Díaz-Guzmán LM, Castellanos-Suárez JI. Lesions of the oral mucosa and periodontal disease behavior in pregnant patients. Med Oral Patol Oral Cir Bucal. 2004; 9:430-437
Lee A, McWilliams M, Janchar T. Care of the pregnant patient in the dental office. Dent Clin North Am. 1999; 43:485-494
Giglio JA, Lanni SM, Laskin DM, Giglio NW. Oral health care for the pregnant patient. J Can Dent Assoc. 2009; 75:43-48
Haas DA, Pynn BR, Sands TD. Drug use for the pregnant or lactating mother. Gen Dent. 2000; 48:54-60
Abbott P. Are dental radiographs safe?. Aust Dent J. 2000; 45:208-213
McCollough CH, Schueler BA, Atwell TD, Braun NN, Regner DM, Brown DL, LeRoy AJ. Radiation exposure and pregnancy: when should we be concerned?. Radiographics. 2007; 27:909-917
Pregnancy is a period of both joy and anxiety in a woman's life and is characterized by various physiological changes in her body brought about by the circulating female sex hormones. The oral cavity is also the seat of changes and these physiologic changes of pregnancy need to be addressed while managing the pregnant woman in the dental clinic. The main goal is to minimize the occurrence of any complications that might harm the mother-to-be and/or the unborn child. Preventive, emergency, and routine dental procedures are all deemed suitable during various phases of pregnancy, with some treatment modifications and initial planning.
Clinical Relevance: The dentist should be in a position to manage pregnant women in clinical practice effectively.
Article
Ajay G Nayak, Ceena Denny and Veena KM
Pregnancy is a special period in a woman's life where the maintenance of health is as important as the joys of impending motherhood. Therefore, understanding the changes that occur within the pregnant woman's body is of prime importance for any clinician attempting to deliver quality care. These changes are primarily affected by the circulating sex hormones, oestrogen and progesterone.1 Traditionally, dentists have exhibited reluctance on their part in providing treatment to pregnant women, mainly due to uncertainty of the risks involving two individuals, the woman and the unborn foetus, and also due to the myths prevalent about pregnancy itself.2 The vast body of literature has shown beyond doubt that the oral health of pregnant mothers has a major impact on the health of their infants. This fact highlights the heightened need for a pregnant woman to receive routine dental care throughout her pregnancy.
Maternal changes in pregnancy
Pregnancy is not considered a medically compromised state anymore, rather an extension of the healthy state.3 The physiologic changes of various systems can cause certain symptoms like nausea, vomiting, nasal congestion, heartburn, alteration in taste and food craving, hyperventilation and shortness of breath, and fatigue. The cardiovascular, endocrine, haematologic, respiratory, gastro-intestinal and genito-urinary systems are the generally affected body systems (Table 1). As the pregnancy progresses, the cardiac output of the mother steadily increases by 30–50%, with a concomitant 20–30% increase in the heart rate.1 There is a decrease in the blood pressure, especially in the second and third trimesters, while the patient is in a supine position. This is due to decreased venous return to the heart from the compression of the abdominal aorta and inferior vena cava by the gravid uterus, which can result in 14% reduction in cardiac output. Hypotension, bradycardia and syncope characterize supine hypotension syndrome.2
1st Trimester
2nd Trimester
3rd Trimester
Fatigue, backaches, mood swings
Gradually getting used to changes
Definite physical alterations
Nausea and vomiting/morning sickness
Stabilizing of systemic changes
Significant increase in weight
Frequent urge to urinate Dizziness
Physical changes begin appearing
Difficulty in moving around
Snacking binges
Uterus becomes more gravid
Danger of premature labour
Foetal organogenesis begins
Development of the foetal systems
Almost completion of foetal development
Hypertension during pregnancy
Hypertension in pregnancy is generally categorized into women who had hypertension before pregnancy and those women who become hypertensive during pregnancy. Women with high blood pressure values prior to the 20th week of gestation are assumed to have pre-existing hypertension. However, any pregnant woman with elevated blood pressure should be referred to her obstetrician to be evaluated for the possible development of pre-eclampsia, observed in 5% of all pregnancies, which manifests as a triad of hypertension, proteinuria and oedema.1
Supine hypotension syndrome
During the second and third trimesters, a decrease in blood pressure and cardiac output can occur while the patient is in a supine position. This is due to decreased venous return to the heart from the compression of the abdominal aorta and the inferior vena cava by the gravid uterus, resulting in 14% reduction in cardiac output. Hypotension, bradycardia and syncope characterize the supine hypotension syndrome. Supine hypotension can be relieved by placing the patient in a 5–15% tilted position on to her left side. If this manoeuvre does not relieve the hypotension, a full lateral position should be adopted by the patient.2
Nausea and vomiting
Vomiting occurs in about two-thirds of pregnant women, beginning approximately 5 weeks after the last menstrual period and peaking between 8 and 12 weeks. This is the result of action of progesterone and oestrogen. The lowered tone of the oesophageal sphincter, the elevated gastric pressure and slowing of gastric emptying causes increased episodes of gastric reflux, heart burn and regurgitation. Preventing gastric content aspiration during any procedure is a major concern when treating pregnant women. Maternal death after aspiration has been reported in 10–25% of all such cases and therefore antacids and H2 antagonists like ranitidine are used to prevent such incidents.4
Hyperemesis gravidarium (morning sickness) occurs in the majority of pregnant women, and for them it is best to avoid morning dental appointment completely. The patient should be advised to avoid citrus drinks or fatty foods as such foods may cause gastric upset due to delayed gastric emptying. To prevent dehydration, pregnant women should be advised to sip small volumes of liquid often. If any vomiting occurs, all procedures should be stopped immediately and the patient should be repositioned upright.1
Haematological changes
In pregnancy, the plasma volume increases significantly, without a corresponding increase in the red cell volume, thereby manifesting as anaemia.1 The other haematological changes in pregnancy include increase in the number of white blood cells, ESR, and the coagulation factors, except for factors XI and XIII. This increase in the clotting factors (VII–X) and the decrease in the anticlotting factors (XI and XIII) increases the risk of thrombo-embolism in a pregnant patient. Hence, to prevent any untoward embolic events, subcutaneous low molecular weight heparin may have to be administered to the patient, under medical supervision, as this does not cross the placenta.1
Gestational diabetes
Gestational diabetes occurs in nearly half of pregnant women and is due to the inability of the pregnant woman's body to produce sufficient amounts of insulin needed to overcome the antagonist action of oestrogen and progesterone. Moreover, obesity and a positive history of Type II diabetes seem to predispose women to gestational diabetes.1,2
Oral changes in pregnancy
There is an old wives' tale about losing a tooth for each child that a woman bears. The erroneous belief being that the developing child's calcium needs are fuelled by absorption from the mother's teeth. While that tale is just a myth, the fact remains that pregnancy can exacerbate dental problems and therefore the dental clinician should be aware of the changes occurring within the oral cavity of a pregnant woman.
Pregnancy gingivitis
Pregnancy-related changes are most frequent and most marked in the periodontium. Pregnancy, by itself, does not cause gingivitis, but can aggravate pre-existing gingival disease.4 The typical appearance of pregnancy gingivitis is that the gingiva is dark red, swollen, smooth and bleeds on minor irritation. These gingival changes usually resolve within a few months of delivery, but only if local irritants are eliminated. It has been recently proved that women with periodontal disease have an increased risk of delivering pre-term (before completion of the nine months gestation) with lower than normal birth-weight of the infant.4 Therefore, treatment of periodontal disease in pregnant women is of clinical significance and can have a positive effect upon the incidence of pre-term births.
Pregnancy granuloma or pregnancy tumour
Pregnancy granuloma is a reactive lesion, usually to local irritation or trauma and, in spite of the terminology, is neither a true neoplasm nor a true granuloma. They usually develop in the first trimester and their incidence increases up through the seventh month of gestation, mirroring the increasing levels of oestrogen and progesterone as the pregnancy progresses. The hormonal influence acts by an intense inflammatory response and by a selective growth of some periodontal pathogens and aggressive microbes, like Prevotella intermedia.5 Clinically, it manifests as a mass of variable size that has a tendency to bleed and may also interfere with mastication (Figure 1). Microscopy of such masses shows the presence of an inflammatory component characterized by lymphocytes, plasma cells and neutrophils, coupled with an abundant vascular component comprising newly formed capillaries and proliferating fibroblasts. After childbirth, when the hormonal levels normalize, such pyogenic granulomas generally resolve without treatment. Some may undergo a fibrous maturation and then resemble a fibroma. However, a thorough dental prophylaxis and oral hygiene instructions decrease the size of the lesion that does not regress. If the mass still persists then surgical removal may be performed for aesthetic reasons.2
Figure 1. Pregnancy tumour/granuloma seen as a sessile outgrowth of the buccal gingiva extending occlusally and almost covering the tooth, as seen towards the end of the second trimester of pregnancy.
Salivary glands
Both major and minor salivary glands may be affected, manifesting as changes in salivary pH and the composition causing a resultant decrease in sodium levels, increased protein concentration, and an increase in salivary oestrogen levels. All these changes combined contribute to an increase in proliferation and desquamation of the oral mucosa.1
Caries
The number of salivary cariogenic micro-organisms may increase in pregnancy, a consequence of the decreased salivary pH and buffer effect, hence these changes in salivary composition in pregnancy may temporarily predispose to dental caries and erosion. The urge to snack frequently may also contribute to an increased rate of decay. These untoward effects, however, can be easily avoided by practising good oral hygiene.5
Benign migratory glossitis
A significant prevalence of benign migratory glossitis has been observed and recently reported in pregnant women.4 It is seen on the dorsum of the tongue and is characterized by focal areas of depapillation with yellowish elevated margins of hyperkeratotic papillae.1 Taste alterations may be reported by some patients and may be consequent to changes in the tongue papillae. There may be a concurrent symptom of burning sensation that coincides with the onset of the pregnancy and subsides after delivery.
General guidelines for management in the dental clinic
An accurate history is of paramount importance at the first visit. All details regarding past pregnancies must be elicited and any complications that occurred then need to be noted. If this is the patient's first pregnancy, then further caution should be exercised as no past history exists. Details of the patient's attending gynaecologist should be noted in the patient's records, so that any appropriate clarification or consultation may be sought. The patient's home schedule for oral hygiene maintenance measures must be enquired into and necessary reinforcements regarding their importance should be made. Dietary considerations must be looked into and adequate nutrition must be stressed.1
Treatment guidelines according to the trimester
All dental appointments for the pregnant woman should be short to avoid development of fatigue. Incidence of mood swings and irritability are common in pregnancy and these should be taken into consideration when setting up appointments.1,5 During the first trimester (from the conception to the 14th week), it is prudent to educate the patient to be prepared for the impending oral changes,6 to advise to prevent occurrence of any orofacial infections that might jeopardize the health of both the mother and the unborn child and to avoid unnecessary use of drugs and radiographs. Dental hygiene procedures such as oral prophylaxis (scaling and root planing) are permissible as they minimize the bacterial load of pathogens, thereby reducing the occurrence of pregnancy-related periodontal problems.5,6 Radiography, in the first trimester, should be generally avoided but, if deemed essential, the patient should compulsorily wear a lead apron and radiation exposure should be kept to a minimum with only necessary views, never a full-mouth series. Emergency problems that arise should not be deferred to be managed in the second trimester but should be alleviated immediately.2 Elective restorative care may be undertaken with precautions, however, extensive restorative work should not be undertaken in this trimester.
The second trimester (14th to 28th week of gestation) is the most amenable period in which to perform dental treatment procedures.1–6 Any treatment that was deferred in the first trimester should be performed now. Reinforcement of the oral hygiene measures should be done in this trimester. If gingival inflammation persists, oral prophylaxis may be repeated. Radiographs can be obtained with necessary precautions.
The third trimester (29th week to childbirth) is when the patient has the most discomfort, especially towards the end of the pregnancy. The increased body weight of the patient may cause her difficulty in fitting within the confines of the dental chair. Therefore elective dental treatment should be avoided in the last month and can be postponed till a few weeks after delivery. Also, if the patient is laid flat on her back for prolonged periods, the gravid uterus may compress the abdominal aorta and inferior vena cava, leading to supine hypotension syndrome.2 In such situations, it is advisable to discontinue all dental procedures and make the patient lie in the left lateral position (Figure 2) with gentle elevation of the dental chair head.
Figure 2. The left lateral position to be adopted if the patient develops supine hypotension.
Drug prescription in pregnancy
Prescribing drugs to a pregnant woman requires caution and the clinician needs to bear in mind many factors, especially the risk versus benefit consideration (Table 2). Certain drugs have been known to cause miscarriage, teratogenecity and low birth-weight of the neonate. Moreover, drugs are absorbed more easily during pregnancy as the serum concentration for drug binding is much lower than in the non-pregnant state.1,3 Therefore, it is always prudent to obtain a clearance from the patient's obstetrician and physician.
Group of drugs
Safe to use
Unsafe/Contra-indicated
Analgesics
Paracetamol (all trimesters)Ibuprofen (1st and 2nd trimester)
For painful conditions in the oral cavity, non-steroidal anti-inflammatory group of drugs (NSAIDs) are the preferred drugs, which also constitute the most commonly prescribed group of drugs by the dental clinician. However, not all the drugs in this group are safe, some are to be avoided in all trimesters of pregnancy, while some are contra-indicated in specific trimesters.7 Paracetamol (at therapeutic ranges of 500–1000 mg) is considered safe in all three trimesters of pregnancy, however, for short-term usage only, while Ibuprofen (400–600 mg) is considered a risk in the first trimester and definitely contra-indicated in the last trimester because of its associated risks like prolonged labour, haemorrhage, premature closure of ductus arteriosus and pulmonary hypertension in the foetus.7,8 Aspirin is compatible at low doses (40–150 mg/day), but there exists a risk for use of higher doses in the first and third trimesters, as well as during the nursing period, as it is also known to cause constriction of ductus arteriosus, prolong gestation and delay labour.8 NSAIDs can also cause gastro-intestinal complications in the patient.1 Since many NSAIDs are available as over-the-counter medications, the patient should be made aware of their implications and warned strictly not to use them for longer periods and, even for the short-term, only under strict supervision.
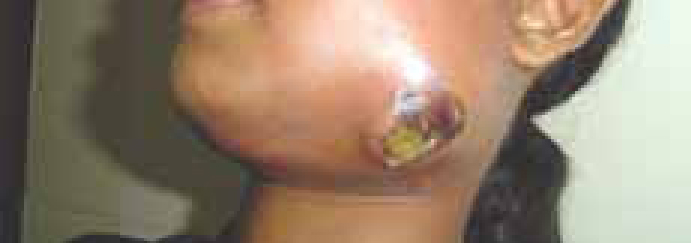
Infections occurring in the pregnancy should always be combated at the earliest opportunity and this is best done by the judicious use of antimicrobials. Infections that are neglected may spread to contiguous tissues (Figure 3) and pose a threat to both the mother and the unborn child. In orofacial infections, the penicillin group (Amoxicillin and Ampicillin) and cephalosporins (oral – Cephalexin; parenteral – Cefotaxime and Ceftriaxone) are the preferred antibiotics.2,8 If the pregnant patient is allergic to penicillin, then erythromycin (stearate salt only), azithromycin or clindamycin can be prescribed. Despite their efficacy, the tetracycline group of drugs is not prescribed to a pregnant woman, given their association with bone and dental abnormalities in the foetus and instances of maternal liver toxicity.8 Topical application of antifungal drugs, like nystatin or clotrimazole, are considered to be safe in pregnancy, while ketoconazole may cause adrenal insufficiency and hepatotoxicity, and therefore is best avoided.8
Figure 3. Neglect of oral hygiene measures and fear of dental treatment procedures lead to severe fascial space infection in the eighth month of pregnancy, which could have been easily prevented.
Local anaesthetics, like lignocaine and prilocaine, are safe for use in pregnant women who do not have any specific contra-indications, such as allergy.2,6,7 Vasoconstrictors such as epinephrine, when used in low concentration, do not cause any foetal harm, but that does not preclude necessary precautions, like avoiding injection into the blood vessels by aspirating in at least two different directions and maintaining total dosages at or below therapeutic ranges.2
Anxiolytics, such as Alprazolam and diazepam, are completely contra-indicated in pregnancy owing to reports of foetal malformations and developmental anomalies in the foetus.8
Radiography for the pregnant patient
Providing dental care in pregnancy may necessitate the dentist to obtain radiographic images of the orofacial structures, using ionizing radiation, to arrive at a correct diagnosis and to formulate an effective management strategy. In such a scenario it is extremely important for dentists to have a clear perception of the actual risks and benefits of performing radiographic studies during pregnancy. The patient or her relatives, having read unreliable information either in print or on the internet, may be wary of the procedures involving x-rays. It is the duty of the attending dentist to clarify any misconceptions that may have arisen in the patient's mind.9
Ionizing radiation (x-ray) is composed of high-energy photons that are capable of damaging DNA and generating caustic free radicals.9,10 A patient's dose of photons is measured in grays (Gy) and the rem, or in the older and more commonly recognized unit, the rad. The estimated foetal dose from dental radiograph is about 0.0001 rad for about 50,000 examinations. Foetal risk is considered to be negligible at 5 rad or less when compared to the other risks of pregnancy, and the risk of malformations is significantly increased above control levels only at doses above 15 rad.10 Radiation exposures greater than 500 mGy are known to cause foetal damage. The most sensitive period for inducing developmental abnormalities is during the period of organogenesis in the first trimester, between 18 and 45 days of gestation, and the most vulnerable period for radiation-induced central nervous system damage is 8–15 weeks after conception. Adverse foetal effects associated with radiation exposure include small size of the head, mental retardation, intellectual deficits, or induction of childhood malignancies. Therefore, the radiation risk depends upon the gestational age at the time of exposure, foetal cellular repair mechanisms, and the absorbed radiation dose level.10 Even though the exposure dose for full mouth dental radiographs (0.25μGy) is negligible to cause any abnormalities to the foetus, it is absolutely essential for the dentist to ensure that the pregnant patient avoids the smallest unnecessary dose of radiation by following the principle of ALARA (As Low As Reasonably Achievable). Radiographs must not be requisitioned unless absolutely necessary and retakes must be avoided at all costs. Protective measures, such as wearing lead aprons and a thyroid shield, combined with the use of high speed films (E/F speed) and rectangular collimator should help reduce the dose to a minimum.9,10
Conclusion
Pregnancy is a major event in a woman's life and a time when oral health care is of prime importance. The pregnant patient should not be denied appropriate treatment for the sole reason that she is pregnant. It is always wise to err on the side of caution and utilize a conservative approach in management. This brief overview should help refamiliarize the dental practitioner with the appropriate decision-making in providing oral care, especially the medications available to treat a gravid patient, with their inherent risks and benefits as they relate to the changing maternal-foetal physiology.