Hervás-García A, Martínez-Lozano MA, Cabanes-Vila J Composite resins. A review of the materials and clinical indications. Med Oral Patol Oral Cir Bucal. 2006; 11:E215-220
Lee JH, Um CM, Lee IB. Rheological properties of resin composites according to variations in monomer and filler composition. Dent Mater. 2006; 22:515-526
Bagherian A, Shirazi AS. Flowable composite as fissure sealing material? A systematic review and meta-analysis. Br Dent J. 2018; 224:92-97
Erdemir U, Sancakli HS, Yaman BC Clinical comparison of a flowable composite and fissure sealant: a 24-month split-mouth, randomized, and controlled study. J Dent. 2014; 42:149-157
Beun S, Bailly C, Devaux J, Leloup G. Physical, mechanical and rheological characterization of resin-based pit and fissure sealants compared to flowable resin composites. Dent Mater. 2012; 28:349-359
Simonsen RJ. Preventive resin restorations and sealants in light of current evidence. Dent Clin North Am. 2005; 49:815-823
Savage B, McWhorter AG, Kerins CA, Seale SN. Preventive resin restorations: practice and billing patterns of pediatric dentists. Pediatr Dent. 2009; 31:210-215
Chuang SF, Jin YT, Liu JK Influence of flowable composite lining thickness on Class II composite restorations. Oper Dent. 2004; 29:301-308
Aggarwal V, Singla M, Yadav S, Yadav H. Effect of flowable composite liner and glass ionomer liner on class II gingival marginal adaptation of direct composite restorations with different bonding strategies. J Dent. 2014; 42:619-625
Baroudi K, Rodrigues JC. Flowable resin composites: a systematic review and clinical considerations. J Clin Diagn Res. 2015; 9:ZE18-24
Blum IR, Wilson NHF. Consequences of no more linings under composite restorations. Br Dent J. 2019; 226:749-752
Sadeghi M, Lynch CD. The effect of flowable materials on the microleakage of Class II composite restorations that extend apical to the cemento-enamel junction. Oper Dent. 2009; 34:306-311
Boruziniat A, Gharaee S, Sarraf Shirazi A Evaluation of the efficacy of flowable composite as lining material on microleakage of composite resin restorations: a systematic review and meta-analysis. Quintessence Int. 2016; 47:93-101 https://doi.org/10.3290/j.qi.a35260
Nguyen KV, Sathorn C, Wong RH, Burrow MF. Clinical performance of laminate and non-laminate resin composite restorations: a systematic review. Aust Dent J. 2015; 60:520-527
McCoy RB, Anderson MH, Lepe X, Johnson GH. Clinical success of class v composite resin restorations without mechanical retention. J Am Dent Assoc. 1998; 129:593-599
Cieplik F, Scholz KJ, Tabenski I Flowable composites for restoration of non-carious cervical lesions: results after five years. Dent Mater. 2017; 33:428-437
Geštakovski D. The injectable composite resin technique: minimally invasive reconstruction of esthetics and function. Clinical case report with 2-year follow-up. Quintessence Int. 2019; 50:712-719
Terry D, Powers J. A predictable resin composite injection technique, Part I. Dent Today. 2014; 33:96-101
Purayil T, Chakravarthy A, Ginjupalli K, Ballal N. Evaluation of bond strength of splinting materials to the teeth using three adhesive systems-an in vitro study. Saudi J Oral Sci. 2015; 2:94-98
Johari Y, Ariffin Z, Taib H, Mokhtar N. Minimum intervention dentistry with indirect fibre-reinforced composite bridge: a case report. Arch Oral Sci. 2016; 11:49-53
The versatility of flowable composites. Part 2: clinical uses Matheel AL-Rawas Yanti Johari Nazrul M Yusoff Dasmawati Mohamad Adam Husein Dental Update 2025 49:8, 633-636.
Authors
MatheelAL-Rawas
BDS, MResDent (Prosthodontics), FRACDS
Specialist and Clinical Lecturer, Prosthodontic Unit, School of Dental Sciences, Universiti Sains Malaysia; Hospital Universiti Sains Malaysia
BDSc, Grad DipClinDent, DClinDent, FRACDS, Senior Lecturer, Prosthodontics Unit, School of Dental Sciences, Universiti Sains Malaysia, Kelantan, Malaysia.
Flowable composite (FC) is a type of tooth-coloured restorative material with a lower viscosity compared to other types of resin composites. FC is considered as a versatile dental material, with a wide range of application. FCs have progressively gained importance in clinical dentistry. The increase in consumer demand has resulted in a gradual upsurge of dental professionals relying on composites in injectable form. Scientific and technological improvements in their properties and handling characteristics have not only seen FCs grow in popularity, but resulted in the development of different generations and types of dental FCs suitable for use in all cavity types, lining, core build-ups, and most recently, bulk-fill flowable composites.
CPD/Clinical Relevance: To provide clinicians with an overview of the indications and clinical applications of the conventional FCs.
Article
Most of the resin composites used today are of a putty-like consistency, which suits the needs of different dental applications. Nevertheless, as demand from clinicians has increased, the search has begun for a material that can offer easy handling and better adaptation into minimal and deep cavity preparations with difficult access. This led to the launch of flowable composite at the end of 1996.1 Low viscosity and better wettability allow the material to flow into every corner and surface without voids or gaps, in contrast to that of putty-like composites. Flowable composites may reduce chairside time and improve the quality of the restoration.2
Clinical indications for conventional flowable composite
Pit and fissure sealant
While most clinical studies have reported that flowable composites (FCs) have better clinical performance in comparison to other sealants,3 some have also added that they have better retention rates as well.4 The mechanical properties of multiple commercial FCs were measured and compared to four conventional sealants. They found that commercial FCs yielded superior results in the tested parameters in comparison to conventional sealant materials.5
Preventive resin restoration (PRR)
Given the difficulty of packing putty-like composites into small cavities, FCs are better as they not only flow, but also retain the benefits of both resin composites and sealants.6 A survey sent to paediatric dentists found that most clinicians favoured the use of FCs in preventive resin restorations.7 Considering the small dimensions of the cavities prepared for PRR as opposed to Class I cavities, the occlusal wear of conventional FC may be limited. Occlusal wear can vary among different materials because it depends on several factors, including size and volume of filler particles.
Cavity Liner
Flowable composite may be used as the first increment or liner for the restoration before filling the rest of the cavity with conventional composite. This step is crucial as the flowable composite can seal the margin and irregularities of the cut cavity surface.8,9 Furthermore, owing to its low viscosity, a flowable composite can function to properly wet the cavity surface.10 Although the study by Blum and Wilson recommended against placing linings under composite restorations,11 the authors of this review contend that FCs have the ability to seal irregularities and the cavity margins when applied as a first thin increment in the restoration process (Figures 1 and 2). Additionally, FCs do not limit the surface area for bonding, or limit material thickness, because flowable and packable types are made of the same material, resin composite. Sadeghi and Lynch showed that FCs were able to mitigate microleakage if applied as a first thin increment.12 However, in two systematic reviews and meta-analyses,13,14 restorations in which FCs had been used as an intermediate layer did not improve the clinical performance. As a result, the use of flowable composites as a lining material remains debatable.11
Figure 1. Carious cervical lesion on the cervical area of mandibular left first molar (LL6).Figure 2. Restoration was made with conventional flowable composite (Filtek Z350Xt, 3M ESPE) as a liner capped with packable composite after usage of retraction cord and cervical matrix.
Class V non-carious cervical lesions
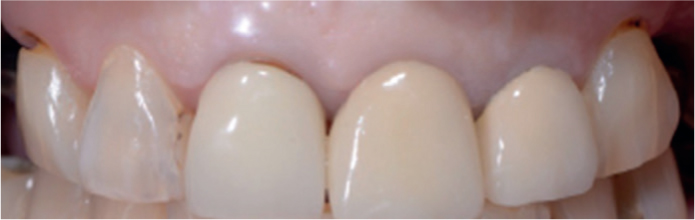
When a tooth is flexed during mastication, the concentration of chewing forces in the cervical region may cause chipping and microfractures. Restorative materials with rigidity and a high modulus of elasticity have a reduced ability to withstand tooth flexure in the cervical region.15 FCs are characterized as materials with a low modulus of elasticity, which is similar to that of a tooth structure. Figures 3–6 demonstrate the restoration of non-carious cervical lesions (NCCLs) with FC.
Figure 3. Non-carious cervical lesions (NCCLs) affecting the cervical parts of maxillary right and left canines (UR3 and UL3).Figure 4. Restoration of NCCLs with conventional flowable composite after usage of retraction cord and a cervical matrix.Figure 5. NCCL affecting the cervical part of mandibular right first premolar (LR4) due to hard bristle toothbrush use.Figure 6. Photograph was taken immediately after restoration of NCCL in Figure 5 by using conventional flowable composite after proper isolation.
A study evaluated the use of two types of FCs to treat 50 patients presenting with Class V abfraction lesions and reported good performance over a period of 5 years, with retention rates of 94.7% and 84.2%.16
Minimally invasive composite veneers by an injection moulding technique
This is an indirect/direct technique using a diagnostic wax-up and silicone key to inject high strength FC, such as G-aenial Universal Flo (GC, Leuven, Belgium), over teeth. With little to no preparation required, it can be used for definitive or transitional restorations, and to restore fractured or worn dentition. The use of these improved-formula conventional FCs in this technique is not only minimally invasive, but inexpensive in comparison to ceramic veneers.17,18
Other indications
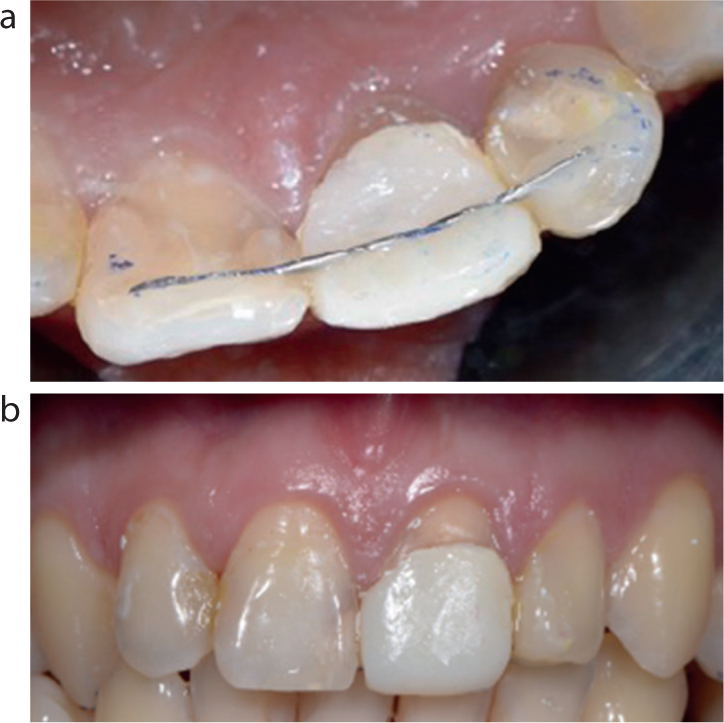
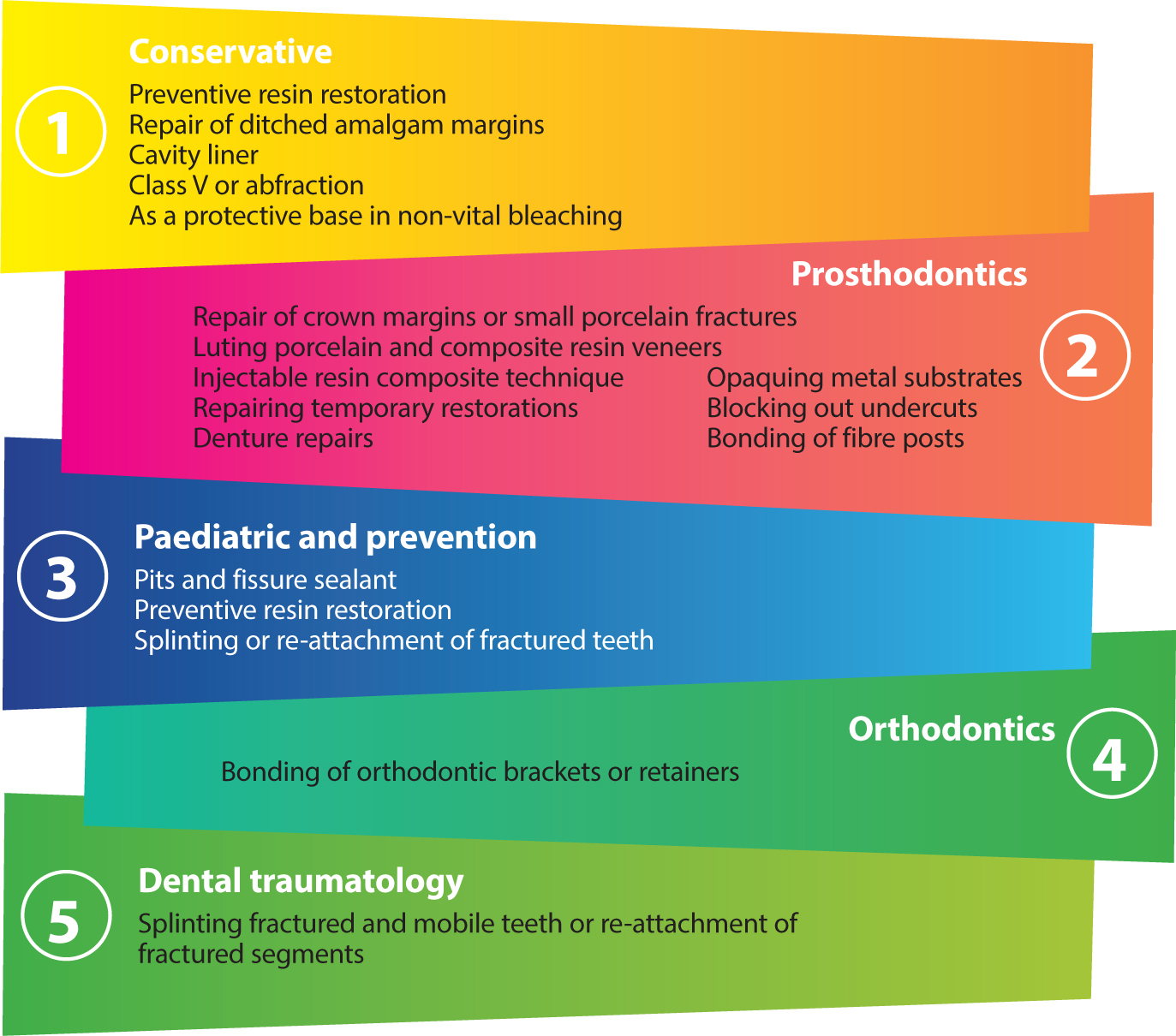
In order to splint a fractured tooth, FCs can be used to attach orthodontic wire or ribbon to the tooth structure. Figures 7 and 8 show the splinting of a temporary crown after an incident of a fractured crown of root canal-treated tooth. In orthodontics, FCs are used to bond braces or brackets to teeth.19 An FC was successfully used in a recent case report to cement a fibre-reinforced composite cantilever bridge.20Figure 9 summarizes all the indications mentioned above, as well as other uses mentioned by Baroudi and Rodrigues.8
Figure 7. The patient presented to the clinic with a fractured root canal-treated maxillary left central incisor (UL1) at the end of a working day and the next 3 days were holidays. The patient wanted a temporary solution to close the gap and restore his smile.Figure 8. Fixation of the temporary crown, splinted with adjacent teeth by using orthodontic stainless-steel wire and conventional flowable composite (Filtek Z350Xt, 3M ESPE) (a) Occlusal view. (b) Frontal view.Figure 9. Summary of the indications for the use of conventional flowable composite.
Conclusion
Different clinical situations demand specific materials to produce the desired results. Versatile materials, such as flowable composites with their various types, can offer easy application and distinctive qualities. Conventional FCs can have different ratios of fillers and range of viscosities. High flow FCs can be used for a wide range of applications, such as lining a contained cavity. On the other hand, medium-to low-flow highly filled FCs that are stackable and sculptable, can be used for restoring classes I–V and composite veneers. A few other types of flowable composites are worth mentioning, such as self-adhering FCs, bioactive FCs and bulk-fill FCs. Self-adhering FCs can save time, especially in children and anxious patients; however, their performance need further investigation before being recommended at this stage. Bioactive FCs with their ion-release features can repair or help in tooth tissue regeneration, especially in deep cavities or where there is a need for further protection against cariogenic bacteria. Finally, Bulk-fill FCs can offer high-quality restoration and can save valuable time for the patient and clinician with single-increment restorations. As with all dental materials available in the market, each material has its benefits and limitations that affect its overall longevity. Dental practitioners should, therefore, choose suitable materials for each clinical case based on the best evidence currently available.