Moy PK, Iacono VJ. Impact of biological and technological advances on implant dentistry. Int J Oral Maxillofac Implants. 2011; 26:7-10
Lund JP. Introduction: It is time to tackle denture disability. In: Feine JS, Carlsson GE (eds). Carol Stream, IL: Quintessence; 2003
Walls AW, Steele JG. Geriatric oral health issues in the United Kingdom. Int Dent J. 2001; 51:(3)183-187
Mojon P, Thomason JM, Walls AW. The impact of falling rates of edentulism. Int J Prosthodont. 2004; 17:(4)434-440
Implementation of Directive 2007/47/EC for Active Implantable Materials.Brussels: Cosmetic and Medical Devices Directive;
Wood MR, Vermilyea SG. A review of selected dental literature on evidence-based treatment planning for dental implants: report of the Committee on Research in Fixed Prosthodontics of the Academy of Fixed Prosthodontics. J Prosthet Dent. 2004; 92:(5)447-462
Malo P, de Araújo Nobre M, Lopes A, Moss SM, Molina GJ. A longitudinal study of the survival of All-on-4 implants in the mandible with up to 10 years of follow-up. J Am Dent Assoc. 2011; 142:(3)310-320
Anitua E, Orive G. Short implants in maxillae and mandibles: a retrospective study with 1 to 8 years of follow-up. J Periodontol. 2010; 81:(6)819-826
Hobkirk JA, Abdel-Latif HH, Howlett J, Welfare R, Moles DR. Prosthetic treatment time and satisfaction of edentulous patients treated with conventional or implant-supported complete mandibular dentures: a case-control. Int J Prosthodont. 2008; 21:(6)489-495
J Prosthet Dent. 1998; 79:(1)2-108
Thomason JM Two implant retained overdentures – a review of the literature supporting the McGill and York consensus statements. J Dentistry. 2011; https://doi.org/10.1016/j.jdent2011.08.017
Mackie A, Lyons K, Thomson WM, Payne AG. Mandibular two-implant overdentures: three-year prosthodontic maintenance using the locator attachment system. Int J Prosthodont. 2011; 24:(4)328-331
Radiation Protection: Cone Beam CT for Dental and Maxillofacial Radiology. 2011. www.sedentexct.eu
Dawson ALondon: Quintessence; 2009
Esposito M Interventions for replacing missing teeth: augmentation procedures of the maxillary sinus.
The loss of all teeth from one or both dental arches is a significant disability affecting self-confidence, communication, masticatory function and aesthetics. Whilst missing teeth cannot be restored to the natural state, the development of a prosthetic dentition has been a goal of dental science throughout the centuries. Contemporary techniques allow for the replacement of missing dentition with fixed or removable solutions, solving many of the problems. Implant dentistry has transformed this area of medicine. This article provides dental practitioners with an overview of this important area of patient care.
Clinical Relevance: Dental practitioners in clinical practice will frequently see edentulism; a good understanding of the available options for rehabilitation is essential.
Article
The aim of this article is to provide the busy practitioner with a clear overview of contemporary implant-retained solutions to edentulism, with the emphasis being on the techniques supported by good clinical results over a clinically appropriate term. Prominence is given to techniques most suited to a general dental practitioner with some experience of implant dentistry.
Elsewhere within this issue of Dental Update there is information regarding pretreatment assessment, treatment planning and replacement of missing teeth with implant-retained solutions (pp128–134). This article will assume that prior knowledge and only information specific to full-arch restorations will be discussed.
There is no doubt that dental implants have had a major influence on the restorative options in restorative dentistry. The reliability of contemporary implant dentistry is challenging our perception of restorative dentistry in the wider sense, with the pressure of assessing prognoses for heavily restored teeth as compared to the reliable provision of an osseointegrated replacement. The particular challenges of edentulism have, through the ages, provided the profession with a significant challenge. A significant improvement in quality of life has been provided with the osseointegrated solution.1 The benefits of osseointegration are unlikely to be available to all, hence the need to continue to manage edentulism conventionally, with dental implants offering an improvement upon edentulism, but not a replacement for the natural dentition.
Edentulism is a disabling condition where ‘people with no teeth are considered physically impaired’. Edentulous patients could also be considered disabled, due to their inability to eat and speak effectively, which are two of the essential tasks of life; they could be considered handicapped, as they tend to avoid eating and speaking in public.2
The prevalence of edentulism has been estimated as falling to 4% of the UK population.3 There have been numerous studies detailing the rates of edentulism; some of these have identified confounding factors.
Finland, Sweden and the United Kingdom are the only three European countries with reliable epidemiological data allowing for data projection over the next two decades.4 Their data predict a 50–60% reduction in edentulism over the next 20 years. It is this type of change that has already shaped provision of full denture prosthetic training in dental schools throughout Europe. Whilst implant-retained prosthetics can offer much to an edentulous individual, there are significant economic, individual and anatomic limits to their provision.
The demographic group where edentulism is most prevalent will be an ever increasing age group, which will potentially increase the surgical complexity and management of such cases. Therefore, a good understanding and practical ability with conventional prosthetic techniques will continue to be required, and such skills needed, for potentially more challenging cases.
Interpretation of epidemiological data should consider that many individuals are edentulous in only one jaw; the resultant management of an edentulous jaw functioning against a dentate jaw posing additional problems, but the data are not easily recovered from statistics on edentulism. One factor that is clear is that patients losing their teeth now are better informed and expect more from any replacement, be that conventional or implant-retained. This factor may in part explain the increase in litigation, with implant dentistry rapidly catching conventional prosthetics as the most frequent area for legal action.
When considering the provision of dental implants the practitioner has a legal and ethical responsibility to choose a medical device which has a sufficient outcome assessment based on published data5 and provide treatment which falls within his/her level of competence and training.
Goals of treatment
One of the chief goals of treatment is the improvement of social, psychological and functional parameters by the modification or replacement of removable dentures with dental implants to stabilize or support a prosthesis (fixed or removable).
The management of failing crown and bridgework has been covered earlier in this issue of Dental Update (pp78–84); this paper will focus on dental implant options for the edentulous patient, with brief consideration given to those with a terminal dentition as they contemplate the transition to edentulism.
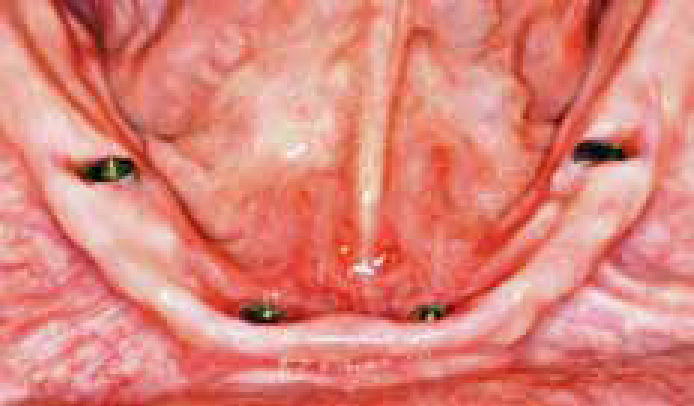
Initially, implant-supported prostheses were only indicated for the edentulous mandible: 4–6 implants placed inter-foraminally to support a prosthesis. With sufficient antero-posterior spread of implants, a fixed solution is possible; generally a distal cantilever of 10–12 mm will support sufficient occlusion (Figures 1–4). If this is not possible, an implant-retained overdenture should be provided.6
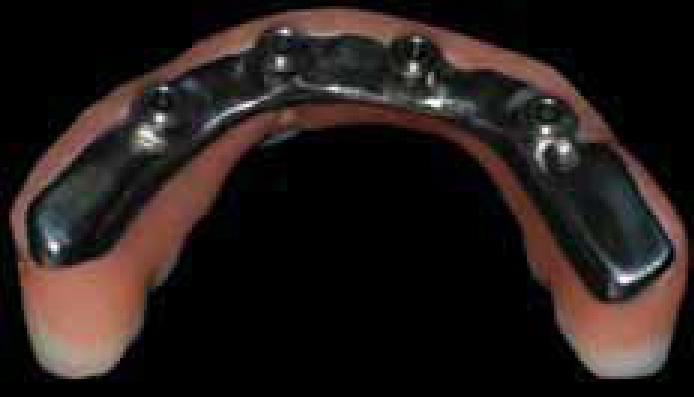
Figure 1. Four implants in the mandible with good distribution.Figure 2. NobelProcera™ Implant Bridge custom-milled titanium bridge framework.Figure 3. NobelProcera™ definitive bridge from mucosal aspect.Figure 4. Aesthetics can be very acceptable with fixed implant prosthetics.
Treatment planning
The number of implants required depends upon the proposed restoration and the implant dimensions, amongs other factors. There has been a tradition of providing fixed full-arch restorations using porcelain fused to metal (PFM) construction. Owing to thermal contraction of the substructure (often gold) in the casting process, technical limitations are imposed on framework length. This can be addressed by using short lengths of fixed bridgework, or sectioning the framework and soldering.
In the first scenario, fixed arch prosthetics in the maxilla are frequently provided by four PFM bridges, with implant support at each end of a 3-unit bridge. This approach requires 8 implants and supports 12 prosthetic ‘teeth’.
The alternative of a one-piece cast metal framework, supporting all the teeth, has technical issues as thermal contraction creates dimensional inaccuracy. The framework will be sectioned between the implants and soldered; the greater the number of implants the more soldered joints will be required, which is technically challenging. It is normal for such a construction to be supported by 6–8 implants. In the mandible 4–6 implants are usually considered sufficient for this type of reconstruction, the difference in number of implants being attributable to implant distribution and bone volume/density.
More recent advances in CAD/CAM (computer-aided design/computer-assisted milling) technology have enabled construction of milled titanium frameworks (Figure 2). This technology allows reductive machining at room temperature from a solid block of material, allowing significant improvement of accuracy by avoiding any thermal dimensional changes, as found in traditionally cast frameworks. This has primarily been utilized to form titanium frameworks, but the technology also enables ceramic materials such as zirconia to be used. The use of ceramics as a full-arch superstructure support is designed to provide an improvement over traditional metal frameworks by eliminating the aesthetic challenge of a dark and opaque framework, and offering a potentially greater degree of biocompatibility. The use of full-arch ceramic frameworks is in its infancy and currently lacks long-term data. The CAD/CAM titanium framework has been highly successful, with titanium being well tolerated by the mucosa, cost-effective, readily available and easily milled. Typically, the titanium framework is used to support traditional acrylic prosthetic teeth in a simple pink acrylic veneer. This offers many advantages over porcelain, in terms of cost, reparability, and dimensional change (fabricated without firing ceramics) (Figure 3).
The aesthetics available with good quality acrylic denture teeth can be excellent, and allow for characterization and individualization similar to porcelain, but at a reduced cost (Figure 4). Paulo Malo's 10-year data support this approach, with 93.8% implant success at 10 years and few prosthetic complications, when immediately loaded in the mandible.7 There have been many modifications of this theme, including using the titanium framework to support individual all ceramic crowns, where the framework is veneered with pink composite ‘gingivae’.8
Generally, there is a lack of long-term data regarding the use of short implants (<8.5 mm) in the maxilla. There are plenty of case reports, but a lack of randomized controlled studies. There does seem to be an increasing tendency to use short implants as an alternative to a more invasive bone augmentation technique, with some promising implant survival rates in the hands of experienced users.9
Edentulous at presentation
For this group of patients, denture problems relate to non-adaptation to conventional prosthetic solutions. The overwhelming majority of studies describe complaints relating to mandibular prostheses.10
These functional problems relate primarily to lack of stability and retention with conventional dentures influenced by:
Border extension;
Accuracy of fit;
Adequate ridge morphology;
Suitable contour of polished surface;
Tooth position;
Occlusion;
Adaptive capacity.
The addition of dental implants will usually have a significant positive impact on the functional problems relating to complete dentures. Management of the above principles does not guarantee a satisfactory outcome, however, they should be considered important parameters regardless of the means of additional retention, which can be:
Implant-supported prosthesis (implant borne and retained).
Mandibular implant-retained overdenture (MIRO)
For many years the MIRO has been accepted as the standard of care for the edentulous mandible.11,12 There are a number of MIRO configurations which relate to the number of implants used and their connection system. Typically, two implants are provided inter-foraminally to support a MIRO. Some authors have suggested four implants be used to provide additional stability, though there is little evidence to support this; additionally, four implants would allow for a fixed configuration if loading and distribution are appropriate.
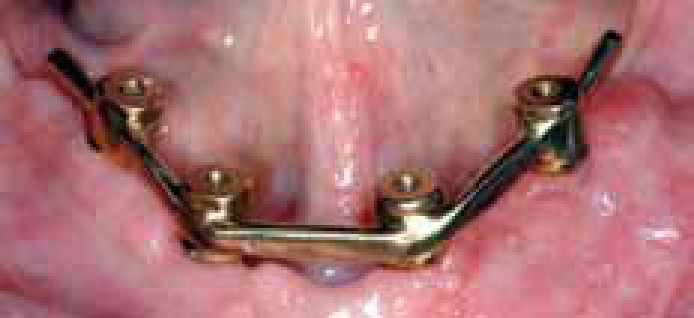
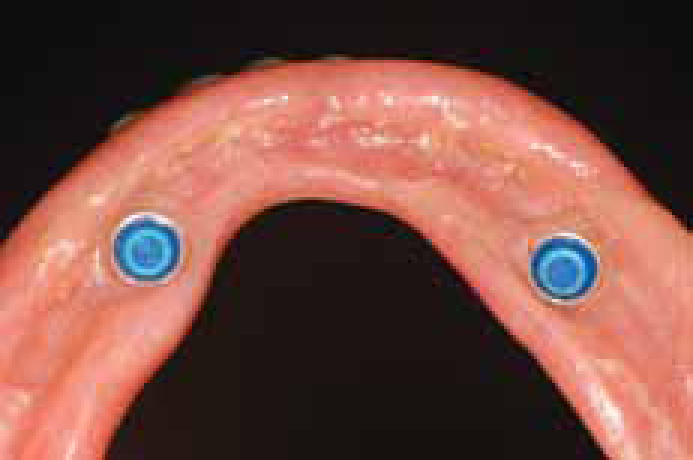
Figure 5. Gold bar supported by four implants.Figure 6. Two Locator abutments for overdenture retention.Figure 7. Locator housings in readiness for connection to prosthesis.Figure 8. Locator housing secured in prosthesis, fitted with light retention inserts (blue).
Distribution of dental implants in the anterior mandible will be limited by anatomy (Figure 1). Ideal positioning of implants allows for:
Maximizing antero-posterior distance for stability and reduced cantilever of the prosthesis;
Avoidance of exit of mental nerve;
Maintenance of prosthetic options;
Angulation of the implants allowing retentive elements to be within prosthetic envelope.
Fixed dental prosthesis
There is no doubt that a fixed solution is frequently perceived by a patient as a better replacement for missing teeth; certainly there is a strong emotional and psychological demand for a fixed solution. The reality may provide a significant, even insurmountable, aesthetic challenge (particularly in the maxilla) and a removable solution offers a readily cleanable solution, which is a real advantage in terms of personal hygiene and longevity of both restoration and, more importantly, the implants.
With four or more well distributed implants per arch, treatment options include an implant-supported prosthesis. Historically, these prostheses were fabricated with a gold framework veneered with porcelain in a similar construction to a conventional PFM bridge. The prosthesis would be screwed to the implants directly, which means that, if the implant was labially orientated, a small screw hole would become visible on the labial surface. Abutments connected to the implants, referred to as angled abutments, provide a relatively small angle change, usually between 10 and 30 degrees, to optimize the screw access. A small prosthetic screw is used to retain the prosthesis.
Additional components, such as these angled abutments, come at a price, both in financial terms and technical implications. The use of angled abutments in the maxilla is commonplace. The angled abutment incorporates an extra level into the construction, which increases complexity, and may demand an additional impression, further introducing potential for errors. The added abutment level has a space requirement, in a situation where space is usually very limited. Any additional component has the potential for failure, so the more screws there are, and the more components, the more likely are prosthetic complications such as screw fracture and abutment loosening.
In the mandible, the screw access is more likely to be lingual of the incisal edge, allowing a straight connection. Frequently, this would not require an abutment, allowing construction of the definitive restoration to be screwed directly to the implant.
Aesthetics
With the MIRO restoration aesthetics are relatively straightforward, the location of the implants having little impact on the position of the replacement teeth and gingival tissues. The removable solution for the maxilla places greater emphasis on implant position, as space is crucial. The size of the retentive elements is less easy to fit within the prosthetic envelope, resulting in unacceptable bulk and even causing difficult aesthetic issues.
When considering a fixed solution, aesthetic demands on decision-making can be a real challenge, with the most problematic situation identifiable by revealing the gingival tissue on smiling. An essential step in treatment planning and consent is the try-in stage prior to implant placement. This can be undertaken with a conventional wax try-in, the amount of labial flange a good indicator of aesthetic difficulty. This allows the patient to be informed of the potential aesthetic risk of visibility of the prosthetic margin on smiling. This can often only be overcome prosthetically by the use of a removable solution; yet, if there is sufficient bone, the alveolar crest can be surgically repositioned apically to avoid this problem. Therefore, the patient needs to be aware of these requirements before embarking on such treatment, and it would be prudent in these marginal cases to advise a patient that the outcome cannot be predicted 100%.
For some patients, the idea that dental implants can provide ‘screw-in teeth’ germinates in the mind as a replacement for lost teeth that is indistinguishable from the natural dentition. Management of patient expectation is crucial in this regard.
Implant placement
Following discussion of the treatment plan, patient consent must be gained. Patients must be informed of potential benefits and success rates, as well as possible risks, and be made aware of alternatives. Fixed full-arch prostheses are complex to plan, deliver and maintain14 and patients need to be aware of their responsibilities regarding maintaining these restorations and the practitioner confident about patient compliance. A plan of treatment can then be arranged. This would usually require a number of laboratory items, in particular a surgical stent, which is used during surgery to guide the location and orientation of the proposed implants. Implant dentistry is a restorative discipline with a significant surgical element. However, the responsibility must be to ensure that implant placement is driven by the proposed restorative solution.
The use of CT scans to provide information on bone dimension has evolved to enable computer-aided planning and the subsequent fabrication of accurate surgical stents fabricated from the CT data. Figures 9 to 11 have been produced using NobelGuideTM software (Nobel Biocare). Though not essential, a CT scan, or more often a cone beam CT (CBCT) scan, will provide information guiding the angulation, dimension, depth and location of proposed implant sites. With reduction in effective radiation dosage due to restriction of scan volumes and increased detector sensitivity, the use of contemporary highly accurate CBCT will no doubt increase and probably become the norm for treatment planning of the edentulous patient.15
Figure 9. CBCT scan allowing prosthetically driven treatment planning.Figure 10. CBCT technology enables implant positioning from restorative aspect.Figure 11. NobelGuide™ surgical guide for accurate implant placement.
Implants are placed surgically under aseptic protocols, usually under local anaesthesia with or without IV sedation. The surgery for placement of two implants inter-foraminally in the mandible is reasonably straightforward. Particular risks are altered sensation to the lip and chin, and bleeding (which may be significant), as well as the usual surgical risks. In the maxilla, a full-arch reconstruction involving six or more implants may carry no greater surgical risk, though specific attention needs to be placed on the anatomical limits posed by nasal and maxillary sinuses (Figure 12).
A protocol of loading a full-arch on four implants, known as ‘All-on-4’, has been proposed to simplify surgery and reduce costs, risks and treatment times for edentulous patients by utilizing the bone between the sinuses in the maxilla, and intra-foraminally in the mandible to install four implants. In the maxilla, the distal implants are angled to avoid perforation of the maxillary sinus and decrease the length of any prosthetic cantilever. Sinus augmentation, first described by Boyne and James in 1981, has become an established procedure to enable placement of implants in the posterior maxilla, where pneumatization of the sinus would otherwise preclude the placement of dental implants,16 though contemporary techniques attempt to reduce the incidence of this procedure.
Loading protocols
The most reliable technique is to allow undisturbed healing during osseointegration; this is known as delayed healing. This time period varies according to systemic factors, local bone conditions, implant surgery and implant parameters, amongst other features, but is typically 3–6 months.
The alternatives are:
Immediate loading: where implants are placed and loaded in function the same day (Figure 14);
Early loading: where implant prosthesis is placed from 48 hours up to 3 months following implant placement.
Figure 14. Immediately placed implants after healing.
Restoration
Overdentures
Healing abutments are replaced with precision attachments. These are torqued down firmly to the implants as per manufacturer's recommendations. Transfer impression copings (Figure 13) are connected and a suitable impression material (addition cured silicone or poly-ether) used to pick up these components in a special tray. The technician is then able to process the definitive overdenture with the components in place. Chairside adjustment is often a simple case of choosing the appropriate insert (recommended to start with the lowest value) and providing instruction to the patient on insertion/removal and maintenance.
Figure 13. Transfer copings for Locator system.
Fixed full-arch
The treatment planning provides a template for the definitive restoration. In the more complex cases, this needs to be reviewed following exposure of the implants (second stage surgery). To restore the implants, the practitioner needs to take an impression. This may often be of the implant ‘head’ and is known as a fixture level or implant head impression (Figure 15). This case shows six implants in the maxilla, the distal two have angled abutments fitted. This allows a model to be fabricated with replicas of the implants embedded in the model in the implant positions.
Figure 15. Immediately loaded implants with provisional bridge, see Figure 14.
Impression-taking
Impression ‘transfer’ copings are carefully attached to the implants; confirmation of accurate seating may be undertaken with radiographs. An ‘open tray’ impression would typically be used, where a special tray has openings to allow the tray to sit over the copings in the mouth, and protrude slightly. The hole is occluded with wax, and the impression taken, ensuring that the impression copings protrude through the wax (Figures 16–18).
Figure 16. Fixture or implant level impression copings in position.Figure 17. Special tray, open design, with openings for impression copings.Figure 18. Impression guide pins protrude through wax.
The impression is removed from the mouth by unscrewing the copings and withdrawing impressions and copings together. The technician attaches a ‘replica’ of the implant to the coping and creates an accurate model. The same technique is applicable to implant or abutment level impression with the appropriate abutment or implant level impression coping.
A silicone index (Figure 19), made from the diagnostic try-in, allows the clinician to choose appropriate abutments as necessary to alter the screw angulation, or modify the depth of the prosthetic level. If abutments are required these are placed clinically, torqued to the correct tightness (manufacturer's recommendations) and another impression taken, this time of the abutments. In cases where a CAD/CAM framework is constructed, an acrylic jig is made on the model, and tried in clinically. This ‘verification jig’ is used to confirm accuracy of the model and is used at either the implant or abutment level, as required. It may be necessary to section the jig and reconnect with cold-cured acrylic in the mouth, to ensure passive fit (Figures 20 and 21). With a PFM construction, the framework can be sectioned and reconnected in a similar manner. A new model is then fabricated and the framework either soldered conventionally or laser welded.
Figure 19. Silicone index (pink) and ‘scan ready’ acrylic replica of proposed framework.Figure 20. ‘Verification jig’.Figure 21. Close up of ‘verification jig’.
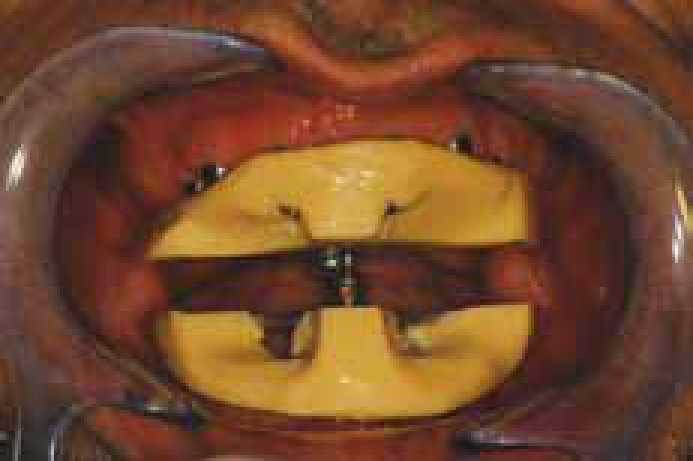
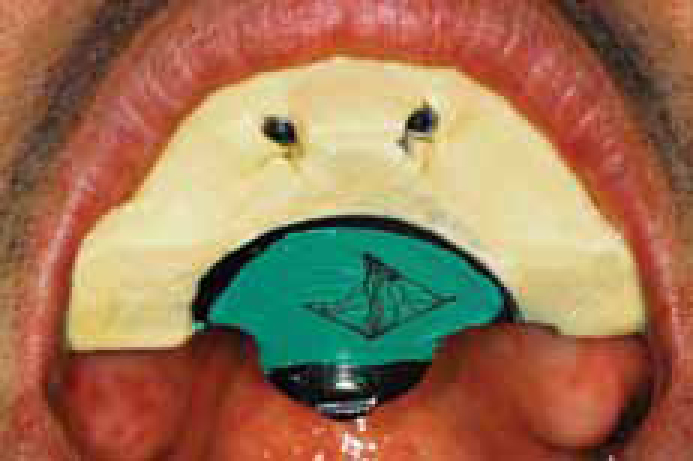
Accuracy with all stages is to be recommended. Registration of the bite is particularly important. Implants offer a tremendous advantage over conventional prosthetics in this respect, as registration equipment can be screwed to the implants (Figures 22–24).
Figure 22. Gnathomat ‘M’ (Ivoclar-Vivadent) modified to record bite registration accurately.Figure 23. Vertical dimension adjusted with central screw.Figure 24. Gothic Arch trace to identify registration position.
The try-in stage should be primarily to confirm:
Aesthetics;
Phonetics;
Occlusion;
Cleansibility.
Particular emphasis is placed on any restorative margins and visibility on full smile.
This involves screwing the abutments to the implants at the correct torque, protecting the screw, often with cotton wool or PTFE tape, and then sealing the access cavities with a resin composite. The use of a prosthetic screwdriver helps to reach difficult access points, providing safer delivery of the prosthetic components. Occlusion is checked and modified if necessary.
The patient is instructed in the oral hygiene aspects of maintenance. A review appointment would normally be made for one week.
Review
At the initial review appointment the occlusion, function, comfort and hygiene should all be checked. In addition, baseline radiographs should be taken, as appropriate, and a timescale for a maintenance regime discussed.
Conclusion
The ability of bone to adhere to biomaterials, in particular titanium, has transformed the field in prosthetic dentistry. Dental implants are now considered routine and many of the sceptics have been converted. Implant dentistry offers a stimulating challenge for the practitioner, where the provision of life-changing treatment is greatly satisfying. Successful implant dentistry does not happen by accident and careful attention to treatment planning, consent, protocol and detail is recommended.