Rebelo MAB, Rebelo Vieira JM, Pereira JV Does oral health influence school performance and school attendance? A systematic review and meta-analysis. Int J Paediatr Dent. 2018; https://doi.org/10.1111/ipd.12441
Quadri MFA, Ahmad B. Elucidating the impact of dental caries, pain and treatment on academic performance in children. Int J Paediatr Dent. 2023; https://doi.org/10.1111/ipd.13060
Gilchrist F, Marshman Z, Deery C, Rodd HD. The impact of dental caries on children and young people: what they have to say?. Int J Paediatr Dent. 2015; 25:327-338 https://doi.org/10.1111/ipd.12186
Abed R, Bernabe E, Sabbah W. Family impacts of severe dental caries among children in the United Kingdom. Int J Environ Res Public Health. 2019; 17 https://doi.org/10.3390/ijerph17010109
Rodd H, Hall M, Deery C ‘I felt weird and wobbly.’ Child-reported impacts associated with a dental general anaesthetic. Br Dent J. 2014; 216 https://doi.org/10.1038/sj.bdj.2014.333
Feu D, Lessa FCR, Barcellos LA The impact on the quality of life caused by the early loss of primary molars. Int J Dent Hyg. 2022; 20:620-626 https://doi.org/10.1111/idh.12568
Delvecchio E, Salcuni S, Lis A hospitalized children: anxiety, coping strategies, and pretend play. Front Public Health. 2019; 7 https://doi.org/10.3389/fpubh.2019.00250
Brown N, Fenton R, Harford S. Impact of the Covid pandemic on health care equity in NHS General Dental Practice. Community Dent Health. 2022; 39:181-186 https://doi.org/10.1922/CDH_00226Brown06
Iheozor-Ejiofor Z, Worthington HV, Walsh T Water fluoridation for the prevention of dental caries. Cochrane Database Syst Rev. 2015; 2015:(6) https://doi.org/10.1002/14651858.CD010856.pub2
Elmer TB, Langford JW, Morris AJ. An alternative marker for the effectiveness of water fluoridation: hospital extraction rates for dental decay, a two-region study. Br Dent J. 2014; 216 https://doi.org/10.1038/sj.bdj.2014.180
Roberts DJ, Massey V, Morris J The effect of community water fluoridation on dental caries in children and young people in England: an ecological study. J Public Health (Oxf). 2023; 45:462-469 https://doi.org/10.1093/pubmed/fdac066
Evaluation of water fluoridation scheme in Cumbria: the CATFISH prospective longitudinal cohort study. 2022. www.ncbi.nlm.nih.gov/books/NBK586987/ (accessed June 2023)
Henein C, Landes D. NHS dental activity: a population marker for the effectiveness of community water fluoridation in children in England. Br Dent J. 2022; https://doi.org/10.1038/s41415-021-3822-1
McLaren L, McNeil DA, Potestio M Equity in children's dental caries before and after cessation of community water fluoridation: differential impact by dental insurance status and geographic material deprivation. Int J Equity Health. 2016; 15 https://doi.org/10.1186/s12939-016-0312-1
Kim HN, Kim JH, Kim SY, Kim JB. associations of community water fluoridation with caries prevalence and oral health inequality in children. Int J Environ Res Public Health. 2017; 14 https://doi.org/10.3390/ijerph14060631
Matsuo G, Aida J, Osaka K, Rozier RG. Effects of community water fluoridation on dental caries disparities in adolescents. Int J Environ Res Public Health. 2020; 17 https://doi.org/10.3390/ijerph17062020
Sagheri D, McLoughlin J, Clarkson JJ. A comparison of dental caries levels in two communities with different oral health prevention strategies stratified in different social classes. J Public Health Dent. 2007; 67:1-7 https://doi.org/10.1111/j.1752-7325.2007.00002.x
Bomfim RA, Watt RG, Tsakos G Does water fluoridation influence ethnic inequalities in caries in Brazilian children and adolescents?. Community Dent Oral Epidemiol. 2022; 50:321-332 https://doi.org/10.1111/cdoe.12676
Whelton HP, Ketley CE, McSweeney F, O'Mullane DM. A review of fluorosis in the European Union: prevalence, risk factors and aesthetic issues. Community Dent Oral Epidemiol. 2004; 32:9-18 https://doi.org/10.1111/j.1600-0528.2004.00134.x
Pretty IA, Boothman N, Morris J Prevalence and severity of dental fluorosis in four English cities. Community Dent Health. 2016; 33:292-296 https://doi.org/10.1922/CDH_3930Pretty05
Health effects of water fluoridation: a review of scientific evidence. 2014. hdl.handle.net/10182/13121 (accessed June 2023)
Chankanka O, Levy SM, Warren JJ, Chalmers JM. A literature review of aesthetic perceptions of dental fluorosis and relationships with psychosocial aspects/oral health-related quality of life. Community Dent Oral Epidemiol. 2010; 38:97-109 https://doi.org/10.1111/j.1600-0528.2009.00507.x
National Academies of Sciences, Engineering, and Medicine. Review of the Draft NTP Monograph: Systematic Review of Fluoride Exposure and Neurodevelopmental and Cognitive Health Effects. 2020. www.ncbi.nlm.nih.gov/books/NBK555056/ (accessed June 2023)
Newton JN, Young N, Verne J, Morris J. Water fluoridation and hypothyroidism: results of this study need much more cautious interpretation. J Epidemiol Community Health. 2015; 69:617-618 https://doi.org/10.1136/jech-2015-205917
Drummond M, Sculpher MJ, Claxton K: Oxford University Press; 2015
Taylor GD, Carr K, Rogers HJ, Vernazza CR. A systematic review of the quality and scope of decision modelling studies in child oral health research. BMC Oral Health. 2021; 21 https://doi.org/10.1186/s12903-021-01680-3
Ternent L, Homer T, Shen J, Vernazza CR. Measuring cost in oral health care. In: Zaror C, Mariño R (eds). Cham, Switzerland: Springer International Publishing; 2022
Dixon S, Shackley P. Estimating the benefits of community water fluoridation using the willingness-to-pay technique: results of a pilot study. Community Dent Oral Epidemiol. 1999; 27:124-129 https://doi.org/10.1111/j.1600-0528.1999.tb02001.x
Tonmukayakul U, Calache H, Clark R Systematic review and quality appraisal of economic evaluation publications in dentistry. J Dent Res. 2015; 94:1348-1354 https://doi.org/10.1177/0022034515589958
Lowery G, Flinders M, Gibson BJ. When evidence alone is not enough: the problem, policy and politics of water fluoridation in England. Evid Policy. 2021; 17:507-523
Community water fluoridation and the benefits for children James A Atkinson Joshua M Jackson Gary Lowery Greig D Taylor Helen J Rogers Christopher R Vernazza Dental Update 2025 50:7, 565-569.
Authors
James AAtkinson
BDS, MFDS RCPS(Glasg)
Dental Core Trainee, County Durham and Darlington Foundation Trust
Academic Clinical Fellow in Paediatric Dentistry, Unit of Oral Health and Development, School of Clinical Dentistry, University of Sheffield, Claremont Crescent, Sheffield, S10 2TA, UK.
Dental caries prevalence in children is high and inequalities are significant, with a major burden for children, families and the health system. Community water fluoridation (CWF) has been shown to be effective and it may reduce inequalities. Despite concerns, there is no evidence that CWF has any major side effects. CWF can cause mild fluorosis of the teeth, but this can be associated with an improvement in quality of life. Economic evaluations of CWF have consistently shown that CWF is cost-saving. Despite the positive evidence, implementation is limited in the UK, and this appears to be due an inconducive political environment, although this is improving.
CPD/Clinical Relevance: Dental professionals should be aware of the benefits of CWF in order to be able to effectively advocate for its implementation.
Article
Dental caries in children remains a significant public health problem. Community water fluoridation has long been advocated as part of the solution to this problem and yet, implementation remains limited. This article explores the problem of caries in children and the evidence base for CWF (effectiveness, safety and cost-effectiveness). Finally, the reason for the lack of implementation is explored through the lens of policy analysis.
Caries in children: epidemiology and impact
Dental caries is a global epidemic, with the recent World Health Organization Global Oral Health Status Report estimating that 514 million children globally experience caries of the primary dentition.1 Across England in 2021–2022, there were 42,180 NHS hospital dental extraction episodes involving patients under the age of 19, with 63% of these having dental decay as the primary diagnosis.2 In 2020, 10.7% of 3-year-old children and in 2019, 23.4% of 5 year olds in England had experience of dental decay.3,4
Caries does not affect groups of children with equal prevalence. Of the 3-year-old children with decay experience recorded in 2020, significant regional variation exists. For example, in England, 6.7% of children in the East of England had caries experience compared to 14.7% in Yorkshire and The Humber.3,4 Alongside regional geographic variations, significant dental inequalities also exist between different ethnicities and by deprivation score.3,4 Of 5-year-old children in England with decay, significantly higher decay rates were found in the ‘Other Ethnic Groups’ (44.3%) and ‘Asian/Asian British groups’ (36.9%) compared to the England average decay rate of 23.4%.3 Toothache was reported by 25% of 12 year olds eligible for free school meals in 2020 compared to 16% of children not eligible for them.3 In the year 2021–2022, the caries-related tooth extraction rate for children in England's most deprived communities was around 3.5 times that of those in the most affluent communities.2
The impacts of dental decay on children are known to be significant, and include pain, distress, sleepless nights, struggling to eat, loss of teeth, missed school days, reduced school performance and hospital admission.5,6,7 In England, tooth decay is the most common cause of hospital admission among children of ages 6–10 years.2 The implications for the family of a child with tooth decay can include sleepless nights, days missed from work and increased stress.8
While the immediate impacts of decay are known to be upsetting to children, treatments can also provide challenges. General anaesthetic provision for dental extractions can cause children anxiety, distress, post-operative pain and difficulty eating afterwards.9 In addition, premature loss of primary teeth in children is known to negatively impact oral health-related quality of life.10
Extraction of carious teeth in under 19 year olds cost the NHS an estimated £50.9m in the financial year 2021–2022.2 This is an increase on the previous year; however, this increase is likely to have been related to service recovery following COVID-19. Hospital admissions for preventable disease not only cause a greater burden on national service provision, but present psychological impacts resulting in greater anxiety, with state anxiety shown to be higher in hospitalized children in comparison to non-hospitalized children.11 As primary, secondary and tertiary dental services aim to return their output to pre-COVID levels, it is likely that children will be faced with longer waiting times, and present to clinicians with increased levels of caries.2,12
The efficacy of community water fluoridation
Given the significant burden of dental decay in children, prevention of the disease is important. Several evidence-based interventions exist operating at different levels from upstream regulatory and community-based interventions to individual chairside or self-administered options. This article focuses on the public health intervention of community water fluoridation.
The efficacy of community water fluoridation (CWF) has been the subject of multiple systematic reviews. A reduction of 35% in the number of decayed, missing or filled (dmft) primary teeth has been reported as a result of the introduction of CWF.13 Similarly, a reduction of 26% in DMFT of permanent teeth has been suggested.13 There was an increase of 15% in the percentage of caries-free children, although there was little evidence to suggest that water fluoridation results in a change in caries levels among groups with different socio-economic status.13 Similarly, an earlier systematic review concluded that water fluoridation was associated with an increased proportion of children without dental caries, although the authors highlighted that the quality of studies was low to moderate, with high risk of bias.14
More recently, a report by Public Health England showed that caries experience in 5 year olds was most prevalent (25%) in areas with the lowest water fluoride concentration, and least prevalent (20%) in areas with highest water fluoride concentration, demonstrating community water fluoridation can reduce the prevalence and severity of dental caries.15 The greatest benefit was evident in the most deprived areas. CWF has also been associated with a reduction in hospital admissions for dental extractions.15,16 The prevalence of caries experience among 5 year olds was significantly lower with increasing fluoride concentrations irrespective of deprivation levels, with a greater effect being seen in areas of greater deprivation.17 It is interesting to note that a new study of re-introduction of CWF in Cumbria, suggested a lower effect of CWF, although this has yet to be incorporated into any systematic reviews.18
When considering healthcare inequalities, water fluoridation is associated with a significant reduction in dental interventions in the most deprived populations,19 although caution must be applied when making inferences regarding an individual's levels of deprivation, which may vary greatly from person to person among a similar socio-economic group. One study observed greater inequalities in healthcare following the cessation of a community water fluoridation programme.20
Two further studies compared a group exposed to CWF and a non-CWF control group, concluding that CWF can reduce dental caries and healthcare inequalities.21,22 It has been suggested that CWF reduces the gap in dental caries experiences between different social classes when compared to alternative community-based strategies.23 While CWF has been associated with reduced inequalities in caries prevalence among different ethnic groups in more disadvantaged settings, it does not appear to be as effective within populations in more affluent areas.24 To the authors' knowledge, all studies examining the relationship between water fluoridation, inequalities and health outcomes are limited to observational data and insufficient to draw casual inferences.
Community water fluoridation provides the opportunity to indiscriminately deliver health benefits to a wide population, which may have the greatest impact upon those with barriers to accessing dental resources and those in groups with lower socio-economic status.
Safety and side effects
In recent years, there has been increasing opposition to CWF owing to a range of potential safety concerns. The only widely accepted risk associated with excessive fluoride consumption relates to enamel fluorosis.25 When a developing tooth germ is exposed to high levels of fluoride, the enamel mineralization is adversely affected, resulting in a well-mineralized enamel surface with a subsurface porosity, which manifests visually as an opacity.26 The development of enamel fluorosis is dependent on the dose, duration and timing of exposure, producing deeper porosities and surface breakdown when these factors are increased.26
At the levels of water fluoridation found within the UK, the presence of enamel fluorosis is predominantly of aesthetic, rather than functional concern, producing mild to moderate white opacities.27 Higher levels of fluoride can be found naturally in drinking water in other parts of the world, producing severe enamel fluorosis, characterized by brown discolouration and pitting.25 There is a substantial body of evidence to demonstrate that enamel fluorosis is also caused by consumption of fluoride from sources other than tap water, as shown by the growing prevalence of enamel fluorosis in areas without CWF.28 This can occur owing to inappropriate use of fluoridated dental products, such as swallowing toothpaste, or inappropriate prescribing/use of fluoride supplements.
A study of enamel fluorosis in four cities in England observed the prevalence to be higher among children in fluoridated Newcastle and Birmingham (61%), compared to non-fluoridated Liverpool and Manchester (37%).27 Nonetheless, it is important to acknowledge that enamel fluorosis is particularly difficult to assess, not least because of the use of different measurement indices across studies, and the potential for misdiagnosis with other conditions that produce enamel opacities.13,25 It is perhaps more useful to consider the impact of enamel fluorosis on an individual's oral health-related quality of life (OHRQoL).29 Interestingly, while the evidence suggests that severe fluorosis has a negative effect on OHRQoL, mild fluorosis does not appear to cause concern, and has even been associated with increased OHRQoL.29
Concerns have also been raised regarding the potential effects of incorporation of fluoride into bones, with claims that it has an adverse effect on bone strength and mineral density, increasing the risk of fracture and osteosarcoma. There is a strong body of evidence to demonstrate that CWF up to 1ppm does not produce these adverse effects.30 Furthermore, routine monitoring of potential adverse effects of fluoride in England has failed to identify any association between hip fractures and CWF.15 Moreover, fluoride is not classed as a carcinogen for humans at any level, and there is no evidence of an association between osteosarcoma and CWF.28
It has also been postulated that higher levels of fluoride exposure (over 1.5ppm in drinking water) may be associated with cognitive impairment in children, although there is no evidence that this occurs at lower levels of fluoride exposure (such as those found within the UK water supply), or in adults.31 A number of these studies failed to consider any other potential reasons for cognitive impairment.28 Similarly, suggested associations between CWF and hypothyroidism have been disregarded, owing to a lack of credible evidence.32
Economic aspects of CWF
Despite the clinical efficacy and safety of CWF, the costs of implementation must be offset against these benefits to consider adopting it is an efficient use of resources. Resources available for health services (e.g. national health services (NHS in the UK)) are scarce, that is, there will never be enough resources to be able to provide all the healthcare that is needed. Therefore, choices must be made to decide what interventions to provide to maximize the benefits to society. Economic evaluations can be conducted to support decision makers to allocate limited resources. An economic evaluation compares two or more alternative courses of action in terms of their inputs (costs) and outputs (benefits). They are often run in conjunction with a clinical trial, but if the differences in costs and/or benefits are likely to extend beyond the trial period, then a decision analytical model can be produced.33 More detailed information on economic evaluations in oral healthcare in children can be found in published literature.34,35
Economic evaluations, such as cost-effectiveness analysis (CEA) and cost-benefit analysis (CBA), are most common in oral health. Estimating the costs for these analyses will depend on the perspective of the analysis (e.g. a health service perspective will only include costs that fall on the health service). Estimating outputs differs across analyses. CEA measures outputs in natural units (e.g. the number of episodes of pain avoided), whereas CBA measures output in monetary terms (e.g. monetary valuation of health, and non-health benefits, such as the willingness to pay for that intervention). CEA reports an incremental cost-effectiveness ratio, that is how much extra cost is incurred to obtain an extra unit of that outcome (e.g. an episode of pain avoided). In contrast, CBA presents results as a simple sum (as both costs and benefits are in monetary terms) representing the net monetary benefit, or loss, or the ratio of benefits to costs.33
Considering CWF, costs that should be included in an economic evaluation would focus on capital and operational. Capital costs, primarily include initial equipment set-up and the expected costs for maintaining this over the expected lifespan,36 and have been estimated to range between £1.6 million and £2 million.37 Whereas operational costs of CWF would include administrative support costs, costs of fluoride added to the water etc,36 and are estimated to cost approximately £330,000 per annum.37 In addition, annual costs to receive water fluoridation, routine dental costs, such as the cost of a check up, as well as decremental costs, such the costs of receiving a filling, or an extraction, should be included in any evaluation into CWF. Of note, Public Health England reported that CWF would cost about £0.52 per person per annum served by those fluoridation schemes. However, the costs of CWF would not fall on customers through water charges. Rather, the entire costs are covered by local authorities in their public health role, but will in the future fall to the secretary of state for health and social care.38
In contrast, estimating the benefits of CWF is more challenging. Measurements of natural units, such as reduction in number of decayed teeth, or reduction in number of general anaesthetics can be ascertained through routine data sets, where available. In contrast, ascertaining benefits, such as societal willingness to pay (WTP), could be used given that CWF potentially has a wider benefit than just to the individuals with dental caries. However, at present WTP values for CWF are old and limited to a small sample.39
The most recent comprehensive systematic review of all dental economic evaluations reported that only a handful of studies assessed the value of water fluoridation, with most presenting their results as net savings, as derived from the difference between water fluoridation programme costs, and costs of treating of dental caries and productivity losses averted. However, none of these studies elicited societal willingness to pay.40 A specific scoping review studying economic evaluations of CWF did find that all 24 studies included showed that CWF was cost saving compared with no CWF, but judgements on whether it is more cost effective than other preventive measures will depend on societal values of whether the extra cost incurred by CWF is worth the extra benefits gained.41
Therefore, it could be argued that where dental caries remains a significant public health issue, implementing CWF as a method to reduce dental caries rates, and indeed subsequent treatment burden, may not only benefit patients, but indeed the wider economy in terms of the costs savings to society. As such, these cost-savings could be re-invested into other areas of NHS dentistry. However, well-designed economic evaluations are required to fully determine how cost-effective CWF is, and further valuations of the benefits are necessary to make judgements about whether it is worth implementing CWF over, or as well as, other measures.
Policy and politics
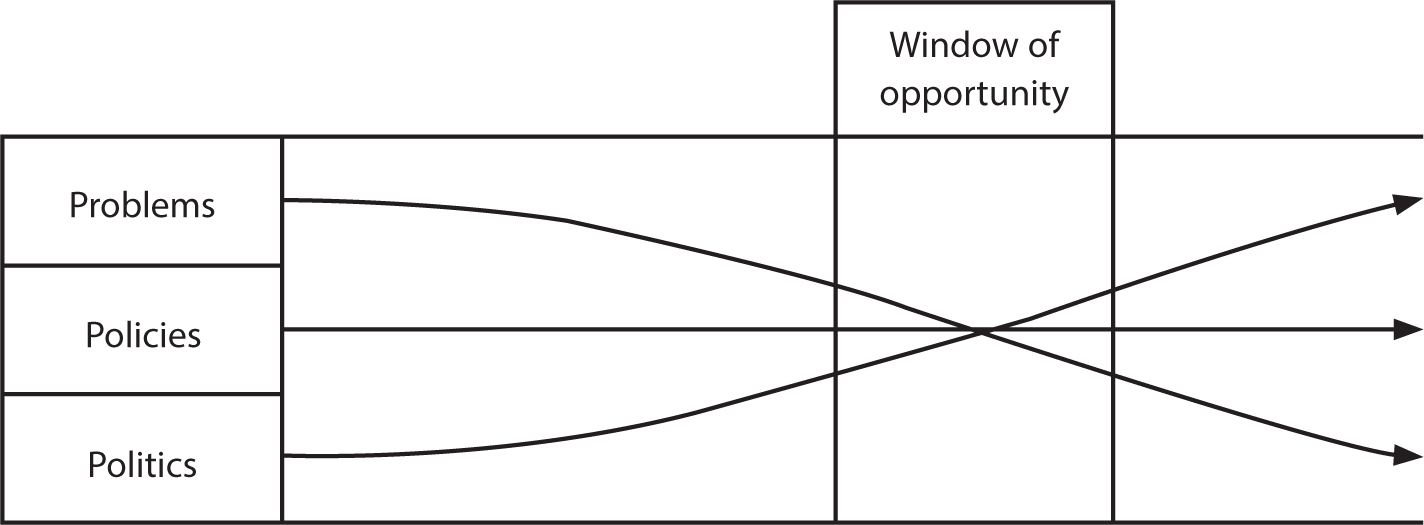
Despite the positive evidence for CWF, implementation in the UK remains limited. This can be explained by understanding the policy context of CWF. Attempts to understand water fluoridation policy in England are particularly well captured by the analytical insights provided by Kingdon's multi-streams approach (MSA).42 Put simply, the MSA suggests that policy implementation requires affirmative answers to three related questions (Figure 1):
Is there a widely recognized problem requiring government intervention?
(Does a credible policy solution exist?
Is the political environment conducive to supporting that policy?
Figure 1. Three streams combine to open a ‘window of opportunity’. Reproduced with kind permission from Lowery et al.43
If aligned, a ‘window of opportunity’ opens for policy change. With a clearly defined problem (paediatric dental health inequalities), and policy solution (water fluoridation) already articulated, it is to the politics stream that we turn presently.
Dental and academic community efforts to advocate for water fluoridation have, historically, been frustrated by government failure to follow the evidence and legislate for a policy that is highly effective and cost efficient. This reticence is attributable to the presence of a small, but vocal, opposition that ensures that water fluoridation is a controversial and risky political intervention. The result has been that successive governments have delegated decision making locally, with a legal requirement to consult the affected citizenry. The existence of similar incentive structures has nevertheless contributed to a prolonged period of policy paralysis with the political stream never fully aligning with the problem and policy streams.43
The COVID pandemic nevertheless created a rare window of opportunity for policy change. Political support was most evidently manifest in both the Health and Care Act (2022) and the Health and Care bill: water fluoridation policy paper which committed to ‘a population health approach, informed by the evidence’,44 with water fluoridation singled out as the “most effective public health measure there is for reducing oral health inequalities and tooth decay rates, especially among children”.44,45 The most significant policy commitment was to transfer responsibility for water fluoridation from local authorities and give the Secretary of State the power to directly introduce, vary or terminate water fluoridation schemes and assume responsibility for local consultations.45
Windows of opportunity can nevertheless close quickly without action being taken.42 Three current (in 2023 in the UK) considerations serve as a cautionary note in respect to water fluoridation. First, political change in the form of a quick succession of prime ministerial appointments has seen each incumbent eager to disassociate themselves from their predecessor's policies. Secondly, the COVID pandemic has been superseded by a cost-of-living crisis that has consumed political attention, thereby potentially displacing childhood tooth decay (and associated inequalities) from the Government's broader health agenda. This is evident in respect that, thirdly, numerous public health commitments have been delayed, scaled back, or cancelled. Arguably, the most prominent exemplar is delays to restrictions on multibuy deals and advertising foods high in fat, salt, and sugar in light of the ‘unprecedented global economic situation’.46 Risks, therefore, exist that childhood tooth decay becomes part of a more prosaic social challenge, with water fluoridation incorporated into the ‘primeval soup’ of multiple and competing policy initiatives, including targeted local interventions and emphasis on individual/parental responsibility. The dental profession has a key role to play in advocating that there is a problem and a viable policy solution, but the effectiveness of advocacy may be reduced if the political window is not optimal.
Conclusion
In summary, childhood caries remains a public health concern with significant prevalence, inequalities and service delivery problems leading to a significant quality of life and economic burden on children, families and the NHS. CWF is a safe, effective and cost-saving public health preventive approach with the potential to reduce inequalities, although quantification of the value of CWF is yet to be fully established. A current lack of implementation is related to the former lack of a conducive political environment. It appears that the political window is currently open but this could easily change.