Baron R, Ferrari S, Russell RG Denosumab and bisphosphonates: different mechanisms of action and effects. Bone. 2011; 48:(4)677-692
Appraisal Consultation Document: Denosumab for the Prevention of Osteoporotic Fractures in Postmenopausal Women. 2010;
Castellano D, Sepulveda JM, Garcia-Escobar I, Rodriguez-Antolin A, Sundlöv A, Cortes-Funes H The role of RANK-ligand inhibition in cancer: the story of denosumab. Oncologist. 2011; 16:136-145
New Drug Evaluation: Denosumab for Postmenopausal Osteoporosis. 2010;
Kyrgidis A, Toulis KA Denosumab-related osteonecrosis of the jaws. Osteoporosis Int. 2011; 22:(1)369-370
Ryan P, Saleh I, Stassen LFA Osteonecrosis of the jaw: a rare and devastating side effect of bisphosphonates. PMJ. 2009; 85:674-677
Rosen HN, Moses AC, Garber J Serum CTX: A new marker of bone resorption that shows treatment effects more often than other markers because of low coefficient of variability and large changes with bisphosphonate therapy. Calcific Tissue Int. 2000; 66:100-103
Marx RE, Cillo JE, Ulloa JJ Oral bisphosphonate-induced osteonecrosis: risk factors, prediction of risk using serum CTX testing, prevention, and treatment. J Oral Maxillofac Surg. 2007; 65:(12)2397-2410
Marx RE Current issues forum: osteonecrosis. JOMI. 2007; 22:(1)146-153
Osteonecrosis of the jaw (ONJ) following bisphosphonate use is well documented. However, to our knowledge, there are few cases reported on ONJ related to the use of other pharmaceutical agents, such as denosumab – a monoclonal antibody that is prescribed for the treatment of osteoporosis and is used as an anti-cancer agent. Here we present the first case in the UK of a patient who has developed ONJ following treatment with denosumab. The purpose of this report is to highlight the potential effects of this monoclonal antibody on bone turnover and the subsequent results of osteonecrosis of the jaw. It is hoped that this will allow early recognition by medical and dental practitioners, and appropriate referral and treatment.
Clinical Relevance: Readers should be aware of other causes of osteonecrosis of the jaw.
Article
Denosumab (Prolia®) is a monoclonal antibody that lowers osteoclast activity, by inhibiting RANK-L during osteoclastogenesis and therefore reduces bone resorption.1 In the UK, it has been authorized for the treatment of osteoporosis. It is recommended as a treatment option for the primary prevention of osteoporotic fragility fractures in post menopausal women, who are non-compliant, intolerant or have a contra-indication to bisphosphonate use. It is administered as a single subcutaneous injection into the thigh, abdomen or back of the arm. The recommended dosage is 60 mg every six months.2 The drug is also administered at higher dosages of up to 180 mg every four weeks for other conditions, including bone metastases, multiple myeloma and bone loss in men with hormone ablation in prostate cancer.3
Reported side-effects associated with denosumab treatment include arthralgia, upper respiratory tract infections and cellulitis.4 ONJ has been seen in patients taking denosumab who have received higher doses of the drug in advanced cancer treatment.5 ONJ in women receiving denosumab for post menopausal osteoporosis is rare; currently there are no cases reported in the UK.
Case report
A 79-year-old woman attended the oral and maxillofacial department at the Royal Berkshire Hospital in Reading in March 2010, following a referral from her GDP for extraction of the lower right first molar due to gross caries and a history of pain. The patient suffered from hypertension and osteoporosis and was taking regular medication of bendroflumethiazide, omeprazole and denosumab. She had been taking 60 mg denosumab subcutaneously every six months for five years, since June 2005, when she had been enrolled into the clinical trial for the drug. The patient confirmed that she had never used any form of bisphosphonates.
Surgical extraction of the lower right first molar, under antibiotic cover and using a chlorhexidine mouthwash, was performed in April 2010 with no post-operative complications.
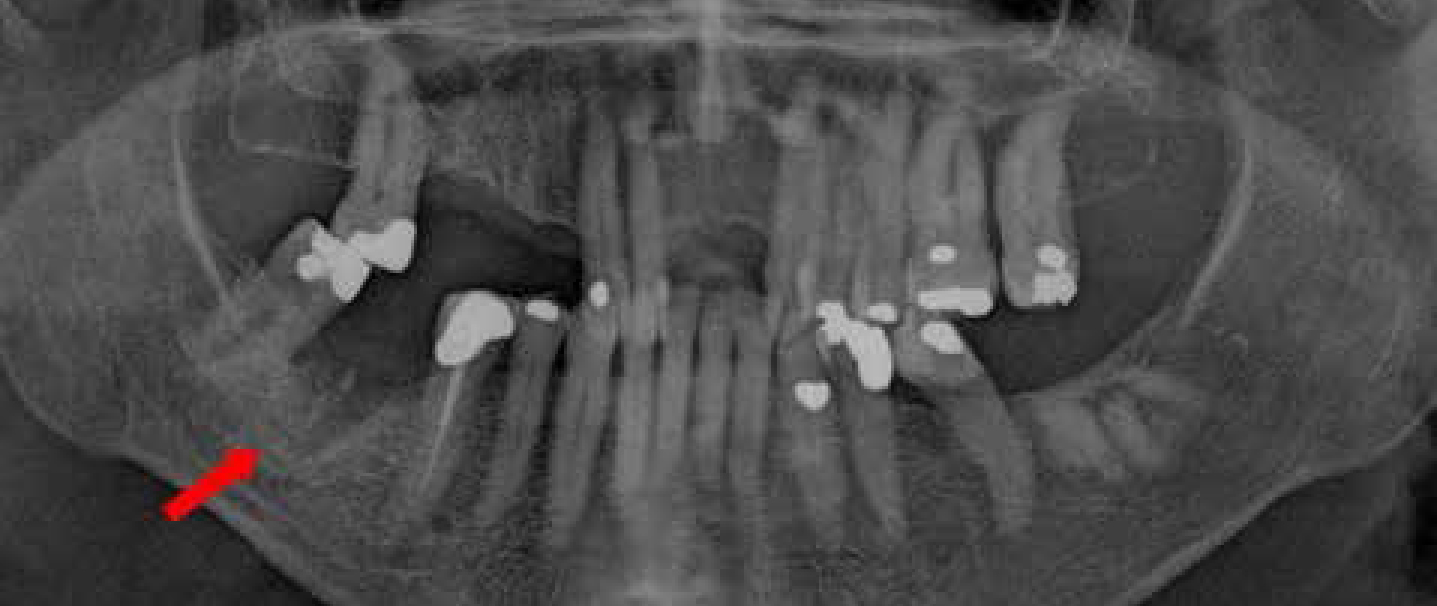
The patient then re-attended the department in January 2011 following referral from her GDP owing to delayed healing of the lower right first molar socket, which had been identified during a six month routine recall. She complained of some pain in the area. On clinical examination there was bone exposure, tenderness to palpation, as well as suppuration of the socket on pressure. A DPT radiograph was taken and this highlighted a radiolucency at the extraction site (Figure 1). The diagnosis of ONJ was then made, in line with the definition by the American Academy of Oral and Maxillofacial Surgeons (AAOMS), as an area of exposed bone in the maxillofacial region which fails to heal in eight weeks, in the absence of a history of radiotherapy to the jaws.6 However, it is to be noted that this case is ONJ due to non bisphosphonate-induced osteoclastic inhibition.
Figure 1. DPT taken ten months post extraction of the lower right first molar – radiolucency at site.
As a result of the diagnosis, an initial treatment plan of exploration and debridement of the socket under local anaesthetic was postponed and the patient was sent for a CTX (C-terminal telopeptide) serum blood test as a baseline investigation. The use of the CTX test as an indicator of the risk of ONJ is under investigation. During bone resorption, the dominant type 1 collagen is degraded, releasing the C terminal telopeptide known as CTX or CrossLaps® (Elecsys Roche Diagnostics GmbH, Mannheim, Germany). When bone turnover is decreased by a bisphosphonate, the CTX is low, and these effects are seen within weeks of beginning bisphosphonate therapy.7,8 It is reported that values of less than 100 pg/ml represent a high risk of ONJ; 100–150 pg/ml, moderate risk; and greater than 150 pg/ml, minimal or no risk. The CTX test results identified a level of 0.01 μg/l. This is equivalent to100 pg/ml. This patient was therefore identified as being at ‘high risk’ of ONJ.8,9
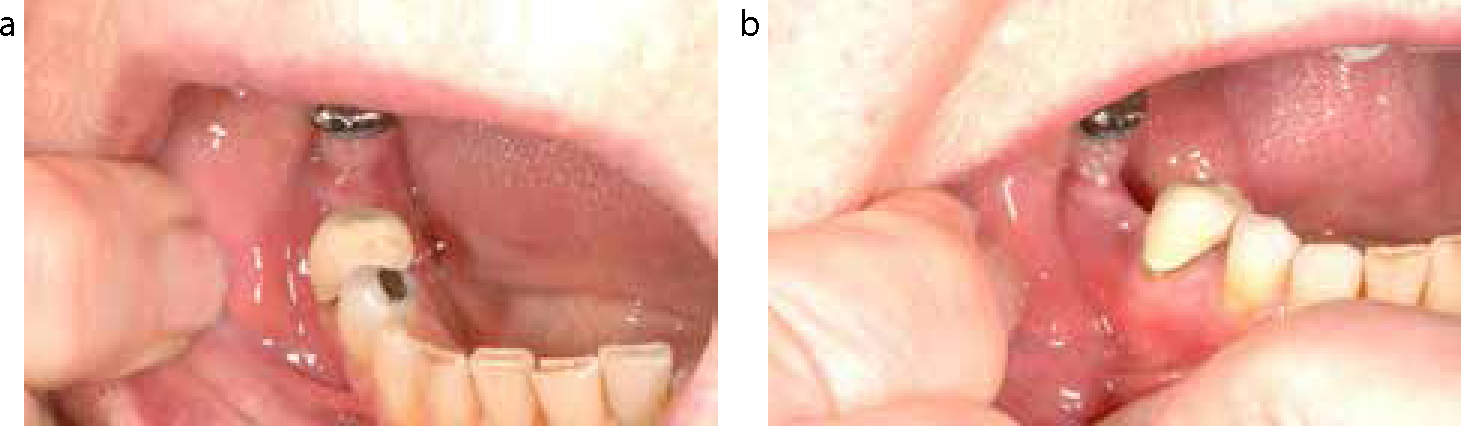
After liaison between the OMFS department and the associated drug company, the patient was advised to stop taking denosumab, ie commence a ‘drug holiday’ in February 2011. Following a review, ten months post extraction and one month after stopping denosumab, the socket appeared to be healing and there was no exposed bone (Figure 2). The patient was kept under review and the CTX test repeated as necessary. It was recommended to be repeated four months after the initial drug holiday and at four month intervals thereafter. Once the CTX value exceeded 150 pg/ml, debridement could be considered.9
Figure 2.
(a, b) Taken eleven months post extraction. The site is beginning to heal and there is no longer exposed bone, however, suppuration from the area continues.
Discussion
The effects of ONJ can be serious and lead to a long term poor quality of life. Patients should be fully informed on any prescribed drugs and their long-term effects. It is imperative that patients are seen for a full dental assessment before any drugs affecting osteoclast activity are administered so that preventive dentistry can be instigated and any teeth with a poor prognosis can be extracted in order to try and prevent future oral surgery causing ONJ. Medical and dental practitioners must recognize the significance of this drug when assessing a patient's medical history and planning treatment.
Conclusion
The authors feel there is a need for further investigation into the reliability of the CTX test for assessing the risk levels of ONJ for patients taking drugs affecting osteoclast activity. Further studies into the effects of denosumab and ONJ also need to be conducted.