
References
Sectional fixed appliance therapy in the mixed dentition
From Volume 44, Issue 11, December 2017 | Pages 1083-1088
Article

Common dental malocclusions seen in the mixed dentition include premature loss/over-retained deciduous teeth, submerged molars, supernumerary teeth, midline diastema, crossbites, increased overjet, open bites, ectopic eruptions and crowding.1 The available scientific data suggest that malocclusions have negative effects on oral health-related quality of life, predominantly in the dimensions of emotional and social wellbeing.2 Interceptive treatment is thus recommended in order to reduce the severity of a developing malocclusion. In properly selected cases, like dental anterior crossbites or unerupted incisors, interceptive orthodontic treatment not only improves function and aesthetics, but also achieves a relatively stable outcome, even after the removal of the appliance.3
Although a comprehensive orthodontic finish without a second phase of treatment in the permanent dentition is not obtained in all cases, carefully planned interceptive treatment may help to reduce further orthodontic treatment.4
A removable appliance can be given as a mode of interceptive orthodontic treatment. Wiedel and Bondemark, through their randomized controlled trial, concluded that anterior crossbites during the mixed dentition stage can be corrected using either removable or fixed appliances with equal success rate in terms of stability.5 However, removable appliances can exert only single-point contact on teeth, leading to unsophisticated tipping movements in most cases. In addition, these appliances can be difficult for the patients to fit and will not be worn if they are either too loose or too tight. Thus, success of the interceptive treatment using a removable appliance depends upon patient compliance, both for wearing and adjusting the appliance. The treatment will not work if this co-operation is not forthcoming.6
In this regard, use of sectional fixed appliances is gaining in popularity. This appliance is versatile, easy to use and well tolerated by all patients. It also allows rapid correction of many incipient malocclusions, with a single short phase of fixed appliance therapy in the early mixed dentition stage.6
The fixed sectional appliance
The fixed sectional appliance usually takes anchorage from the maxillary molars and has brackets bonded onto maxillary anteriors. The number of maxillary anteriors to be bonded varies according to the case. The basic sectional fixed appliance design has bands cemented on both upper first permanent molars, brackets bonded onto the erupted maxillary incisors and continuous archwires to provide/maintain good arch form, as well as control of anterior teeth; 2 mm of archwire that is left protruding from the molar tubes should be annealed to allow it to be turned down hard against the tube. This step is important to prevent the archwire sliding forward (except in cases of anterior crossbite where it is desirable), thus preventing increase of arch length, trauma to the soft tissues or loss of anchorage for the molars. Supporting stainless steel tubing should be ideally placed to strengthen the long unsupported span of wire between the molars and incisors. This protects the archwire from distortion due to occlusal forces.1
When a fixed appliance includes only some of the teeth, archwire spans are longer. This gives biomechanical advantages as large moments are easy to create and the wires themselves are springier. However, this can lead to less strong appliances that get broken or displaced or that cause soft tissue irritation.7
The four cases outlined below illustrate the effectiveness and versatility of the appliance.
Case 1
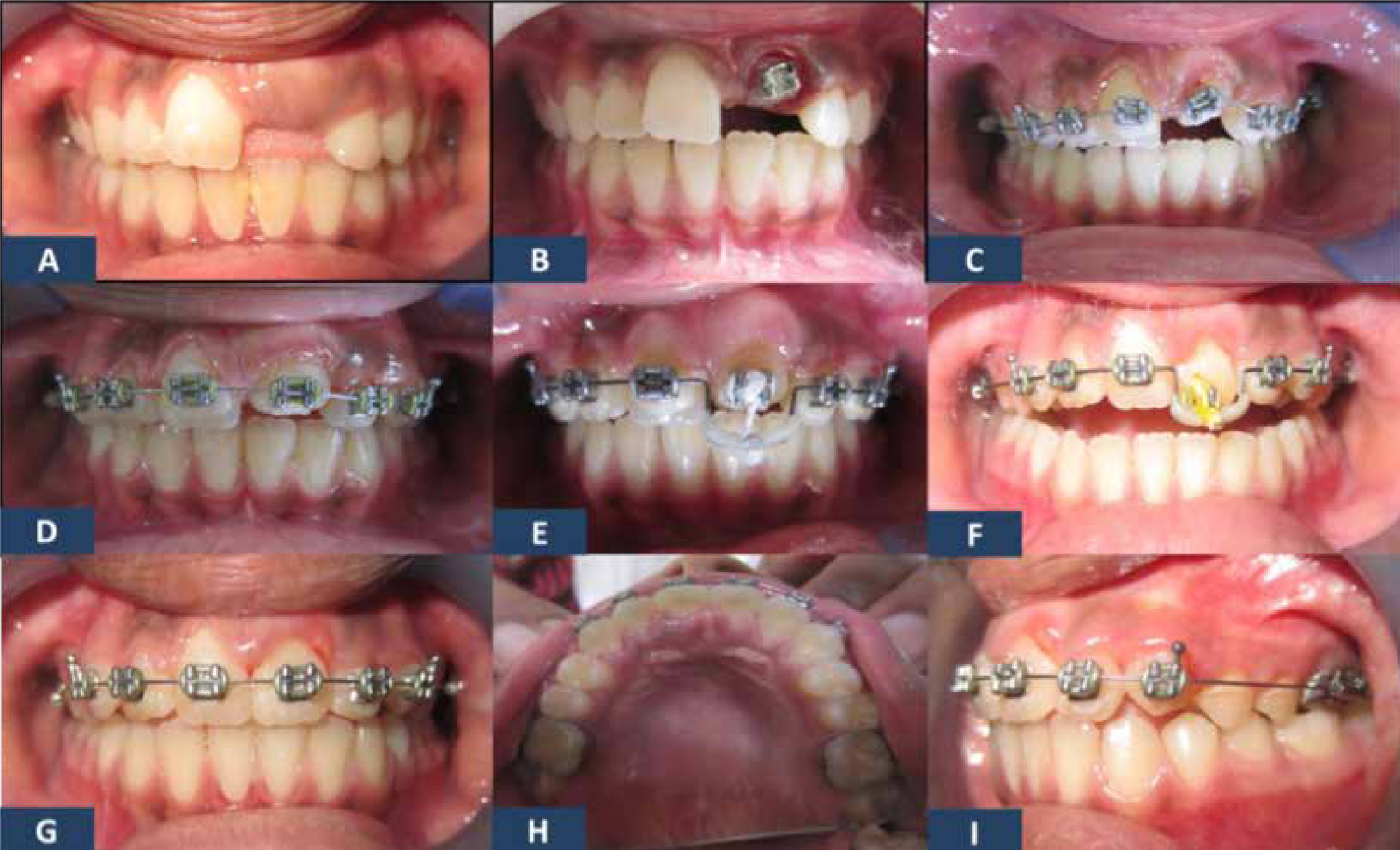
A 13-year-old female patient reported to the department with a chief complaint of an unerupted tooth. Clinical examination showed an unerupted upper left central incisor (UL1) which could be palpated clinically (Figure 1a). She had a Class I molar relationship on a Class I skeletal base. An intra-oral periapical radiograph (IOPAR) showed no supernumerary teeth or any hard tissue obstruction. The tooth UL1 was exposed with an apically repositioned flap and a straightwire bracket was attached (Figure 1b). The molars were banded. Five erupted anterior teeth were bonded, and engaged with a 0.014” round nickel titanium (NiTi) wire (Figure 1c). Two weeks later the tooth was partially erupted (Figure 1d). A 0.02” round stainless steel wire was engaged with a downward bend and tooth UL1 was engaged in that bend with an elastic thread (Figure 1e). One month after this appointment, the tooth UL1 erupted to its proper position (Figures 1g–i). No retainers were placed. The total treatment time was one and a half months.
Case 2
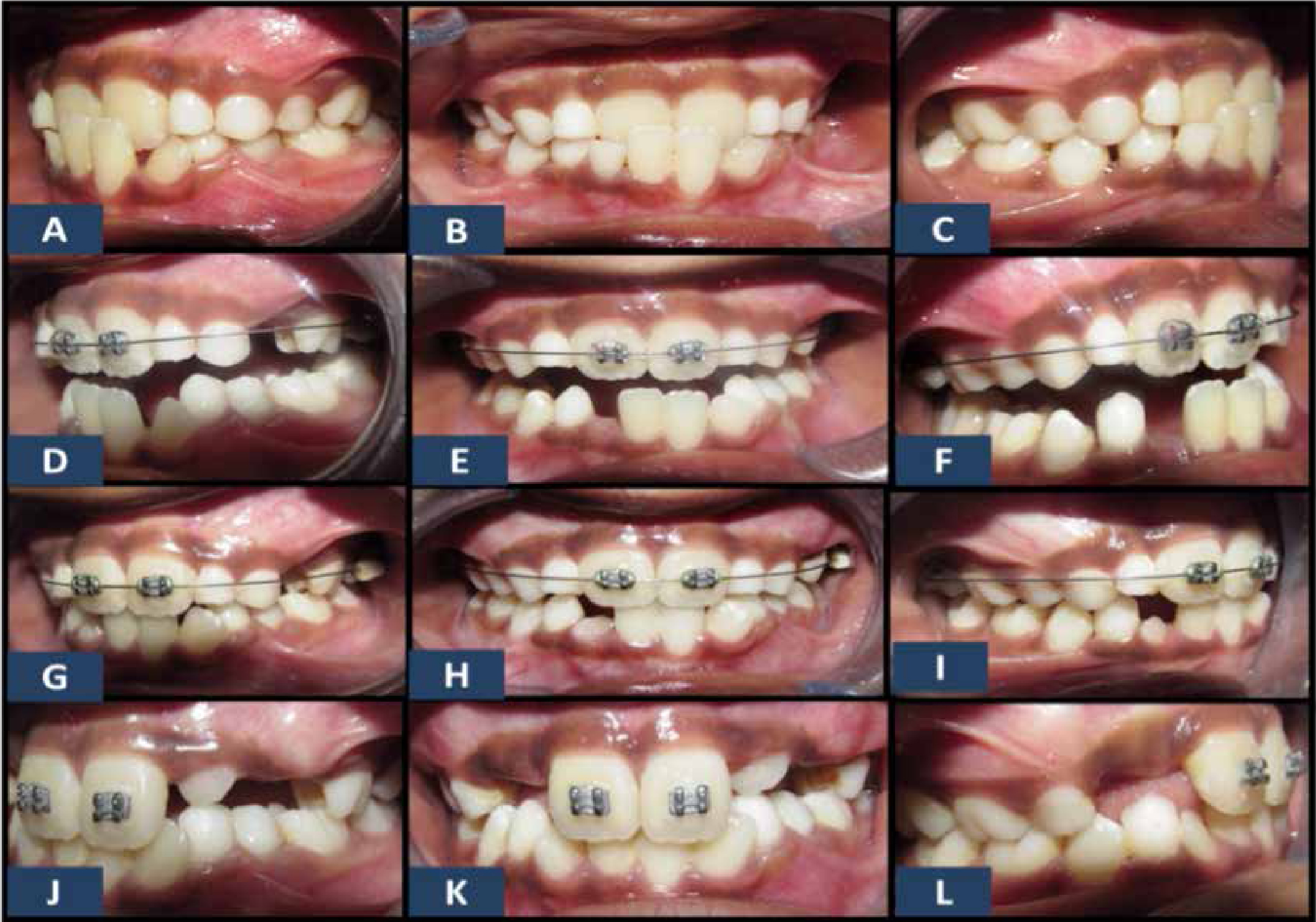
A nine-year-old female patient reported to our department with the chief complaint of malaligned teeth. Clinical examination showed dental anterior crossbite with a functional shift in relation to the upper right central incisor (UR1) and the upper left central incisor (UL1). She had a Class III incisor relationship on a Class I skeletal base (Figures 2a–c). A 2 x 2 fixed appliance was designed with straightwire brackets and bands on molars. A 0.014” round NiTi wire was engaged (Figures 2d–f). Though the bite needs to be raised to disengage the teeth in crossbite, it was not done in this case as the crossbite correction was progressing well at recalls, even without the bite disengagement. The crossbite correction was completed within one month (Figure 2g–i). No retainers were indicated in this case because of the positive overjet, with normal overbite obtained post treatment (Figure 2j–l).
Case 3
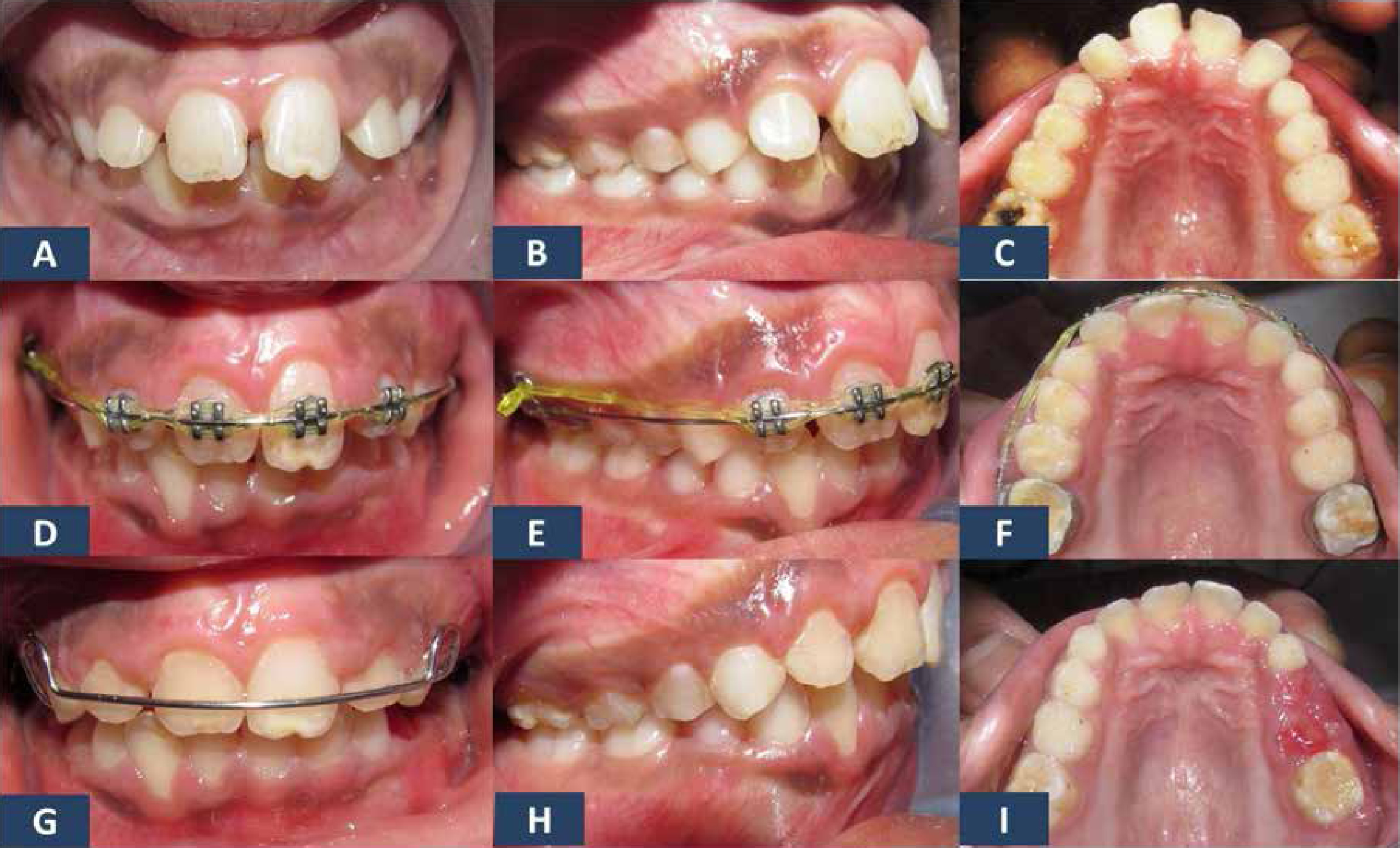
A 10-year-old male patient reported to the clinic with a chief complaint of forwardly placed upper front teeth. Clinical examination showed proclined and spaced anteriors. The ovejet was 7 mm. There was no deep bite and adequate vertical clearance was present (Figure 3a–c). There were no skeletal discrepancies and no history of thumb-sucking. Early treatment was indicated because of the potential for traumatic injuries. When the option of treatment using removable appliance was given, both the child and the parents did not prefer it. Thus a sectional fixed appliance was planned by bonding straightwire brackets on all four maxillary incisors and bonding the maxillary first permanent molars. A 0.014” round NiTi wire was initially engaged for one month followed by a 0.016” round NiTi wire for another month. After the initial levelling and alignment, a 0.02” round stainless steel round wire was then engaged and the teeth were retracted using an elastomeric chain from one side maxillary first permanent molar to the other (Figure 3d–g). The maxillary incisors were retracted over one month. A Hawley retainer was given to the child to prevent relapse and the child was put on a regular follow-up to modify the retainer whenever necessary during the transition from the mixed to the permanent dentition.
Case 4
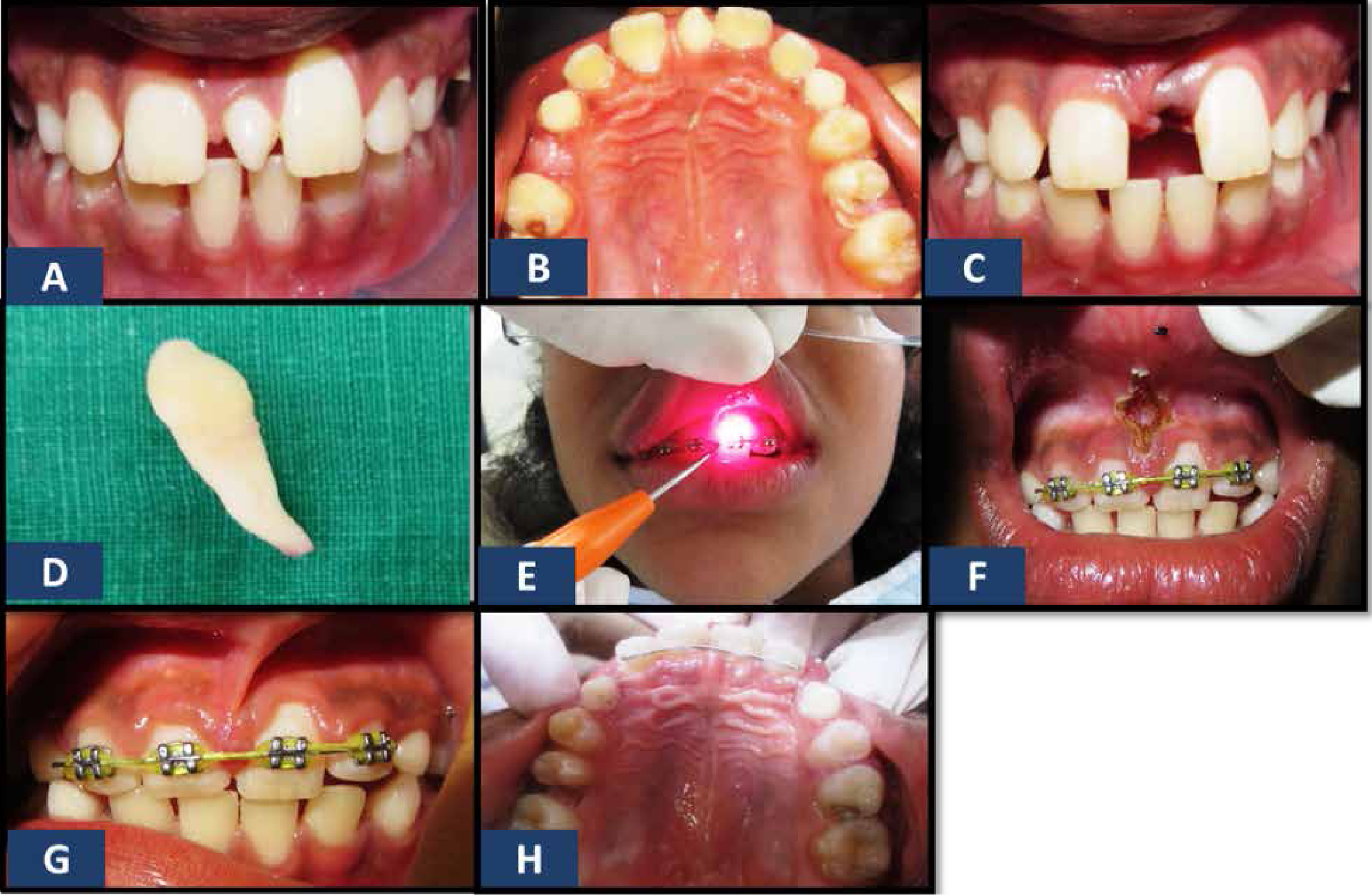
A nine-year-old female patient reported with a chief complaint of an extra tooth in the upper front tooth region. On clinical examination, a fully erupted mesiodens was seen (Figure 4a–b). The mesiodens was extracted under local anaesthesia (Figure 4c–d). The resulting midline diastema was 8 mm, the closure of which required bodily movement of the maxillary central incisors. A sectional fixed appliance was placed involving all the four maxillary incisors with a 0.02” round stainless steel wire and an elastomeric chain between them. Following space closure, frenectomy was performed using a laser (Figure 4e–g). The teeth were retained with a palatally bonded retainer (Figure 4h).
Discussion
It is important to make an annual assessment of patients in the mixed dentition to identify developing problems and, where necessary, to initiate treatment or refer to a specialist. Interceptive treatment can play a key role because early treatment can, not only correct the occlusion, but may also encourage normal development of the teeth and jaws.8
In this regard, the fixed sectional appliance used in the mixed dentition is an extremely versatile appliance. There has been much debate in the literature regarding the ideal timing of orthodontic treatment.6 According to the guidelines laid down by the British Orthodontic Society, the majority of orthodontic treatment can commence in the late mixed and early permanent dentition. However, earlier referral is needed in certain circumstances when interceptive treatment is indicated.9 While undertaking interceptive treatment, diagnosis and treatment planning play a key role and are as important as in comprehensive treatment.7
Early intervention can simplify or eliminate the need for later treatment.8 The main advantage of early treatment in properly selected cases is that it not only quickly restores anterior aesthetics, but may also reduce the complexity and duration of any subsequent treatment required. Rotations and diastemas, as well as incorrect tooth inclinations and angulations, may therefore be treated quickly using this versatile technique.6
However, in complex mixed dentition cases, a second stage of treatment in the early permanent dentition may be required, in spite of effective treatment in the mixed dentition. Hence, final finishing and root positioning is not indicated in most of the interceptive cases. Long spans of treatment can result in ‘burning out’ of the patients, as well as damaging the teeth and the supporting structures. Thus, while treating the malocclusions in the mixed dentition, it is important to have well defined goals and endpoints which should include appropriately planned treatment course, duration and mode of retention.7
During the course of fixed sectional appliance therapy, it is important to obtain radiographic images routinely, especially while moving lateral incisors that are adjacent to unerupted canines. Care must be taken so that the roots of the lateral incisors are not inadvertently tipped into the path of the erupting canines. It is also important to check for the unerupted teeth radiographically, as presence or absence can alter the course and direction of the treatment.7
The final stage of transition from mixed to the permanent dentition is an unstable period. Thus, once the treatment is complete and desired results have been achieved, retention must be planned, keeping in mind the patient's current versus initial dentition status, as well as subsequent changes in dentition and occlusion that will occur as the child matures.7
Summary
The decision to use fixed appliance sectional therapy over removable appliance therapy as a mode of interceptive orthodontic treatment should be judiciously made after considering treatment needs and patient compliance.
Cases selected for early orthodontic interventions should have well defined goals and endpoints of treatment.