cyst and ameloblastoma.6 Despite being unable to differentiate between cystic and non-cystic periapical radiolucencies using radiographic evidence alone,7 the general consensus of a well circumscribed radiolucent area bordered by a thin radio-opaque line usually symbolizes a cyst.8
Case history
2006
A 23-year-old male patient presented to the Oral and Maxillofacial Surgery outpatient clinic at Mid Yorkshire Hospitals NHS Trust in December 2006. The routine dental referral was regarding a cyst associated with the upper right central (UR1) and lateral (UR2) incisors.
The patient had no dental complaints, but revealed the history linked with these teeth. At age 15, dental trauma had been sustained to the upper right maxillary incisors, which were subsequently root-treated and restored. His referral was prompted by a further incident in June 2006, where the patient was allegedly punched in the face whilst on holiday in Mexico, leading to dislodgement of the post-crown on the UR1.
There was no relevant medical history, nor did the patient take any regular medication. The patient had no known drug allergies and smoked approximately 10 cigarettes a day. Clinical examination showed no obvious swelling or draining sinus tract, and neither the UR1 nor UR2 were tender to percussion or palpation. Both were grade II mobile, with the UR2 discoloured and the UR1 associated with a 6 mm palatal periodontal pocket.
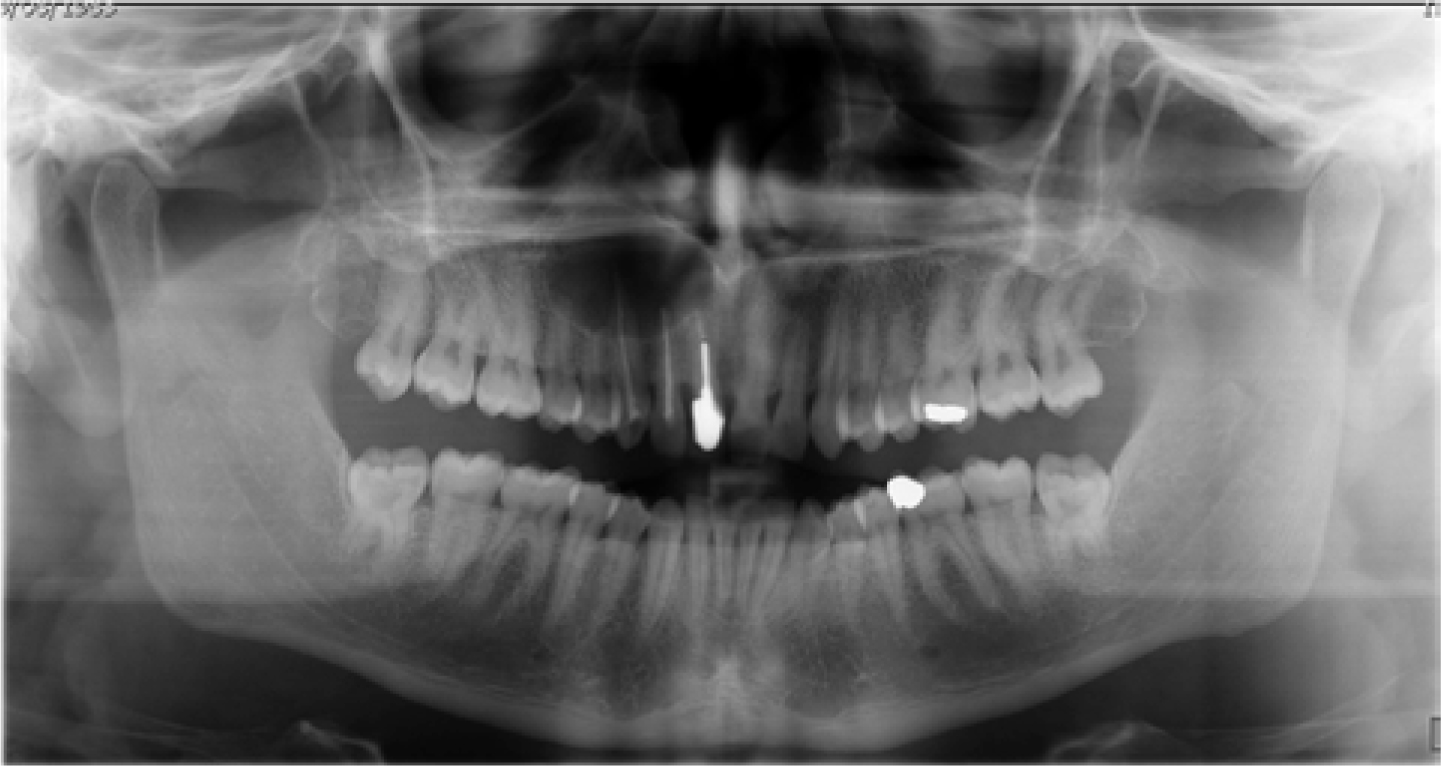
An orthopantogram (OPT) was taken (Figure 1). Radiographic examination showed a smooth, unilocular, periapical radiolucency centred over the UR2, but also involving the UR1. Both teeth appeared to be adequately root-treated, with the root-fillings extending between 0.5 and 2 mm from the radiographic apices, exhibiting good condensation with no deficiencies visible. However, judgement would ideally be reserved until a periapical radiograph was taken. The distal border of the radiolucency extended towards the apex of the upper right canine tooth (UR3). The post-crown present on the UR1 appeared to be of acceptable length, and there was strong suspicion of a vertical root fracture involving this tooth. The clinical and radiographic findings therefore led to the recommendation that the unrestorable UR1 was extracted.
Understandably, the patient was very keen to retain both teeth and refused extraction. Advice was given to the referring general dental practitioner (GDP) to investigate the UR1 further for vertical root fracture with a view to orthograde re-root treatment of the UR1 and root treatment of the UR2. The patient was subsequently discharged.
Figure 1. Orthopantomogram (OPT) taken on 12 December 2006. The radicular cyst is centred over UR2 and also involving UR1.
2009
The patient was referred to the Oral and Maxillofacial Surgery department again, but this time regarding pericoronitis associated with his wisdom teeth. Another OPT radiograph (Figure 2) was taken. Based on NICE guidelines, there was no indication for removal as he had only experienced a single episode of pericoronitis and the teeth had no other associated dental pathology.9
Figure 2. OPT taken on 15 June 2009. The radicular cyst has extended distally past the UR4 with the inferior border immersing the apical third of the UR3's root.
Radiographic examination of the OPT showed the radicular cyst associated with the UR1 and UR2 had expanded laterally across the right side of the maxilla with a well corticated border. The enlargement extended distally past the upper right first premolar (UR4) and the inferior border had surrounded the apical third of the UR3 root. It appeared that no further restorative treatment had been completed with regards to either the UR1 or UR2, and further cystic spread was likely to have devitalized the UR3. Again, the patient was not keen for any surgical treatment and hence was discharged.
2015
A new referral of the patient was made by a GDP from another practice in April 2015. The GDP stated that the patient was seen for a routine check-up, having last attended in August 2013, and the cystic lesion was noted after taking an OPT radiograph, despite the patient being asymptomatic. The letter also informed our team that the UR2 and UR3 were root-treated in 2012.
During the consultation, the patient stated that, despite being aware of the cyst in 2006, he had been unwilling to have it treated due to a variety of issues. He developed an infection of the area in 2012 which was treated with antibiotics.
Clinical examination revealed a grade III mobile crown on the UR1, but no buccal expansion or adversity was detected from the maxillary anterior teeth. Radiographic examination of the latest OPT taken (Figure 3) illustrated greater cystic expansion. The well corticated, unilocular radiolucency had extended even further distally past the upper right second premolar tooth (UR5), and was approaching the mesial and palatal roots of the upper right first molar (UR6). The image also suggests that there may have been some root resorption of UR3 and UR4. Superiorly, the cyst expansion intimated the risk of both oro-antral and oro-nasal communication if enucleated, especially due to the extension towards the nasal floor. The UR2 appeared to have had orthograde endodontic retreatment, however, on this occasion, the condensation was suboptimal. The root treatment of the UR3 fell short of the 0.5 to 2 mm ideal from the radiographic apical constriction.10 Ideally, there should be no space between the canal filling and canal wall, preventing the passage of micro-organisms and fluid along the root canal, but there was a deficiency of condensation mesially.10 Sadly, the UR1 was in the original state, as seen in 2006, but with an obvious radiolucent line visible from the base of the post, extending obliquely towards the distal aspect of the root, signifying incomplete root fracture.
Figure 3. OPT taken on 29 July 2015. The radicular cyst is enlarging: approaching the roots of UR6, perhaps causing root resorption of UR3 and UR4, and developing a greater risk of oro-antral/oro-nasal communication from surgery.
Considering the extensive nature of pathology that has developed, the treatment options were given to the patient, and he elected for surgery to have: removal of the UR1; cyst enucleation; and apicectomy and retrograde root filling of UR2 and UR3 under general anaesthetic. The GDP was asked to discuss the immediate and long-term treatment options to replace UR1 with the patient.
A further letter from the patient's GDP in October 2015 reported that the UR1 post-crown had failed and fallen out, leaving the apical portion in situ. Unfortunately, the patient has failed to attend any appointment since this date.
Discussion
Literature linking tooth fracture and odontogenic cyst development is limited.1 Despite the patient's cyst establishment reaching a 10-year history, the relevant procedure had not been carried out due to poor attendance and the patient's unwillingness to proceed. Expansion of the cyst is likely to devitalize adjacent teeth,11 and therefore increase the risks and co-morbidities associated with surgery.
This case report emphasizes a number of features to consider when a patient attends for a routine dental consultation:
Ensure a full history of any dental trauma is recorded, regardless of whether the patient is a child or adult;
Consider whether patients with maxillary anterior crowns and/or associated root canal treatment have a history of dental trauma related to these teeth;
A patient should be warned of the risks associated with a periapical lesion linked to dental trauma, including cystic change with enlargement, devitalization of adjacent teeth, and surgical risks (such as oro-antral or oro-nasal communication), especially if left untreated.
Conclusion
Ultimately, the treatment that was undertaken was limited by the patient's decision not to have treatment and, despite ensuring that the patient was aware of the risks of leaving the cyst in situ, he has failed to comply with the advice and treatment options offered. This case aims to highlight the risks in leaving a suspected radicular cyst in place and also to help practitioners provide informed consent to patients with conditions that are similar to this.