Dahl E. Diagnosing inflammatory and non-inflammatory periapical disease. J Ind Dent Assoc. 1991; 70:22-26
Kuc I, Peters E, Pan J. Comparison of clinical and histologic diagnoses in periapical lesions. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 2000; 89:333-337
Peters E, Lau M. Histopathologic examination to confirm diagnosis of periapical lesions: a review. J Can Dent Assoc. 2003; 69:598-600
Bornstein MM, von Arx T, Altermatt HJ. Loss of pulp sensitivity and pain as the first symptoms of a Ewing's sarcoma in the right maxillary sinus and alveolar process: report of a case. J Endod. 2008; 34:(12)1549-1553
Lee SS, Kim HK, Choi SC, Lee JI. Granulocytic sarcoma occurring in the maxillary gingiva demonstrated by magnetic resonance imaging. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 2001; 92:(6)689-693
Levi PA, Kim DM, Harsfield SL, Jacobson ER. Squamous cell carcinoma presenting as an endodontic-periodontic lesion. J Periodontol. 2005; 76:(10)1798-1804
Torabinejad M, Rick GM. Squamous cell carcinoma of the gingiva. J Am Dent Assoc. 1980; 100:(6)870-872
Selden HS, Manhoff DT, Hatges NA, Michel RC. Metastatic carcinoma to the mandible that mimicked pulpal/periodontal disease. J Endod. 1998; 24:(4)267-270
Thompson IO, Phillips VM, Kalan M. Metastatic squamous carcinoma manifesting as a periapical lesion. J Dent Assoc S Afr. 1992; 47:(11)481-483
Nevins A, Ruden S, Pruden P, Kerpel S. Metastatic carcinoma of the mandible mimicking periapical lesion of endodontic origin. Endod Dent Traumatol. 1988; 4:(5)238-239
Dhanrajani PJ, Abdulkarim SA. Multiple myeloma presenting as a periapical lesion in the mandible. Ind J Dent Res. 1997; 8:(2)58-61
Shah N, Sarkar C. Plasmacytoma of anterior maxilla mimicking periapical cyst. Endod Dent Traumatol. 1992; 8:(1)39-41
Heng CK, Heng J. Implications of malignant lymphoma on a periapical mandibular lesion. Gen Dent. 1995; 43:(5)454-458
Bavitz JB, Patterson DW, Sorensen S. Non-Hodgkin's lymphoma disguised as odontogenic pain. J Am Dent Assoc. 1992; 123:(3)99-100
Graham RM, Thomson EF, Cousin GC, Kumar SN, Awasthi A. A case of facial lymphoma mimicking dental infection. Dent Update. 2009; 36:(4)244-246
Morgan LA. Infiltrate of chronic lymphocytic leukemia appearing as a periapical radiolucent lesion. J Endod. 1995; 21:(9)475-478
Jee A, Domboski M, Milobsky SA. Malignant fibrohistocytoma of the maxilla presenting with endodontically involved teeth. Oral Surg Oral Med Oral Pathol. 1978; 45:(3)464-469
Powell CA, Stanley CM, Bannister SR, McDonnell HT, Moritz AJ, Deas DE. Palatal neurofibroma associated with localized periodontitis. J Periodontol. 2006; 77:(2)310-315
Ardekian L, Rachmiel A, Rosen D, Abu-el-Naaj I, Peled M, Laufer D. Burkitt's lymphoma of the oral cavity in Israel. J Craniomaxillofac Surg. 1999; 27:(5)294-297
Martins MD, Taghloubi SA, Bussadori SK, Fernandes KPS, Palo RM, Martins MAT. Intraosseous schwannoma mimicking a periapical lesion on the adjacent tooth: case report. Int Endod J. 2007; 40:72-78
Buric N, Jovanovic G, Pesic Z, Krasic D, Radovanovic Z, Mihailovic D, Tijanic M. Mandible schwannoma (neurilemmoma) presenting as periapical lesion. Dentomaxillofac Radiol. 2009; 38:178-181
Noel KE, Mardirossian G, Schneider L. Primary intraosseous kaposi's sarcoma presenting as an asymptomatic periapical radiolucency: a case report. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 2007; 103:65-70
Chen YK, Chen CH, Lin CC, Hsue SS, Lin YR, Lin LM. Central adenoid cystic carcinoma of the mandible manifesting as an endodontic lesion. Int Endod J. 2004; 37:711-716
Osteosarcoma of the mandible mimicking an odontogenic abscess: a case report and review of the literature Chetan J Bhadage Sagar Vaishampayan Swapnil Kolhe Hemant Umarji Dental Update 2025 40:3, 216-221.
Authors
Chetan JBhadage
BDS, MDS, Reader
Department of Oral Medicine and Radiology, MGV's KBH Dental College and Hospital, Nashik
Inflammatory lesions, like periapical/odontogenic abscesses, are by far the most common pathologic condition of the jaws. Radiographically, these lesions commonly manifest as widening of periodontal ligament space, discontinuity of lamina dura and ill-defined periapical radiolucency. There are some rare disorders which could cause similar radiographic changes in the jaw bone. With careful scrutiny of periapical radiolucency, regular periodic follow-up radiographs and histo-pathologic examination, the periapical abscess or infection can be differentiated from rare fatal disorders.
Clinical Relevance: This paper highlights the need for vigilant examination of even the commonest, innocuous-appearing periapical changes which sometimes are produced by some rare fatal disorders.
Article
Radiolucent shadows are cast over the periapical regions of teeth in practically all oral radiographic surveys of dentulous patients. Some of these periapical radiolucencies represent innocent anatomic variations, whereas others are caused by benign conditions and require treatment to preserve the associated teeth; still others represent systemic disease conditions that often become the responsibility and obligation of the dental clinician to recognize and bring to the attention of the patient's physician.1
The high incidence and broad spectrum of conditions causing periapical radiolucencies make it imperative that all dental clinicians should acquire a broad and comprehensive working knowledge of the conditions responsible for creating periapical radiolucent shadows.
This paper presents a case of osteosarcoma of the mandible that was first diagnosed and treated as a dental periapical lesion and discusses similar rare cases.
Case report
A 29-year-old Indian female patient reported to the Oral Medicine, Diagnosis and Radiology Department of Government Dental College Mumbai, with the complaint of a non-healing extraction wound in the right mandibular posterior region one month post-extraction with numbness over the right side of her lower lip for two months.
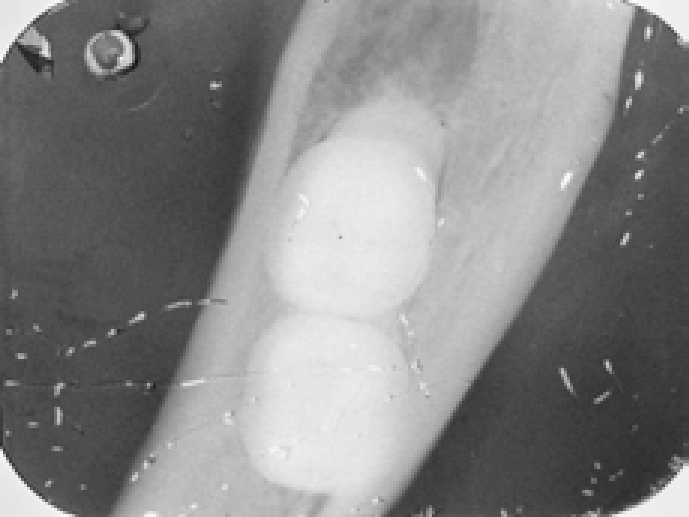
Two months earlier, the patient had attended a local dentist for pain in the above-mentioned area. The periapical radiograph (Figure 1) suggested diffuse bone rarefaction in the periapical region of LR8. The patient was followed up by extraction of the tooth. However, the patient did not experience any improvement in the symptoms. Later she noticed a small oval ulcerating growth arising from the extraction socket. This was slightly tender and slowly increasing in size.
Figure 1. Periapical radiograph showing diffuse bone rarefaction of LR8 and distal root resorption with LR7.
The patient was in good health with no previous history of radiation and was not suffering from any systemic illness. A thorough general examination was carried out and no abnormalities were detected in the patient. An extra-oral examination revealed a palpable, non tender, freely movable right submandibular lymph node. An intra-oral examination revealed an oval-shaped proliferating ulcer in relation with the region of LR8 (Figure 2). The lesion was tender, about 2cm x 2cm in size with soft to firm consistency. The margin and base of the ulcer were greyish white in colour with a normal appearing periphery.
Figure 2. Proliferating ulcer arising from extraction socket.
From the clinical examination, a provisional diagnosis of ‘reactive granuloma arising from extraction socket’ was made. As the ulcer was originating from an extraction socket, the possibility of central malignancy was also considered.
A biopsy of the ulcerated area was carried out and radiographic examination revealed loss of lamina dura in the apical third of LR7 with distal root resorption and ill-defined periapical radiolucency (Figure 3). The LR8 region showed an extraction socket with ill-defined periapical radiolucency.
Figure 3. Post-extraction radiograph showing diffuse periapical rarefaction with mesial and distal root and distal root resorption with LR7 and diffuse rarefaction and extraction socket with LR8 region.
An OPG showed an ill-defined periapical lesion with LR7 and LR8 (Figure 4). There was external root resorption with the distal root of LR7. The OPG also revealed thinning of inferior border of the mandible in the LR8 region.
Figure 4. Cropped OPG showing ill-defined periapical lesion with LR7 and LR8. External root resorption with distal root of LR7 and thinning of inferior border of mandible in LR8 region.
A mandibular occlusal radiograph showed no evidence of cortical plate expansion or periosteal bone reaction (Figure 5).
Figure 5. Mandibular occlusal radiograph.
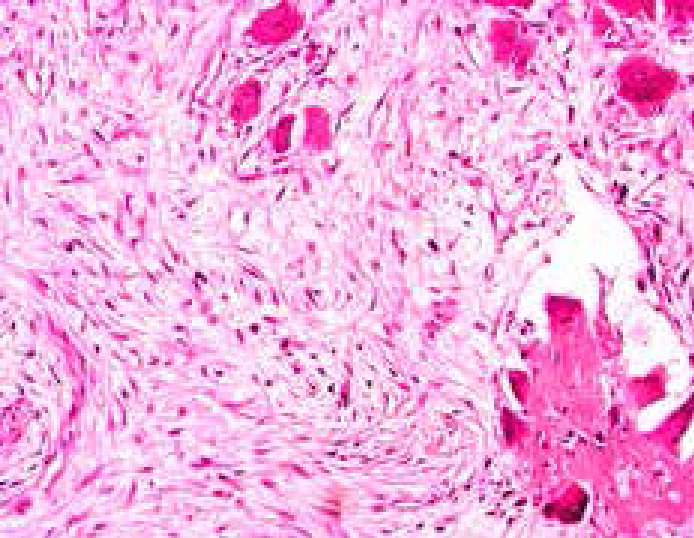
After careful scrutiny, radiographic diagnosis of chronic osteomyelitis and a differential diagnosis of a centrally arising malignancy of the mandible was given. Incisional biopsy revealed osteogenic sarcoma (Figure 6). The patient was then referred for further treatment.
Figure 6. Histopathological appearance of osteosarcoma.
Discussion
Most pathosis in the periapical region is a consequence of dental pulp necrosis. However, there are other pathoses that occur in this site with no relationship to the pulp condition.2,3,4 These non-endodontic lesions will not heal following root canal treatment or extraction. A review of the English-language medical literature, using the Medline database, revealed few rare lesions mimicking an odontogenic abscess. A list of such lesions is presented in Table 1.
Ill-defined radiolucencies associated with the tooth
Adenoid cystic carcinoma
The majority of these case reports emphasized the importance of careful scrutiny of each periapical radiolucency. All the authors stressed the significance of regular follow-ups and histopathologic examination.
Conclusion
It is important to reiterate at least three precepts pertaining to the treatment of radiolucent lesions of the jaws:1
For any periapical radiolucency that is treated by endodontic treatment of the associated tooth, follow-up radiographs should be taken.
If the clinician believes that curettage, with or without root resection, is needed to complement the canal obliteration, the periapical tissue must be subjected to microscopic examination.
If the clinician chooses to extract the tooth, the periapical lesion should also be removed and studied microscopically.
All dentists encounter periapical radiolucency on a day-to-day basis and malignancies represent a small group of these periapical shadows. Early detection and recognition represent a basis for successful treatment.