Durack DT, Lukes AS, Bright DK New criteria for diagnosis of infective endocarditis: utilization of specific echocardiographic findings. Duke Endocarditis Service. Am J Med. 1994; 96:(3)200-209
Thornhill MH, Dayer MJ, Forde JM, Corey GR, Chu VH, Couper DJ Impact of the NICE guideline recommending cessation of antibiotic prophylaxis for prevention of infective endocarditis: before and after study. Br Med J. 2011; 342
Prendergast BD. The changing face of infective endocarditis. Heart. 2006; 92:(7)879-885
Habib G, Hoen B, Tornos P, Thuny F, Prendergast B, Vilacosta I Guidelines on the Prevention, Diagnosis, and Treatment of Infective Endocarditis (new version 2009): the Task Force on the Prevention, Diagnosis, and Treatment of Infective Endocarditis of the European Society of Cardiology (ESC). Endorsed by the European Society of Clinical Microbiology and Infectious Diseases (ESCMID) and the International Society of Chemotherapy (ISC) for Infection and Cancer. Eur Heart J. 2009; 30:(19)2369-2413
Griffin MR, Wilson WR, Edwards WD, O'Fallon WM, Kurland LT Infective endocarditis. Olmsted County, Minnesota, 1950 through 1981. J Am Med Assoc. 254:(9)1199-1202
Mylonakis E, Calderwood SB Infective endocarditis in adults. N Engl J Med. 2001; 345:(18)1318-1330
Strom BL, Abrutyn E, Berlin JA, Kinman JL, Feldman RS, Stolley PD Dental and cardiac risk factors for infective endocarditis. A population-based, case-control study. Ann Int Med. 1998; 129:(10)761-769
Tleyjeh IM, Steckelberg JM, Murad HS, Anavekar NS, Ghomrawi HM, Mirzoyev Z Temporal trends in infective endocarditis: a population-based study in Olmsted County, Minnesota. J Am Med Assoc. 2005; 293:(24)3022-3028
Lacassin F, Hoen B, Leport C, Selton-Suty C, Delahaye F, Goulet V Procedures associated with infective endocarditis in adults. A case control study. Eur Heart J. 1995; 16:(12)1968-1974
Lockhart PB. An analysis of bacteremias during dental extractions. A double-blind, placebo-controlled study of chlorhexidine. Arch Intern Med. 1996; 156:(5)513-520
Lockhart PB, Brennan MT, Kent ML, Norton HJ, Weinrib DA. Impact of amoxicillin prophylaxis on the incidence, nature, and duration of bacteremia in children after intubation and dental procedures. Circulation. 2004; 109:(23)2878-2884
Lockhart PB, Brennan MT, Sasser HC, Fox PC, Paster BJ, Bahrani-Mougeot FK. Bacteremia associated with toothbrushing and dental extraction. Circulation. 2008; 117:(24)3118-3125
Bahrani-Mougeot FK, Paster BJ, Coleman S, Ashar J, Barbuto S, Lockhart PB. Diverse and novel oral bacterial species in blood following dental procedures. J Clin Microbiol. 2008; 46:(6)2129-2132
Lockhart PB, Loven B, Brennan MT, Fox PC. The evidence base for the efficacy of antibiotic prophylaxis in dental practice. J Am Dent Assoc. 2007; 138:(4)458-474
Gould FK, Elliott TS, Foweraker J, Fulford M, Perry JD, Roberts GJ Guidelines for the prevention of endocarditis: report of the Working Party of the British Society for Antimicrobial Chemotherapy. J Antimicrob Chemother. 2006; 57:(6)1035-1042
Martin M. A victory for science and common sense. Br Dent J. 2006; 200:(9)
Connaughton M. Commentary: Controversies in NICE guidance on infective endocarditis. Br Med J. 2008; 336:(7647)
Wilson W, Taubert KA, Gewitz M, Lockhart PB, Baddour LM, Levison M Prevention of infective endocarditis: guidelines from the American Heart Association: a guideline from the American Heart Association Rheumatic Fever, Endocarditis, and Kawasaki Disease Committee, Council on Cardiovascular Disease in the Young, and the Council on Clinical Cardiology, Council on Cardiovascular Surgery and Anesthesia, and the Quality of Care and Outcomes Research Interdisciplinary Working Group. Circulation. 2007; 116:(15)1736-1754
National Institute for Health and Clinical Excellence. Prophylaxis against infective endocarditis 2008. www.nice.org.uk/CG064 (cited March 2008)
, 55th edn. London: Royal Pharmaceutical Society and BMJ Publishing; 2008
Brennan MT, Kent ML, Fox PC, Norton HJ, Lockhart PB. The impact of oral disease and nonsurgical treatment on bacteremia in children. J Am Dent Assoc. 2007; 138:(1)80-85
Lockhart PB, Brennan MT, Thornhill M, Michalowicz BS, Noll J, Bahrani-Mougeot FK Poor oral hygiene as a risk factor for infective endocarditis-related bacteremia. J Am Dent Assoc. 2009; 140:(10)1238-1244
Gibbs JL, Cowie M, Brooks N. Defying explanation. Br Dent J. 2006; 201:(4)
Ramsdale DR, Morrison L, Palmer MD, Fabri B. Lethal consequences. Br Dent J. 2006; 201:(4)
Richey R, Wray D, Stokes T. Prophylaxis against infective endocarditis: summary of NICE guidance. Br Med J. 2008; 336:(7647)770-771
Professor of Oral Medicine, Department of Oral and Maxillofacial Medicine and Surgery, University of Sheffield School of Clinical Dentistry, Sheffield, UK
Infective endocarditis (IE) is a serious, life-threatening disease and oral bacteria are implicated in 35-45% of cases. This has led to the development of guidelines recommending the use of antibiotic prophylaxis (AP) prior to invasive dental procedures in patients at risk of IE. There is considerable controversy about the value of AP in preventing IE, resulting in guideline changes and different guidelines in different parts of the world. In March 2008, NICE recommended the complete cessation of AP prior to dental procedures in the UK. The effects of this controversial change were not entirely as anticipated and may provide important lessons about the role of AP in preventing IE.
Clinical Relevance: The debate over the value of providing antibiotic prophylaxis to prevent infective endocarditis in patients undergoing invasive dental procedures is of importance to dentists worldwide. The effect of the NICE guidelines on antibiotic prophylaxis prescribing and incidence of infective endocarditis in the UK has contributed important new evidence to this ongoing debate.
Article
Martin H Thornhill
Infective endocarditis (IE)
Infective endocarditis (IE) is an infection of the endocardial lining of the heart. It most often affects the heart valves, where it may cause vegetations to develop. These are accumulations of platelets, fibrin and inflammatory cells that are heavily infected with micro-organisms and form fleshy lumps on the valve surfaces. These vegetations can stop the valves from working efficiently, leading to leakage, regurgitation and heart failure. In addition, they release bacteria into the circulation and fragments of the vegetations may break off, releasing infected emboli into the circulation to affect distant sites. Fortunately, IE is rare, but the diagnosis is difficult as initially the symptoms can be subtle or difficult to distinguish from other infections, these include:
Fever;
Chills and sweats;
Anorexia;
Weight loss;
Malaise; and
Non-specific pains.
However, the Duke criteria1 for the clinical diagnosis of IE have helped to improve the investigation and early diagnosis of the disease. This is important, since the early use of high dose antibiotic therapy can significantly improve outcomes. Nonetheless, IE is still associated with an acute mortality of around 17%2 and a high proportion of patients who survive will have long-standing heart valve damage that often requires surgery and is associated with reduced long-term survival. IE is therefore a serious disease and a major concern for affected patients, their cardiologists and cardiothoracic surgeons.3
Epidemiology of infective endocarditis
The epidemiology of IE has changed over recent years.4 While it was once a disease affecting young adults with existing heart valve disease, usually rheumatic valve disease, it now tends to affect older patients, particularly those with prosthetic heart valves, or those without a previous history of valve disease who have received medical interventions such as haemodialysis or intravascular devices. This may reflect the marked reduction in the incidence of rheumatic fever in industrialized countries and the increasing use of more complex surgical interventions to treat cardiovascular and other diseases. There has also been a large increase in the incidence of IE in intravenous drug users. Overall, the incidence of IE appears to be gradually rising in the UK.
The role of oral bacteria in infective endocarditis
There is irrefutable evidence that oral bacteria, usually viridians group Streptococci, are the causal organism in a significant proportion of cases of IE, with oral bacteria being isolated from blood cultures and heart valve vegetation samples. The proportion of IE cases where oral bacteria can be identified is probably in the region of 35–45%.5–9 However, many other organisms can cause IE and an increasing proportion of IE cases are associated with Staphylococcal species, particularly Staphylococcus aureus. This organism is commonly associated with the skin and its increased role in IE cases probably reflects the growing incidence of cases associated with intravenous drug use, transdermal surgical procedures and devices.
The undoubted role of oral bacteria in IE led to the hypothesis that oral bacteria enter the circulation during invasive dental procedures. This is supported by studies that have demonstrated a transient bacteraemia with oral flora following invasive dental procedures such as extractions.10–13 In turn, this led to the idea that such IE could be prevented by giving the patient a bactericidal dose of antibiotics before the procedure, so that any oral bacteria released into the circulation would be killed before they could colonize the heart valves. As a result, antibiotic prophylaxis (AP) has been the primary focus for preventing IE for more than 50 years and has resulted in the development of various national and international guidelines defining the use of AP to prevent IE developing in susceptible individuals undergoing invasive dental procedures. These have often differed considerably in their opinion about the types of patient considered to be at risk of developing IE, the dosage regime to use and the dental procedures that require cover. The problem, however, is that there is little or no firm scientific evidence to demonstrate that AP prior to invasive dental procedures is effective in preventing IE14 and, indeed, two case-control studies have provided evidence to suggest that dental treatment is unlikely to be a risk factor for IE.7,9
Antibiotic prophylaxis guidelines for preventing infective endocarditis
In the UK, a working party of the British Society for Antimicrobial Chemotherapy (BSAC) had for many years issued guidelines, which were periodically updated, on the use of AP for preventing IE in patients undergoing dental procedures. Their guidelines were incorporated into the advice published in the British National Formulary. In the USA, the American Heart Association (AHA) produced similar guidelines. In 2006, however, a BSAC working party examined the evidence for using AP to prevent IE and concluded that there was insufficient evidence to support its use to prevent IE in patients undergoing dental treatment.15 Despite reaching this conclusion, however, they withheld from recommending the complete cessation of AP and, instead, recommended restricting its use to those patients at highest risk of developing IE and who, if infected, would carry a particularly high mortality. These they defined as patients with:
A previous history of IE;
Prosthetic heart valves; or
A surgically constructed systemic or pulmonary shunt. This meant that they were recommending the cessation of AP for many patients in which it was previously recommended, such as those with heart murmurs, native valve disease or a history of rheumatic fever.
The BSAC recommendations were greeted with an editorial in the British Dental Journal entitled A Victory for Science and Common Sense16 that welcomed the recommendations and concluded with the comment, ‘BSAC did consider scrapping antibiotic prophylaxis for dental treatment, but it was a step too far at the present time, hopefully it won't be in the future.’ However, the BSAC recommendations, along with the editorial comments in the British Dental Journal, caused widespread concern amongst cardiologists, including the British Cardiac Society, British Congenital Cardiac Association and the British Cardiovascular Society.16,17 They were concerned that restricting AP for dental procedures only to those patients at highest risk would result in a dramatic increase in the incidence of IE. As a result of the concern and lobbying from cardiologists, the BSAC recommendations were put on hold and the issue was referred to the National Institute for Health and Clinical Excellence (NICE), who were asked to consider all the evidence relating to the role of AP in preventing IE and produce definitive guidance.
In the United States, the American Heart Association (AHA) guidelines committee was undergoing the same deliberations and came to a very similar conclusion to BSAC, ie they recommended the cessation of AP for patients with a history of a murmur, rheumatic fever or other evidence of native valve disease, but recommended it should continue for those patients at greatest risk from IE, such as those with a prosthetic heart valve, previous history of IE or certain congenital heart problems.18 Although this provoked considerable controversy among cardiologists in the USA, these guidelines were implemented in North America and in many other countries that take their lead from the USA in these matters.
In the UK, following an extensive investigation, NICE finally produced their guidance in March 2008.19 To the surprise of many cardiologists, the NICE guidelines went even further than the BSAC guidance and recommended the complete cessation of AP for all patients undergoing dental procedures. In addition, it recommended that AP cease for a wide range of procedures at other sites, including the upper and lower gastro-intestinal tract, genito-urinary tract (including childbirth, urological, gynaecological and obstetric procedures) and upper and lower respiratory tract (including ear, nose and throat procedures, and bronchoscopy).
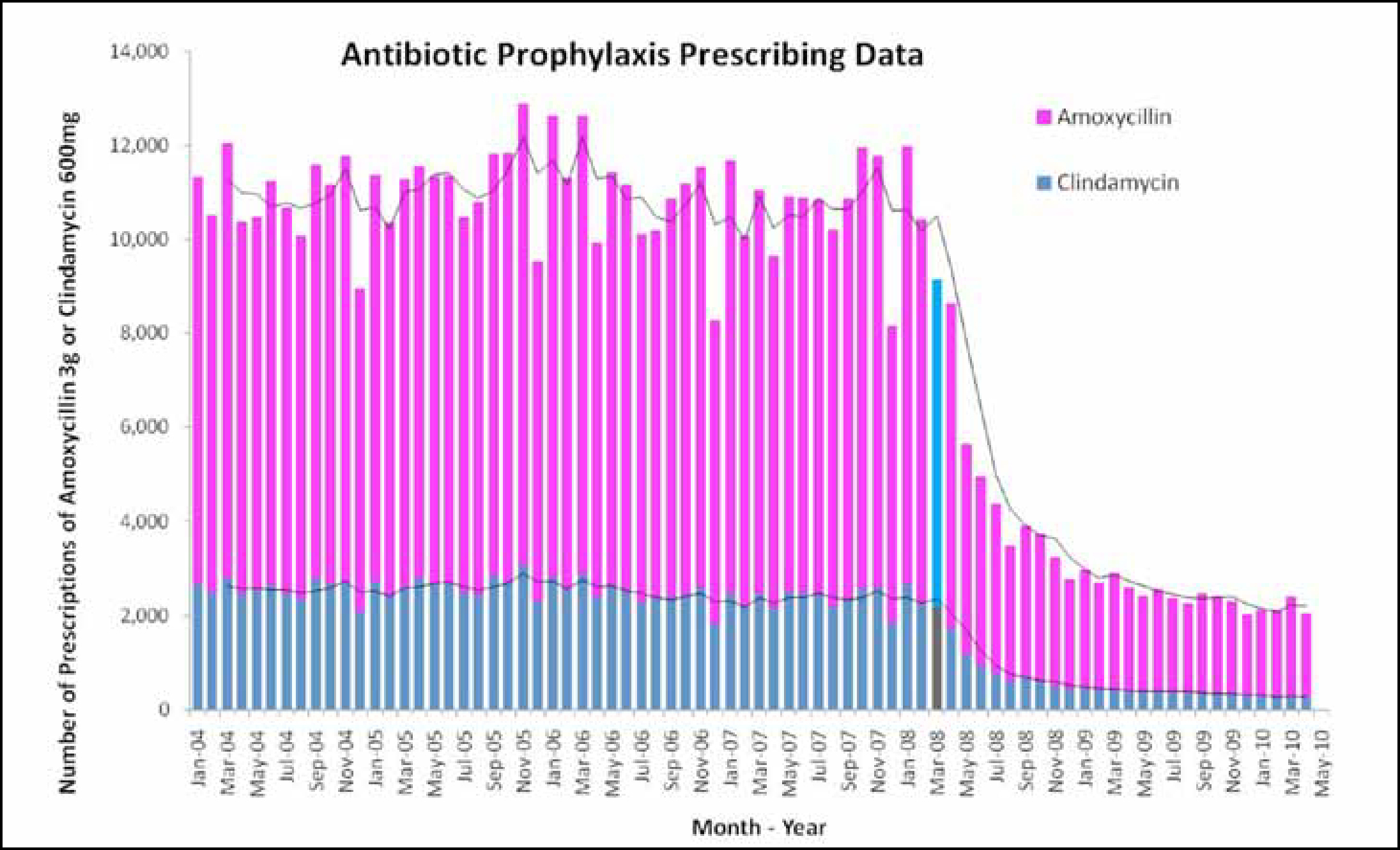
The new NICE guideline19 was followed by a letter from the Chief Dental Officer for England, dated 18th March 2008, recommending that the NICE guidance should be implemented immediately by dentists and the new guidance was immediately incorporated in the latest edition of the British National Formulary (BNF 55, published 17th March 2008).20 Most of the medical defence organizations and professional bodies also strongly advised dentists to comply with the NICE guideline and there was a rapid decline in the volume of AP prescribing (Figure 1) and it seems likely most dentists in the UK quickly adopted the new guidance summarized in Table 1.
Figure 1. The monthly number of antibiotic prophylaxis prescriptions for amoxicillin 3 g (pink bars) or clindamycin 600 mg (blue bars) prior to dental procedures. The different coloured bars indicate March 2008 when the NICE guidelines were introduced and the black lines represent the 3-month moving average figure for amoxicillin and clindamycin prescriptions.
Date
Event
April 2006
Journal of Antimicrobial Chemotherapy publishes new guidelines for the prevention of endocarditis from the British Society for Antimicrobial Chemotherapy.15 These recommend a significant reduction in the use of antibiotic prophylactic cover for dental and other procedures.
May 2006
British Dental Journal Editorial supports the new guidelines and suggests that further reductions in AP should be considered.16
August 2006
Two letters from cardiology groups published in the correspondence columns of the Br Dent J.23,24 Both highly critical of the May Br Dent J Editorial and the reduction in AP for dental procedures proposed in the new BSAC guidelines.
Spring 2006
British Cardiac Society and other cardiology groups request that the UK National Institute for Clinical Excellence (NICE) review and report on prevention of IE.
March 2008
NICE publishes its guidance19 saying that AP for dental and most other procedures is no longer required.
17 March 2008
British National Formulary (No 55) published containing the new NICE guidance not to provide AP for dental and most other procedures.20
18 March 2008
Letter sent from the Chief Dental Officer to all UK dentists alerting them to the new NICE guidance and recommending immediate implementation.
24 March 2008
Letter from Dental Protection Society (one of the 2 major medico-legal insurance organizations for dentists in the UK) advising all dentists to comply with the new NICE guidance immediately.
April 2008
Letter from the Dental Defence Union (the other medico-legal insurance organization for dentists in the UK) advising immediate compliance with the new NICE guidance.
May 2008
British Medical Journal publishes an article summarizing the new NICE guidance.25
Many cardiologists, however, remained extremely concerned. Many had hoped that NICE would overrule the BSAC recommendations and continue to recommend AP for a wide range of patients at risk of IE. Instead, NICE went even further than BSAC in reducing the use of AP. Because of its authority in the UK, however, there was little they could do to get the NICE guidelines changed or replaced.
About a year after the NICE guidelines were published, the European Society of Cardiology (ESC) published its Guidelines on the Prevention Diagnosis and Treatment of Infective Endocarditis.4 These were very similar to the AHA guidelines and recommended the cessation of AP for patients with a history of a murmur, rheumatic fever or other evidence of native valve disease, but recommended that AP should continue for patients at greatest risk from IE, such as those with a prosthetic heart valve, previous history of IE or certain congenital heart problems.
All of the guideline committees around the world have found it difficult to give definitive advice because of the lack of good quality evidence on the value of AP in preventing IE and the emotive nature of the problem. All of them have pointed out that a double blind, randomized clinical trial comparing AP to a placebo is needed to assess the value of AP definitively. However, such a trial has never happened. The problems are several fold. First, because the incidence of IE is so low, it would require an extremely large study to achieve a statistically significant result. This would make the study very expensive and, since it would need to involve a very large number of dental practices, logistically difficult to carry out. Furthermore, in countries where AP is still the ‘Standard of Care’ there are major concerns about the medico-legal consequences of a patient given a placebo developing IE and dying.
Unfortunately, the case for or against AP is heavily clouded by opinion. Those in favour of giving AP point to the devastating consequence of IE and the associated high cost of treating and caring for those that are affected by it. They argue that, if AP can prevent even a small number of IE cases, it should be used, particularly when the cost of providing AP is so low. Others argue that, without any evidence to prove that AP is effective in preventing IE, it is unnecessary and expensive. Furthermore, they argue that AP carries its own dangers and point to the risk of patients developing anaphylaxis and other adverse reactions, as well as the possibility that AP use could encourage the development of antibiotic resistant bacteria. They also point to evidence that AP may not completely prevent a bacteraemia following an invasive dental procedure and cases where IE appears to have developed in patients even where AP has been given.10–14
Most guideline committees are desperate for more evidence on which to base their guidance. Indeed, many had hoped that the decision by NICE to advocate the complete cessation of AP in the UK would result in a natural experiment that would produce the definitive evidence that was needed. Those who advocate the use of AP anticipated that the NICE guidelines would result in an increased incidence of IE and IE-related deaths in the UK, whilst those who regard AP as unnecessary predicted no change in the incidence of IE as a result of the guidelines.
The impact of the NICE guidelines on antibiotic prophylaxis
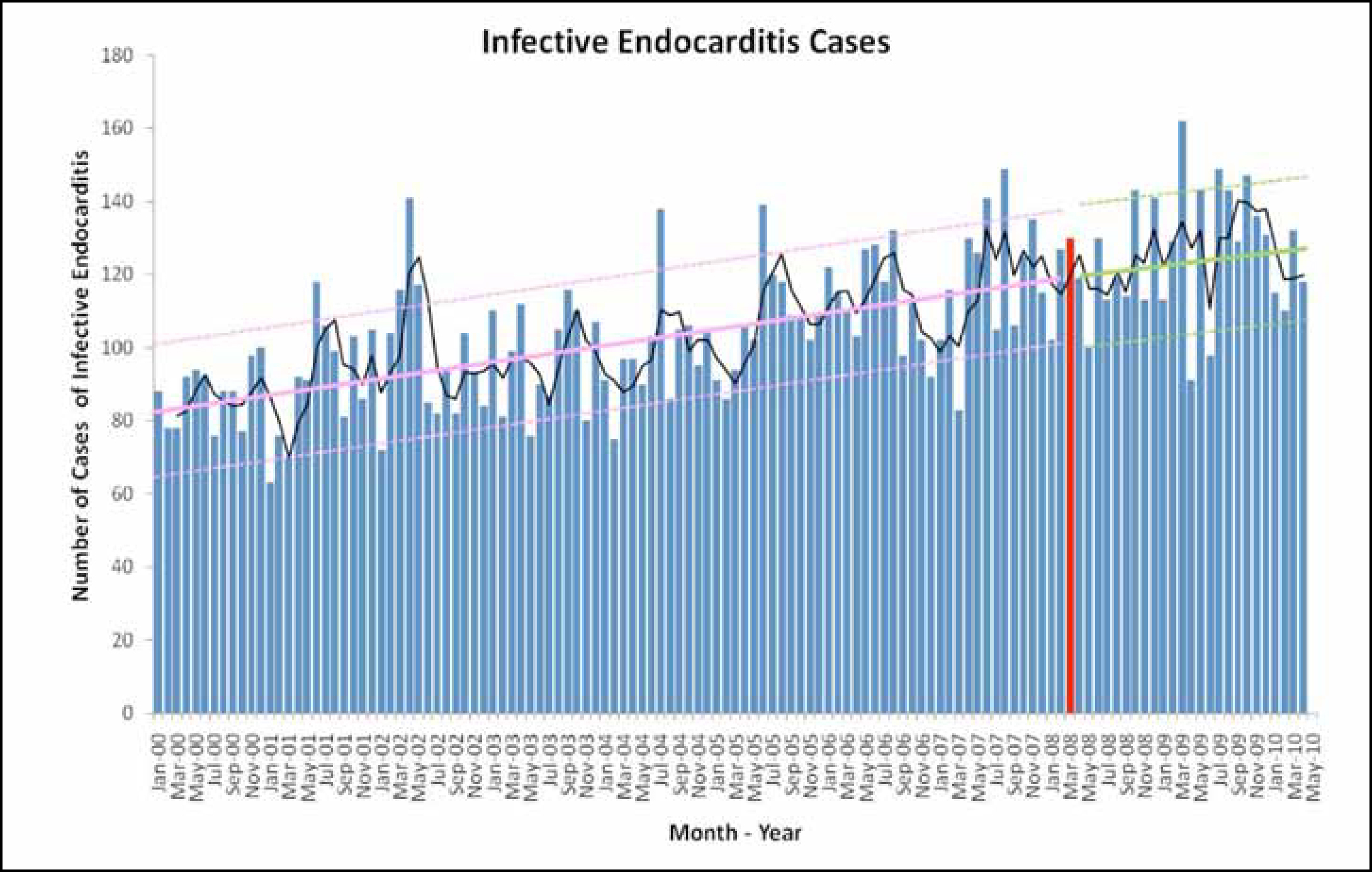
We have recently published two year follow-up data on the impact of the NICE guidelines2 in England. Following introduction of the guidelines in March 2008, there was a rapid reduction in the prescribing of AP, indicating a high level of compliance on the part of dentists (Figure 1); with dentists accounting for 91.9% of all AP prescribing. In total, AP prescribing fell from 10,727 prescriptions a month to 2,292; just 21.4% of the previous level of prescribing. In contrast, although there has been a long-term upward trend in the incidence of IE being recorded in England (Figure 2), we were unable to detect a significant further increase in the incidence of IE in the two years since the introduction of the NICE guidelines.
Figure 2. The monthly incidence figures for infective endocarditis cases (IE). The red bar represents March 2008 when the NICE guidelines were introduced. The black line represents the 3-month moving average figure for IE incidence. The pink lines represent the linear trend (+/− 2 standard deviations) for IE incidence before the NICE guidelines and the green lines represent the linear trend (+/− 2 standard deviations) for IE incidence after the NICE guidelines.
The problem of the ‘high risk’ patient
On face value this would appear to suggest that cessation of AP has not resulted in an increase in the incidence of IE. In other words, that AP is not effective in preventing IE. However, the fact that there appears to be a residual and persistent 20% level of AP prescribing, even two years after the introduction of the NICE guidelines, is a problem. It is particularly a problem because there is considerable anecdotal evidence that many cardiologists in the UK are now following the ECS or AHA guidelines instead of the NICE guidelines. In other words, although many now appear to accept that AP may not be necessary for patients with a heart murmur, history of rheumatic fever or other evidence of native valve disease, they are doing whatever they can to ensure that so called ‘high risk’ patients, such as those with prosthetic heart valves or a previous history of IE, continue to receive AP. There is also anecdotal evidence that some dentists are being pressured into prescribing AP for these patients or, when the dentist refuses to prescribe AP, the patient's cardiologist or general medical practitioner is prescribing it instead. It may not be a coincidence that these ‘high risk’ patients account for ~20% of the patients that AP used to be prescribed for, and that the reduction in AP prescribing following the NICE guidelines has stalled at ~20% of the previous level of prescribing. This means that the 2-year follow-up data following the NICE guidelines is unable to address the case of these ‘high risk’ patients and we still don't know, therefore, if AP is of value in preventing IE in these patients or not. The only way we are likely to be able to obtain this information now is through a randomized controlled trial of AP in these ‘high risk’ category patients. The lack of a significant increase in the incidence of IE in the 2 years following the introduction of the NICE guidelines does, however, suggest that AP for patients with a heart murmur, history of rheumatic fever or other evidence of native valve disease, is unlikely to be of value. Clearly, we must continue to monitor this data, and the longer this trend continues, the stronger the evidence to support this conclusion will be.
What else can be done to prevent infective endocarditis caused by oral bacteria?
If, at least in some cases, AP prior to invasive dental procedures is not effective in preventing IE, how can we explain the presence of oral bacteria in 35–45% of cases of IE? Well we do know that oral bacteria are able to enter the circulation during invasive procedures such as extractions,10–13 causing a brief bacteraemia. However, we also know that a similar bacteraemia follows a number of daily activities such as chewing food and toothbrushing.12,13,21 Furthermore, there is evidence that the extent of this bacteraemia is related to gingival health. So it is more likely that a bacteraemia will be larger and contain a more diverse spectrum of oral pathogens in an individual with poor gingival health and poor oral hygiene than in an individual with good oral hygiene and good gingival health.21,22
It is argued that the frequent bacteraemias resulting from daily activities, such as toothbrushing and mastication, pose a greater overall threat to patients at risk of IE than the rare transient bacteraemia associated with invasive dental procedures, particularly in patients with poor oral hygiene. If true, this would mean that the proportion of oral bacteria-related cases of IE prevented by AP would be very small. In those circumstances, it becomes increasingly difficult to justify the use of AP and a different strategy for preventing those cases of IE associated with oral bacteria might prove more effective. This could involve the targeted delivery of intensive oral hygiene therapy to patients at greatest risk of developing IE in order to maintain high levels of oral hygiene and gingival health and reduce the risk and size of bacteraemia associated with daily activities or invasive dental procedures.