Yildirim GO, Ataoglu H, Kir N, Karaman AI. An alternative method for splinting of traumatized teeth: case reports. Dental Traumatol. 2006; 22:345-349
Kehoe JC. Splinting and replantation after traumatic avulsion. J Am Dent Assoc. 1986; 112:224-230
, 7th edn. Chicago: American Association of Endodontists; 2003
Gahhos F, Ariyan S. Facial fractures: Hippocratic management. Head Neck Surg. 1984; 6:1007-1013
Oikarinen K. Tooth splinting: a review of the literature and consideration of the versatility of a wire-composite splint. Dental Traumatol. 1990; 6:237-250
Andreasen JO. Periodontal healing after replantation of traumatically avulsed human teeth. Assessment by mobility testing and radiography. Acta Odontol Scand. 1975; 35:325-335
Andreasen FM, Andreasen JO, Bayer T. Prognosis of root-fractured incisors: prediction of healing modalities. Endod Dent Traumatol. 1989; 5:11-21
Andreasen FM, Yu Z, Thomsen BL, Andreasen PK. Occurrence of pulp canal obliteration after luxation injuries in permanent dentition. Endod Dent Traumatol. 1987; 3:103-115
Andersson L, Lindskog S, Blomlöf L, Hedström K-G, Hammarström L. Effect of masticatory stimulation on dentoalveolar ankylosis after experimental tooth replacement. Endod Dent Traumatol. 1985; 1:13-16
Cengiz SB, Atac AS, Cehreli ZC. Biomechanical effects of splint types on traumatized tooth: a photoelastic stress analysis. Dent Traumatol. 2006; 22:133-138
Andreasen JO, Andreasen FM, Mejare I, Cvek M. Healing of 400 intra-alveolar root fractures. 2. Effect of treatment factors such as treatment delay, repositioning, splinting type and period and antibiotics. Dent Traumatol. 2004; 20:203-211
Ebeleseder KA, Glockner K, Pertl C, Stadtler R. Splints made of wire and composite: an investigation of lateral tooth mobility in vivo. Endod Dent Traumatol. 1995; 11:288-293
Oikarinen K, Andreasen JO, Andreasen FM. Rigidity of various fixation methods used as dental splints. Endod Dent Traumatol. 1992; 8:113-119
Sübay RK, Sübay MO, Yılmaz B, Kayataş M. Intraradicular splinting of a horizontally fractured central incisor: a case report. Dent Traumatol. 2008; 24:680-684
Hare GC. Multiple replantation of anterior teeth. Oral Surg. 1958; 11:1168-1173
Lello JL, Lello GE. The effect of interdental continuous loop wire splinting and intermaxillary fixation on the marginal gingiva. Int J Oral Maxillofac Surg. 1988; 17:249-252
Oikarinen K. Comparison of the flexibility of various splinting methods for tooth fixation. Int J Oral Maxillofac Surg. 1988; 17:125-127
Alexander PC. Replantation of teeth. Oral Surg. 1956; 9:110-114
Filippi A, von Arx T, Lussi A. Comfort and discomfort of dental trauma splints – a comparison of a new device (TTS) with three commonly used splinting techniques. Dent Traumatol. 2002; 18:275-280
von Arx T, Filippi A, Lussi A. Comparison of a new dental trauma splint device (TTS) with three commonly used splinting techniques. Dent Traumatol. 2001; 17:266-274
Prevost J, Louis JP, Vadot J, Granjon Y. A study of forces originating from orthodontic appliances for splinting of teeth. Endodont Dent Traumatol. 1994; 10:179-184
Fotos P, Spyrakos C, Bernard D. Orthodontic forces generated by a simulated archwire appliance evaluated by the finite element method. Angle Orthod. 1990; 60:277-282
O'Riordan MW, Ralstrom CS, Doerr SE. Treatment of avulsed permanent teeth: an update. J Am Dent Assoc. 1982; 105:1028-1030
Jacob J, Nandlal B. Bond strength of wire-composite resin interface of dental splints using different wire surface treatments – An in vitro study. Endodontology. 2003; 15:2-6
Ganesh M, Tandon S. Versatility of Ribbond in contemporary dental practice. Trends Biomater Artif Organ. 2001; 20:53-58
Andersson L, Friskopp J, Blomlöf L. Fiberglass splinting of traumatized teeth. J Dent Child. 1983; 38:21-24
Kargul B, aglar E, Kabalay U. Glass fiber-reinforced composite resin as fixed space maintainers in children:12–month clinical follow-up. J Dent Child. 2005; 72:109-112
von Arx T, Filippi A, Buser D. Splinting of traumatized teeth with a new device: TTS (Titanium Trauma Splint). Dent Traumatol. 2001; 17:180-184
Adatia A, Kenny DJ. Titanium Trauma Splint: an alternative splinting product. J Can Dent Assoc. 2006; 72:721-723
Nasjleti CE, Castelli WA, Caffesse RG. The effects of different splinting times on replantation of teeth in monkeys. Acta Odontol Scand. 1975; 33:313-323
Wigoper L. Tooth replantation. Br Dent J. 1933; 55
Douglas BL, Douglas W. Clinical observation on replantation of upper anterior teeth. Oral Surg. 1954; 8:27-31
Bakland LK, Camp JH, Trope M, Rossman LE, Walton RE, Dumsha TC. Treating the avulsed permanent tooth. Recommended guidelines of the American Association of Endodontists. Endodontics. 1994;
Andreasen JO. A time-related study of periodontal healing and root resorption activity after replantation of mature permanent incisors in monkeys. Swed Dent J. 1980; 4:101-110
Oikarinen K, Gundlach KKH, Pfeifer G. Late complication of luxation injuries to teeth. Endo Dent Traumatol. 1987; 3:296-302
Neaverth EJ, Goerig AC. Technique and rationale for splinting. J Am Dent Assoc. 1980; 100:56-63
Flores MT, Andersson L, Andreasen JO Guidelines for the management of traumatic dental injuries. I. Fractures and luxations of permanent teeth. International Association for Dental Traumatology. Dent Traumatol. 2007; 23:66-71
Cehreli ZC, Lakshmipathy M, Yazici R. Effect of different splint removal techniques on the surface roughness of human enamel: a three-dimensional optical profilometry analysis. Dent Traumatol. 2008; 24:177-182
The prognosis of a tooth following trauma is critical. This depends on various factors, including the type of splint used for immobilization and the immobilization period. This article discusses the above factors with an added note on splint removal.
Clinical Relevance: This article is relevant for clinicians who treat traumatic injuries as it should help them to decide on the type of splint to be used and the period of immobilization.
Article
One of the questions that arises when a case of trauma is seen is ‘Does this tooth require splinting?’. If yes, consideration is then given to what kind of splint is to be used and for how long? Splinting is required when a tooth has to be immobilized to permit adequate healing following traumatic injuries, such as subluxation, luxation, avulsion and root fracture1 or transplantation.2 This article not only answers the above questions but also focuses on the clinical aspects of splinting traumatized teeth.
The term splint has been defined by the American Association of Endodontics (AAE)3 as a ‘rigid or flexible device or compound used to support, protect or immobilize teeth that have been loosened, replanted, fractured or subjected to certain endodontic surgical procedures.
Hippocrates used wires made of gold and linen for splinting the maxillary and mandibular teeth together.4 Abulcasis, a Spanish physician in the late 10th and early 11th Centuries, used gold, silver or silk ligatures for fixing loosened teeth. Hammond was the first person to use an arch bar splint in 1871. He used a bent metal arch and ligated it to the teeth.5
The design and concept of splinting traumatized teeth evolved from the splints used for immobilization of jaw bones, that required rigid splints for a longer period of time.2 Until the late 1970s, rigid splints were used, which did not allow physiologic tooth movement and were also associated with a greater frequency of pulp necrosis and pulp canal obliteration.6,7,8,9 Semi-rigid splinting is therefore a common and preferred method that allows controlled passive mobilization of the traumatized tooth.10
Requirements for an ideal splint are given in Figure 1. A basic requirement is that the splint should be passive and semi-rigid whilst maintaining physiologic tooth mobility5,11,12,13 (micromovement of less than 150 μm10).
Figure 1. Requirements of a splint.
During splinting, the tooth is immobilized by fixing it to the adjacent unaffected teeth. Generally, the traumatized tooth is fixed to just one tooth on the adjacent side, since evidence does not indicate an additional benefit if the splint is extended to more than one tooth.14 It is also noted that, if the distance between the traumatized tooth and its neighbours is increased, it results in more elastic deviation of the splint and reduced controlled immobilization. This means that the splinting effect may not be the same between spaced arches and non-spaced arches.14
Types of splints
Splints used for immobilizing a traumatized tooth can be classified either as:
These are used when there are multiple missing teeth or during the mixed dentition period when routine devices cannot be placed. They use a soft wire that is fixed around the teeth as a figure of eight (Figure 2) or as a continuous loop. This type of fixation is used when there is need for a short-term intermaxillary fixation.17 The disadvantage of this splint is that the steel wire breaks easily on tightening and the chance of it becoming loose is high. Maintaining oral hygiene is also very difficult and gingivitis is common.18 Since they have a short life, they are recommended to be used only for a few days.
Figure 2. Diagrammatic representation of the suture splint.
Arch bar splints
Arch bars were first introduced by Hammond in the 1870s as splints for maxillary and mandibular fractures.5 They consist of a metal arch bar bent into the shape of an arch which is secured in place with ligature wires (Figure 3). The main disadvantage of this type of splint is that it is a rigid splint and hence its use, in the case of dental injuries, is limited. In addition, where the arch bar is not bent into the correct shape, it can exert orthodontic forces on the tooth. It has also been noted that arch bar splints can become loose and rest on marginal gingivae causing mechanical irritation.19
Figure 3. Arch bar splint.
Acrylic cap splints
This splint is made of rigid acrylic material (Figure 4) and has been used to fix luxated teeth with alveolar fractures.20 It can cause great inconvenience to the patient if prepared directly over the teeth, therefore it is recommended that it be fabricated on a model. But that too has its disadvantage, as it requires an impression, which is contra-indicated in cases of luxation. Therefore, an acrylic cap splint is not routinely used for immobilization of isolated dental trauma.5
Figure 4. Acrylic cap splints.
Composite splints
These splints are fabricated from a band of composite material which is placed directly on the labial surface of the teeth to be splinted together (Figure 5). The resin is applied continuously to the labial surface of the crowns, using a syringe, connecting all the teeth to be splinted.21 Such splints are easy to prepare but they tend to break easily in the interdental region when placed under occlusal load, and therefore are not recommended for long-term splinting.5 It was also noticed, by Filippi et al,21 that composite splints produced an increased irritation to the gingival tissue compared to the use of wire and composite, an orthodontic bracket splint or the titanium trauma splint.
Figure 5. Composite splint.
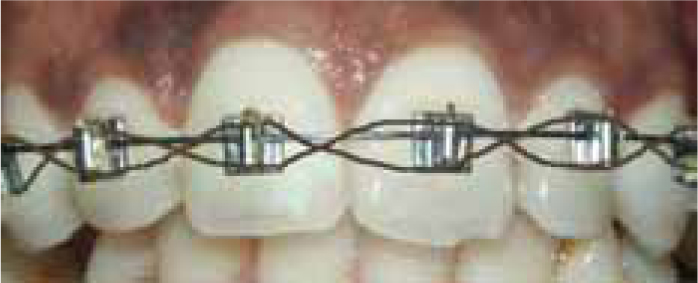
Orthodontic wire and bracket splints
These splints consist of brackets bonded to the middle third of the labial surface of the tooth with light curing composite resin. A 0.3 mm soft wire is then braided from bracket to bracket to connect all the teeth22 (Figure 6). Bracket splints are found to be more irritating to the lips compared to the wire and composite, composite or titanium trauma splints.21 Care should be taken to avoid the application of orthodontic forces on the teeth. Orthodontic wires are never passive and generate forces that range up to 27.33 x 10-2 N, which may result in tipping of the incisors.23,24 The advantage of an orthodontic splint is that simultaneous tooth movement and tooth repositioning is possible when needed.23 It should also be noted that rectangular wires or wires made of nickel titanium are not recommended, since the force developed by these wires is higher than when round/square stainless steel or cobalt-chrome wires are used. This may be due to the higher elasticity of the nickel titanium wires.23
Figure 6. Orthodontic splint.
Wire and composite splints
This was introduced by O'Riordan et al,25 who used a thin flexible wire of diameter 0.3–0.4 mm as a splint. It is a semi-rigid splint secured by light cured composite resin (Figure 7). The wire and composite splint is the most favoured and routinely used splint for immobilizing a traumatized tooth, as it meets most of the demands of modern tooth fixation. This splint can be used in almost all types of tooth injuries. The composite material is placed over the wire on the labial portion without extending into the interdental area. The amount of composite that covers the wire will influence the rigidity of the splint, since it reduces the free and deformable section of the wire. The diameter of the wire used also determines the rigidity of the splint. The less the diameter of the wire used, the more flexible the splint. Thus a wire of diameter 0.3 or 0.4 mm was found to be more flexible than a 0.5 mm wire.19 The only situation where wire and composite splints cannot be used are on teeth with artificial crowns, large fillings where etching of the surface is not possible, teeth restored with porcelain veneer, or where the adjacent teeth are absent. It may be difficult but not impossible to place this splint on teeth with smaller crowns.5
Figure 7. Wire-composite splint.
Bonding between the wire and the composite was a concern. In a study conducted by Jacob and Nandlal, to evaluate the optimal method of enhancing the wire-composite bond strength of dental splints, they found the bond between the stainless steel wire and the composite could be improved by sandblasting the wire.26
Fibre splints
This was introduced by Smith in the 1960s27 and popularized by Andersson et al28 in 1983. The main advantage of the fibre splint is that it does not require any laboratory assistance and is bonded directly on to the teeth (Figure 8). It has good strength, less volume and is aesthetic and repairable.2 Fibre-reinforced composites are resin-based materials containing fibres aimed at enhancing their physical properties. The fibres used are heterogeneous and varied, depending on the nature of the fibre, the geometrical arrangement of the fibres and the overlying resin material. The fibres commonly used are glass, ultra-high strength polyethylene fibre and Kevlar fibres. The properties of the splint depend on the pattern of arrangement of the fibres (unidirectional, meshwork design or woven arrangement). Key factors which influence the physical properties of fibre-reinforced structures are:
Figure 8. Fibre splint.
Fibre loading within the restoration;
Effectiveness of the bond between the fibre resin interface;
Fibre orientation and fibre position in the restoration.27
The commonly used bondable reinforced fibres in clinical practice are:
Glass fibres – GlasSpan (GlasSpan) and Fibre Splint ML (Polydentia);
Fibres pre-impregnated with resin – Vectris (Vivadent), StickNet (StickTech) and FibreKor (Jeneric/Pentron).27
Ribbond is a biocompatible, aesthetic material made from polyethylene fibre, which was in use until recently. The present day splints utilize silanated E-type glass fibres (EverStick, Stick Tech Ltd, Turku, Finland) embedded in a BISGMA matrix and surrounded by PMMA coating (Interpenetrating Polymer Network) with good flexural strength of 1280 Mpa.29
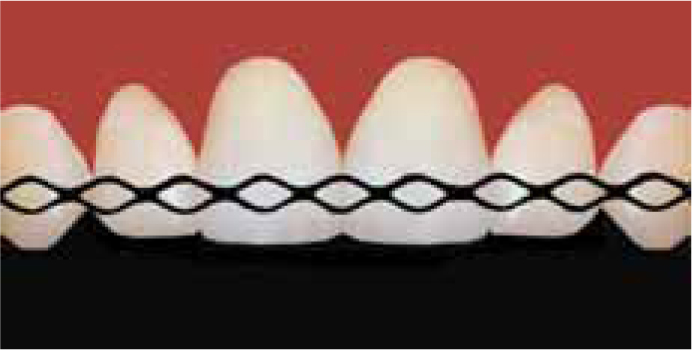
Titanium trauma splints (TTS)
The TTS is a new device developed by von Arx et al.30 It is made of pure titanium and is 0.2 mm thick and 2.8 mm in width (Medartis AG, Basel, Switzerland) (Figure 9). It has a rhomboid mesh structure, making it flexible, to allow for physiologic tooth movement. It can easily be adapted to the contour of the dental arch with fingers without the need of additional pliers. It is easy to cut with any cutting instrument. A TTS splint of about 52mm is required to extend the splint from canine to canine. As it is thin and flexible it can easily be adapted to the desired position. A thin layer of flowable composite is placed into the rhomboid opening of the splint after the application of etch and bonding agent.31
Figure 9. Diagrammatic representation of the titanium trauma splint.
The splint placement comparison study by von Arx et al demonstrated that titanium trauma splints are the easiest and least time consuming to apply (8.5 ± 0.76 min) compared to the wire and composite splint (10.1 ± 1.29 min) or the bracket splint (13.1 ± 0.94 min).22 The amount of composite used to bond the splint to the tooth is small, within the rhomboid opening, making it easier to remove the splint after its use.30 It was also observed that TTS was comfortable for the patient because it was less bulky and did not hinder speech or oral hygiene practice.21
Immobilization period
The period of splinting is crucial for a good prognosis. Initially, it was believed that the longer the splinting period, the better is the healing. But later it was proved that extending the immobilization period led to increased frequency of root resorption and dento-alveolar ankylosis.32 From the earlier immobilization period of 8 months that was practised in the 1930s, it has now been reduced to a few weeks.33 Kehoe2 recommended 2–3 months of immobilization, while Douglas and Douglas34 suggested 6 weeks of splinting for good healing with little or no complications. Andreasen6 has demonstrated that teeth splinted for shorter periods demonstrated better healing than teeth splinted for four or six weeks. It is thus recommended that the period of fixation following avulsion should be kept to a period of 1–2 weeks to avoid root resorption.35,36 It also requires about one week to obtain a strong gingival attachment that is sufficient to support the tooth in the socket following splinting of an extruded tooth.6,35 Extended splinting periods may be required when there is associated injury to the marginal alveolar bone (up to about 6 weeks),37 or in the case of root fractures where immobilization up to 2–4 months may be required.38
The International Association for Dental Traumatology (IADT)39 guidelines for duration of splinting for traumatic injuries are given in Table 1.
Avulsion
Root fracture
Concussion
Subluxation
Extrusion
Lateral luxation
Flexible splint for 2 weeks except when the extra-oral time is >60 minutes.
Stabilize the tooth with a flexible splint for 4 weeks.If the root fracture is near the cervical area of the tooth, stabilization is beneficial for a longer period of time (up to 4 months).
No splinting is needed.Monitor pulpal condition for at least 1 year.
A flexible splint to stabilize the tooth for patient comfort can be used for up to 2 weeks.
Reposition the tooth by gently re-inserting it into the tooth socket Stabilize the tooth for 2 weeks using a flexible splint.
Reposition the tooth with forceps to disengage it from its bony lock and gently reposition it into its original location.Stabilize the tooth for 4 weeks using a flexible splint.
Splint removal
Removal of the splint is as important as placement of the splint. Care must be taken not to cause trauma to the teeth and also to remove all the adhesive material from the tooth surface. Inadequate removal of material may favour plaque accumulation and enamel decalcification. However, over zealous removal of the material from the tooth surface can result in a roughened surface. There are different ways to remove a splint,40 such as using hand scalers, ultrasonic scalers, rubber wheels, abrasive discs, high or low speed burs, tungsten carbide burs, etc. Button brackets are routinely removed with debonding pliers and remaining composite material is chipped off with a curette or a bur.26 The resin from the wire and resin splint is removed with a high speed bur.26 Fibre splints are removed with a tungsten carbide bur. TTS was found to be the easiest to remove. The composite over the TTS is removed down to the level of the splint and the TTS is ‘peeled’ off from the tooth with a haemostat.31 Final polishing of the teeth can be done with finishing discs.1
Splint removal time varied for each splint. It was found to be very fast and easy to remove a titanium trauma splint (3.7 + 0.48 min) compared to the wire and composite splint (6.4 + 2.34 min) or a bracket splint (5.2 + 1.46 min).26
It has been observed that iatrogenic damage to the enamel is common or unavoidable, regardless of the technique used. Debonding with pliers or hand scalers causes the maximum damage, resulting in chipping of the enamel surface. A better technique would be to reduce the bulk of the resin using finishing burs or discs, although it is difficult to recognize the enamel-resin interface without magnification, making it difficult for the clinician to decide ‘when to stop’.40 Soflex discs (3M ESPE, St Paul, MN, USA) and tungsten carbide burs were found to produce least damage to the enamel surface.40
Conclusion
Although there are numerous types of dental splints available to immobilize traumatized teeth, a splint that allows mild physiological movement of the tooth for a minimum period of time, that is easy to place and comfortable to the patient should be the splint of choice. Titanium trauma splints, fibre splints and wire and composite splints fulfil most of these criteria. Titanium trauma splints are not readily available in some countries. Though the choice also depends on the preference of the clinician, these authors prefer fibre splints, as they cause minimum damage to adjacent tissues and are also easy to maintain oral hygiene compared to the wire and composite splints.