Geddis-Regan AR, O'Connor RC. The impact of age and deprivation on NHS payment claims for domiciliary dental care in England. Community Dent Health. 2018; 35:223-227 https://doi.org/10.1922/CDH_4355Geddis-Regan05
Morgan MZ, Johnson IG, Hitchings E Dentist skill and setting to address dental treatment needs of care home residents in Wales. Gerodontology. 2016; 33:461-469 https://doi.org/10.1111/ger.12185
Monaghan NP, Morgan MZ. What proportion of dental care in care homes could be met by direct access to dental therapists or dental hygienists?. Br Dent J. 2015; 219:531-534 https://doi.org/10.1038/sj.bdj.2015.919
Borreani E, Wright D, Scambler S, Gallagher JE. Minimising barriers to dental care in older people. BMC Oral Health. 2008; 8 https://doi.org/10.1186/1472-6831-8-7
El-Yousfi S, Jones K, White S, Marshman Z. A rapid review of barriers to oral healthcare for vulnerable people. Br Dent J. 2019; 227:143-151 https://doi.org/10.1038/s41415-019-0529-7
Sweeney MP, Manton S, Kennedy C Provision of domiciliary dental care by Scottish dentists: a national survey. Br Dent J. 2007; 202 https://doi.org/10.1038/bdj.2007.79
NICE. Oral Health for adults in care homes. NICE guideline [NG48]. 2016. www.nice.org.uk/guidance/ng48 (accessed July 2021)
National Institute for Health and Care Excellence. Oral Health in care homes. Quality Standard (QS151). www.nice.org.uk/guidance/qs151/ (accessed July 2021)
This article examines the planning that goes into successfully providing domiciliary dental care. It includes a comment on patient demand for this type of service, what dental treatment is appropriate to offer, and the impact of relevant legislation introduced over the past 15 years.
CPD/Clinical Relevance: This article highlights some of the considerations that should be taken into account when providing dental care for patients outside the clinic environment when the need arises.
Article
Provision of dental care outside a dental practice can take place in many settings, including a patient's own home, care and nursing homes, hospital wards and schools, and for a number of reasons, including patient frailty. Domiciliary dental care is defined as provision of dental care outside the clinic setting, reaching out to those who cannot attend a clinic-based service, and this differs from dental screenings or epidemiological programmes that may take place in similar settings.1,2 Lewis and Fiske's review2 remains an accurate representation of domiciliary oral healthcare and this article provides an update in the areas most useful for clinicians.
In 2019, the Office for National Statistics reported that the number of people aged 85 and over in the UK is projected to double by 2043.3 As the population continues to age, and older people living with frailty make up a larger proportion of the population, the demand for domiciliary dental care is likely to rise. Geddis-Regan and O'Connor reported that there were 68,063 NHS payment claims for domiciliary dental care for adults in England in 2015. They also noted that service availability may be influenced by provider availability, there was a limited association between levels of deprivation and number of domiciliary claims made, and that access to a service may not always be based on need.4
Geddis-Regan and Walton reported that the prevalence of multimorbidity, defined as the presence of two or more chronic conditions, was 64.9% in those aged 65–84 years and 81% in those aged 85 years and above.5 As a result, 44% of those aged over 65 years take multiple medications daily (polypharmacy). This adds complexity to planning safe dental care for these patients, as well as to interpreting the effects these medications may have on the oral cavity and teeth. Morgan et al6 reported that the commonest complexity was the requirement for spending more time to provide dental care. In a 2015 paper, Monaghan and Morgan7 stated that hygienists or dental therapists could provide a large proportion of the treatment need in care homes.
Domiciliary dental care may also be provided for a range of dental patients other than older people living with frailty and include:
Those with mental health conditions, such as agoraphobia, or severe anxiety induced by attending a dental practice;
School pupils for whom leaving the school to visit a dental practice might be significantly disturbing;
Hospital patients who are required to remain in bed or are unable to leave the hospital due to their medical condition.
Requests for visits may come from a number of sources:
Patients themselves, often because they receive regular dental care on a domiciliary basis and are due for a recall examination or require an unscheduled visit;
Family members of the patient;
Carers of patients who are being supported to live in their own homes;
Care home staff;
Hospital staff;
Other primary care health professionals, such as general medical practitioners or social workers;
Dental practitioners.
Depending on the source of the referral, a questionnaire form may be completed by the dental team with the patient, if possible, or the referrer if this is not possible. An example of a questionnaire can be found in the British Society of Disability and Oral Health document.1 Completion of the form will assist with triaging the necessity and urgency of the request for a domiciliary visit, as well as determining any communication or capacity issues, and enable identification of the initial point of contact and whether they have a valid lasting power of attorney (LPA). This has to be carried out with regard to the General Data Protection Regulations (GDPR),8 but ultimately acting in the patient's best interest while avoiding breaching any patient confidentiality is suggested to be the best approach. Confirmation will be required as to whether the LPA is for health and welfare or finance and property, or is an enduring power of attorney.
After receiving a domiciliary request, the first questions to be asked are whether the patient might be able to attend a dental practice, and if not, the reasons why, and whether any incapacity is short-term so that the dental treatment could wait until the person is more mobile and able to attend the dental practice.
The next challenge can be obtaining a complete medical history. In most circumstances, this may be overcome by providing a medical history form for completion, which is ideally returned to the clinic in advance of the initial appointment. This allows the dental team to be prepared for any medical issues; it also often provides accurate details of the next of kin.
Barriers to dental care
The barriers that exist in relation to domiciliary dental care have been examined in a number of studies. Borreani et al9 reported active barriers, such as cost, fear, availability, accessibility and characteristics of the dentist, and passive barriers such as lack of perception for the need for care. El-Yousfi et al10 reported barriers at an individual level, with the most common being cost or the perception of cost, and at an organizational level, with the lack of availability being the most common barrier. Anecdotally, during discussions at the initial visit, the present authors find that older patients tend not to claim the benefits to which they may be entitled. The reasons for this are beyond the scope of this article, but the result is similar to the barriers mentioned previously. A further barrier can be a lack of awareness that there is a domiciliary service, so that service use often only occurs when a dental problem arises.
There are also barriers from a dentist's perspective. Sweeney et al11 reported that these include time, poor remuneration, concerns about infection control, lack of emergency drugs and suitable equipment, and the difficulties of carrying equipment. Lewis and Fiske2 reported that clinicians can feel that their training was insufficient to prepare them to offer this type of dental care.
Where lack of suitable transport to enable the patient to attend the dental practice is a barrier, community dental services may have access to ambulance transport to bring the patient to the dental clinic. This is particularly necessary when part of the planned dental treatment is inappropriate or unsafe to carry out in a domiciliary environment.
Planning a domiciliary visit
In planning domiciliary visits, a decision is needed on whether a series of appointments for several patients is carried out in a dedicated session, or whether the visits are fitted in around clinical commitments at a dental practice. Whichever approach is chosen, the quality of the service offered must meet the standards set by the General Dental Council12 and the Care Quality Commission (CQC). The CQC assess dental practices and services in England against five pillars,13 namely:
Safety of care;
Effectiveness of care;
Compassion, kindness, dignity and respect from dental staff;
Responsiveness of practice to needs;
Effectiveness of the management of the practice.
Healthcare Inspectorate Wales, NHS Scotland and the Regulation and Quality Improvement Authority carry out dental practice and service assessments in Wales, Scotland and Northern Ireland, respectively. These standards apply equally to dental care provided in a a practice or domiciliary setting and assist in ensuring a patient-centred and effective domiciliary service is provided. Our belief is that a dedicated domiciliary session is more productive and avoids the appearance of rushing to fit in a visit around clinic-based commitments.
An assessment of the requirements for the visit should made when the appointment is booked.2 This will ensure that the required equipment and materials are available. Dental equipment suggestions are available from a number of sources.1,2
To make the best use of the time available, a daily plan is recommended to maximize the number of patients seen, while minimizing the amount of travel between patients. A further consideration is to limit the amount of equipment carried to each visit. Planning involves consideration of:
Where the person lives;
What the dental visit is for and what treatment is likely to be required;
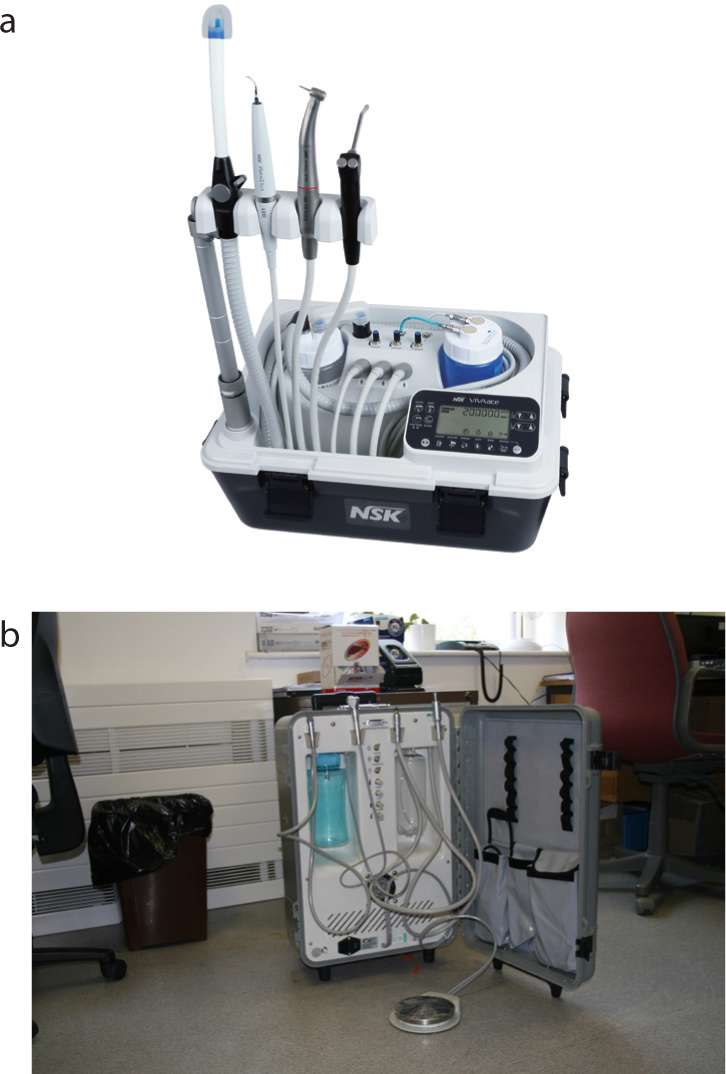
What equipment is likely to be required, whether it is available and in working order (Figure 1). This article reflects domiciliary care planning before the COVID-19 pandemic. Readers are encouraged to consult current guidance on the safe delivery of any type of dental care, including avoidance of aerosol generating procedures, which continue to be developed as changes arise;
Whether any laboratory work is needed and whether it has been received back from the dental technician.
Figure 1.
(a, b) Examples of portable dental units for domiciliary dental care. (Figure 1a courtesy of NSK UK Ltd.)
The next consideration is the most appropriate route from the base clinic to the visit, and also for the series of visits. Local knowledge of routes can be useful at this point and detailed travel directions and information on the availability of parking from the patient can also save time for the first visit. Through planning, the session can be divided up sufficiently to reduce what may need to be brought. Trolley systems can be particularly useful for transporting the required equipment.
Members of the dental team should confirm with their car insurance provider that they are covered for travelling to and from domiciliary visits, including transporting and securing medical gases in the vehicle while travelling, along with any requirements to display a warning sign in the vehicle. An example of a transport emergency card that may be displayed in a vehicle carrying medical gases and clinical waste is shown in Figure 2. The card should be removed from the vehicle when the session is complete.
Figure 2.
(a, b) Transport emergency card for displaying in windscreen.
Although rarely requested, taking photographic identity cards is advised because visits are often to vulnerable persons who may wish the extra reassurance that an identity card can provide.
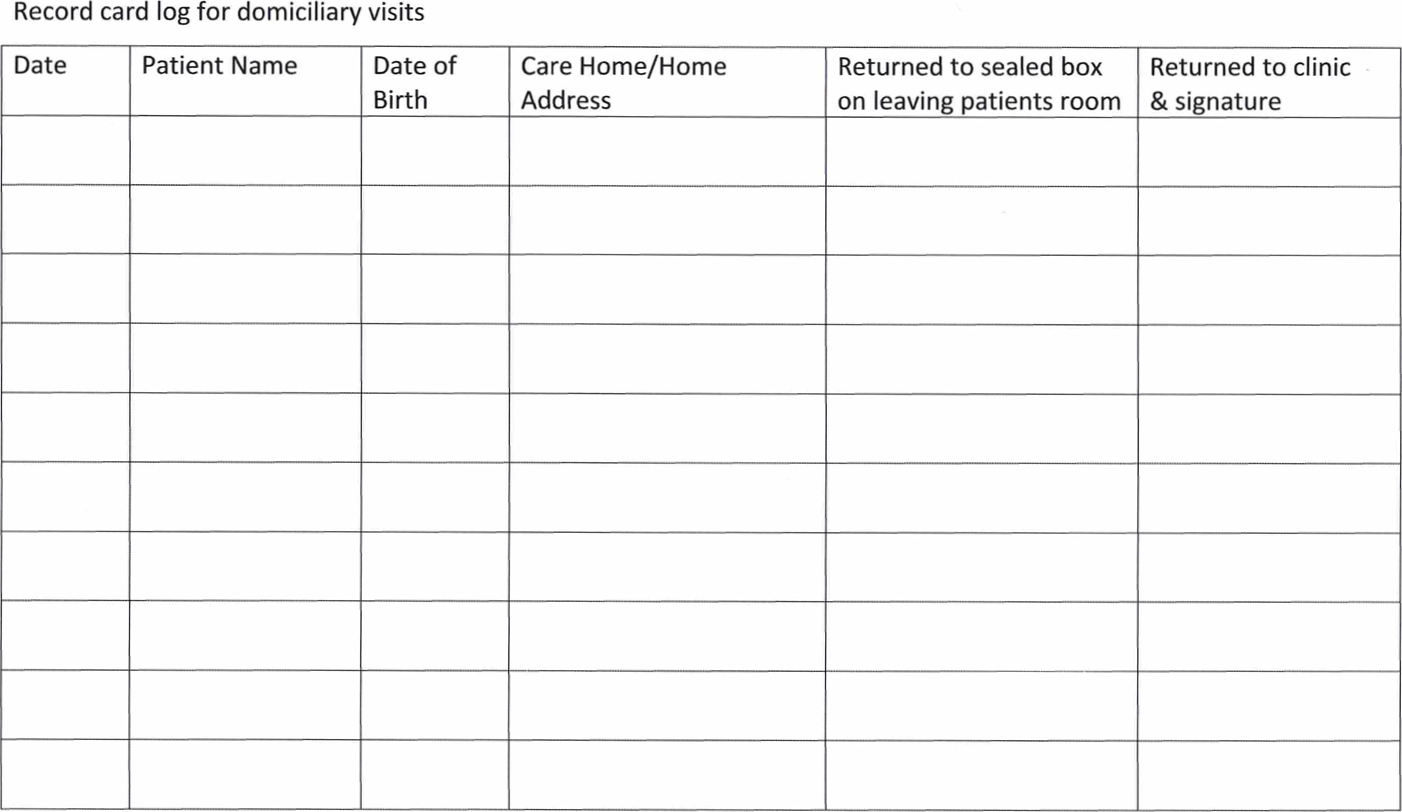
Taking patient record cards out of the dental practice is a risk. They should be transported in a locked container and it is recommended that a checklist is used before leaving each visit to ensure that the cards are safe. An example of a form is shown in Figure 3. In this way any risk to patient confidentiality from a misplaced patient record card is minimized.
Figure 3. Log sheet for patient record cards.
Medical emergency requirements
Emergency drug requirements should be considered. It is suggested that what would be brought is the same as that held in a dental practice environment.
A working and charged mobile phone and prior knowledge of the postcode or grid reference is vital. The what3words app is useful in pinpointing a location, and can be used offline (what3words.com).
The CQC guidance for medical resuscitation equipment in domiciliary dental care14 requires an overall risk assessment of the planned treatment for the patient, the environment in which the visit will take place and the risk of removing the medical emergency equipment from the dental practice.
Routine checks of the emergency drugs and equipment should be carried out before leaving for the domiciliary visits in the same way as those carried out withing the dental practice.
Emergency drugs and equipment should be carried in such a way that they are easily be taken into the visit alongside the required dental equipment. Dental team members should undertake regular simulation exercises to manage medical emergencies that might arise while on a domiciliary visit.
Environmental risk assessment
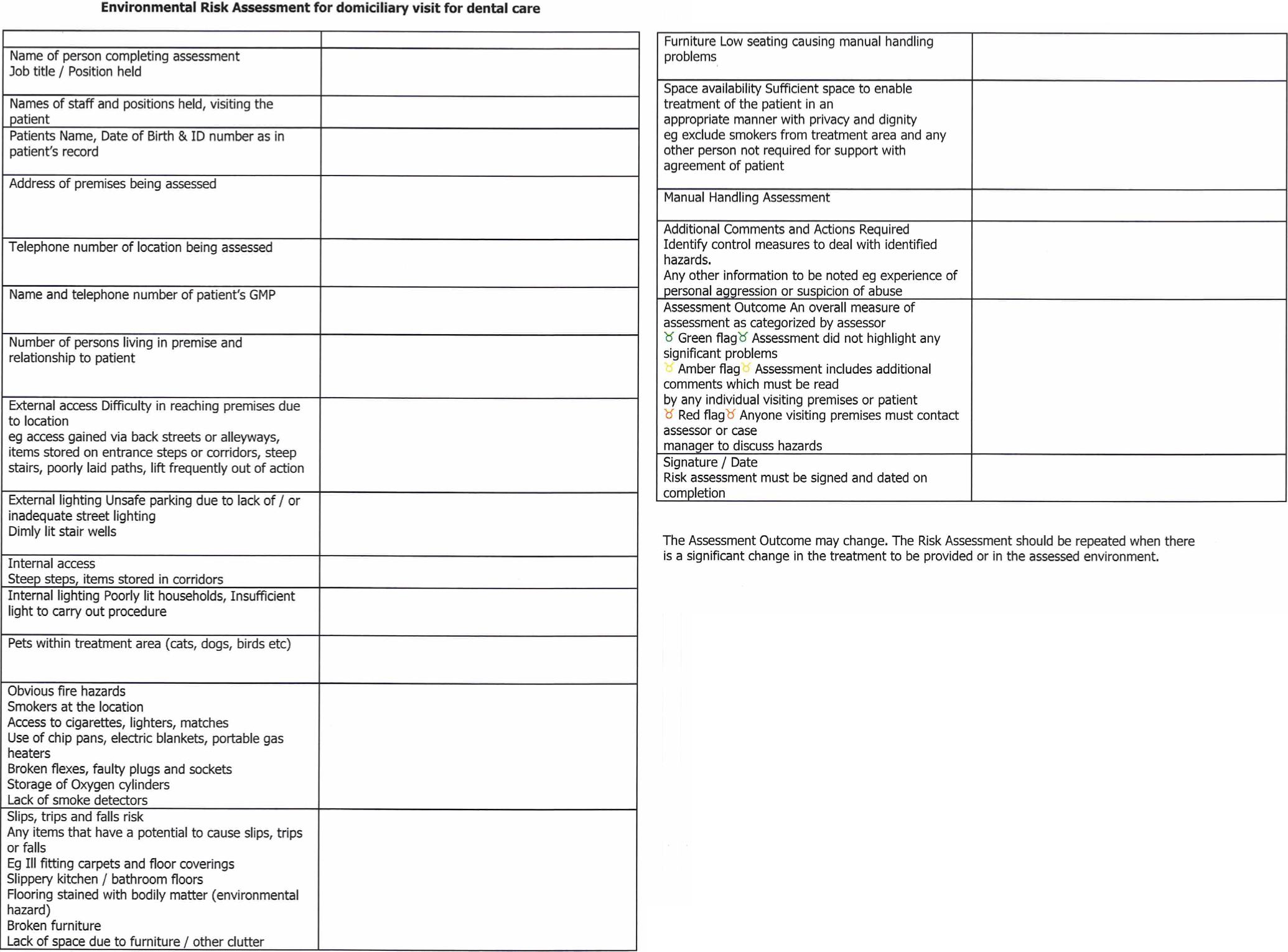
A risk assessment is required for each and every visit as circumstances can change between visits. This is best documented to allow future planning should a patient require a number of visits (Figure 4). Usually a visual check is completed as the visit progresses and any concerns highlighted. If a sufficiently serious concern is identified, it may be necessary to curtail or postpone the visit and explore alternative arrangements for providing care. The patient should also be advised about any concerns and offered support in rectifying them.
Figure 4. Environmental risk assessment form.
Infection prevention and control
The same standard of infection prevention and control is required on a domiciliary visit as that achieved in a dental practice appointment. There is a challenge in meeting this standard and it should be included in the risk assessments completed in advance and on the day of the visit.
Aseptic techniques should be used and a useful guide is available from the Harrogate and District NHS Foundation Trust.15 This will involve ensuring that hand-washing procedures are appropriately carried out, and identifying an area that is prepared and used as the site on which any dental instruments and all clinical waste are placed until the end of the visit. This may be best achieved by using a sterile drape of sufficient size for the procedure intended. It also assists the dental nurse to keep track of everything that is set out and used, and to ensure everything is all removed at the end of the visit. (See the section on the role of the dental nurse for other aspects of their role during domiciliary visits.)
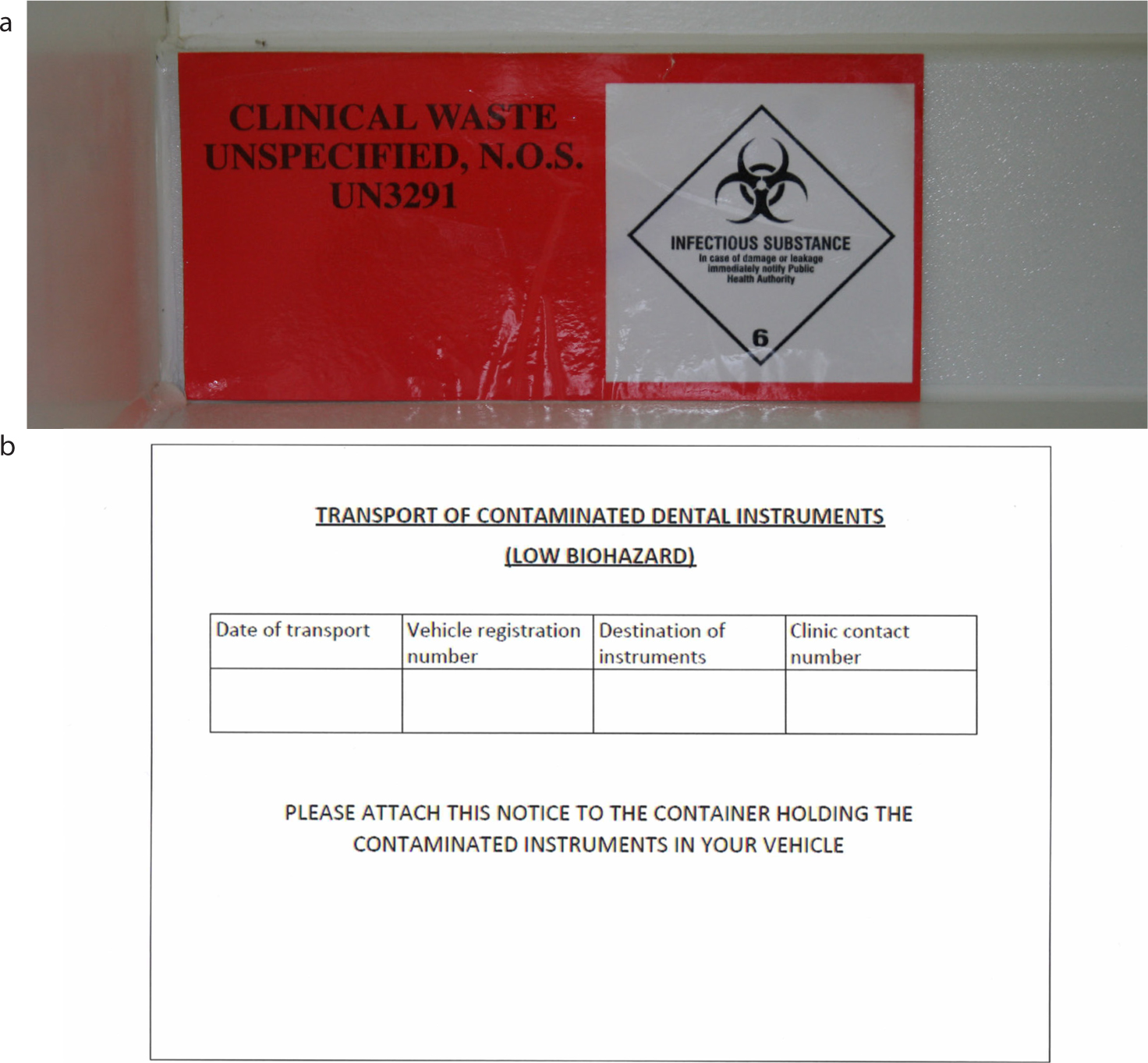
Once a domiciliary visit has been completed, the used dental instruments, any laboratory work and the clinical waste must be removed and transported back to the clinic for disposal or decontamination as appropriate. An example of a suitable transport box is shown in Figure 5. It requires labelling with a clinical waste warning sign as well as the address details and telephone number of the site to which the box is being returned in case of any incident arising before the transport box reaches the clinic (Figure 6). The box should be large enough to accommodate all the waste and used dental instruments accumulated during the visit or series of visits. Various sizes of transport box are available, but it is recommended to consider that the box taken into the domiciliary visit(s) should be small enough for easy handling. It does help concentrate the mind on not taking too many dental instruments on domiciliary visits.
Figure 5. Example of clinical waste transportation box.Figure 6.
(a) Clinical waste warning sign and (b) Clinical waste label to be completed and displayed on the outside of the waste transport box.
What is appropriate dental treatment to carry out on a domiciliary visit?
While the first thought might be that all normal routine dental treatment should be possible to be undertaken on a domiciliary basis, there are a number of considerations regarding what dental treatment is reasonable to be carried out in a domiciliary setting. This could vary depending on the support the patient has once the dental visit has finished. Appropriate dental treatment for a housebound patient who lives alone is likely to be different from that for a patient living in a care home where 24 hour support is available. Irrespective of the site of dental care, there are a number of considerations when planning dental treatment.
Identify the cause of any oral pain or infection, and take steps to resolve this;
Understand the patient's ability and motivations for maintaining a good standard of oral cleaning. This will include identifying any modifications that may be required, such as modifying toothbrush handles for better grip, or liaising with care staff to meet the patients' needs for oral and denture cleaning;
It may be necessary to dress cavities or smooth sharp edges of teeth or fillings that are causing soft tissue trauma. Dressing materials that can be hand mixed and applied are required. There is a range of resin-modified glass ionomer materials available that can meet these requirements, or alternatively, a zinc oxide eugenol cement, such as Kalzinol (Dentsply Sirona, Weybridge, Surrey) may be suitable. The most frequent challenges will be access to the cavity and isolating it from saliva contamination while allowing the material to harden.
Planning the removal of a tooth will need to take into account the patient's medical history and the anticipated difficulty of removal. A grossly mobile tooth is likely to be possible to remove outside a dental clinic without a radiograph; anything more difficult should be planned for a visit to the dental practice, or urgent referral to the local community dental service. The dental practitioner is recommended to be overcautious about attempting complex treatment outside the clinic environment.
Once any oral discomfort is resolved and satisfactory oral and denture cleaning is achieved, then other aspects of dental care, such as restorations and replacement dentures, can be considered. For some patients they may never reach this stage, and pain relief and preventive care maybe all that can be offered.
Unscheduled visits
Unscheduled care can be defined as care that is either requested at short notice, for example when a patient experiences an oral problem, or care that was not part of a previously planned visit, but which results in a change of plan during the visit. In a survey of adults in contact with domiciliary care dental services in 25 primary care trusts across England, Public Health England reported that 14% of those surveyed had a problem or pain in their mouth at the time of the survey, while a further 49% had experienced at least one oral health problem in the previous 12 months.16 Domiciliary dental care services should be flexible enough to be able to react to requests for unscheduled care to at least the same standard as that offered at local dental practice facilities.
Role of the dental nurse
This section considers some additional elements to the role of the dental nurse in the provision of domiciliary dental care.
Communication
Arranging a domiciliary visit is a process of negotiation to arrange the most suitable appointment time, taking into account a patient's or their carers' circumstances as well as those for the dental team. If possible, reduce non-clinical time by travelling to the visit furthest from the dental practice first, working back to the practice during the session. Obtaining travel directions and access arrangements will reduce time spent reaching the patient. Patient confidentiality must be respected and can be achieved by determining the patient's wishes for carers or family to be involved in arranging domiciliary visits and who may be present at the time of the visit. Updating of medical and social histories is recommended at this time.
On-the-day planning
The following steps are recommended:
Contact patients before departure to confirm that there have been no last-minute changes to their circumstances;
Use a dental equipment and instrument checklist for items being taken on the visit, and as an aide-memoire to ensure all items are returned to the clinic;
Check that medical emergency equipment and drugs are available, and ensure that the clinical patient record cards are brought, along with any other appropriate paperwork, such as post-operative instruction sheets.
At the visit
Once the dental team has reached the patient, the role of the dental nurse will be to plan the environment so that it is suitable for providing dental treatment from both an infection control aspect, and also an access aspect. This will include:
Identification and set up of the clinical area with infection control in mind;
Positioning of the patient, whether they are in a bed or a chair, to enable the easiest access for the dental team to provide the dental treatment, while maintaining the patient's comfort and dignity;
Providing a greater communication role than normal. Housebound patients may be lonely and the dental team might be the only people the patient will see that day. Factoring in time to talk is part of a holistic approach to dental care. It also benefits overall care by reducing patient anxiety and improving the social aspect of the examination;
A guarding role is required to discourage inquisitive others, including any pets, from entering the working area, particularly where the dental equipment and materials are laid out for use;
An even greater chaperoning role than in dental practice is required. The dental team must remember that they are visitors to a person's home. This part of the role is especially relevant when visiting patients with memory loss so that any misunderstanding about the visit can be overcome. In circumstances where memory loss could be a risk, then arranging for the patient to have a family member or a carer present can reduce anxiety and avoid any potential challenge about wrong doing;
Ensuring that anything that had been moved to set up the clinical space is returned to the same position at the end of the visit. For patients with limited mobility, forgetting to reposition their walking frame as the visit concludes could increase the risk of falls once the dental team has left.
Care home prevention programmes
There are many benefits to improving basic oral cleaning. These include reduction in oral discomfort and improved quality of the eating experience. In recognizing this, a number of care home-based prevention programmes has been developed within the past 10 years.
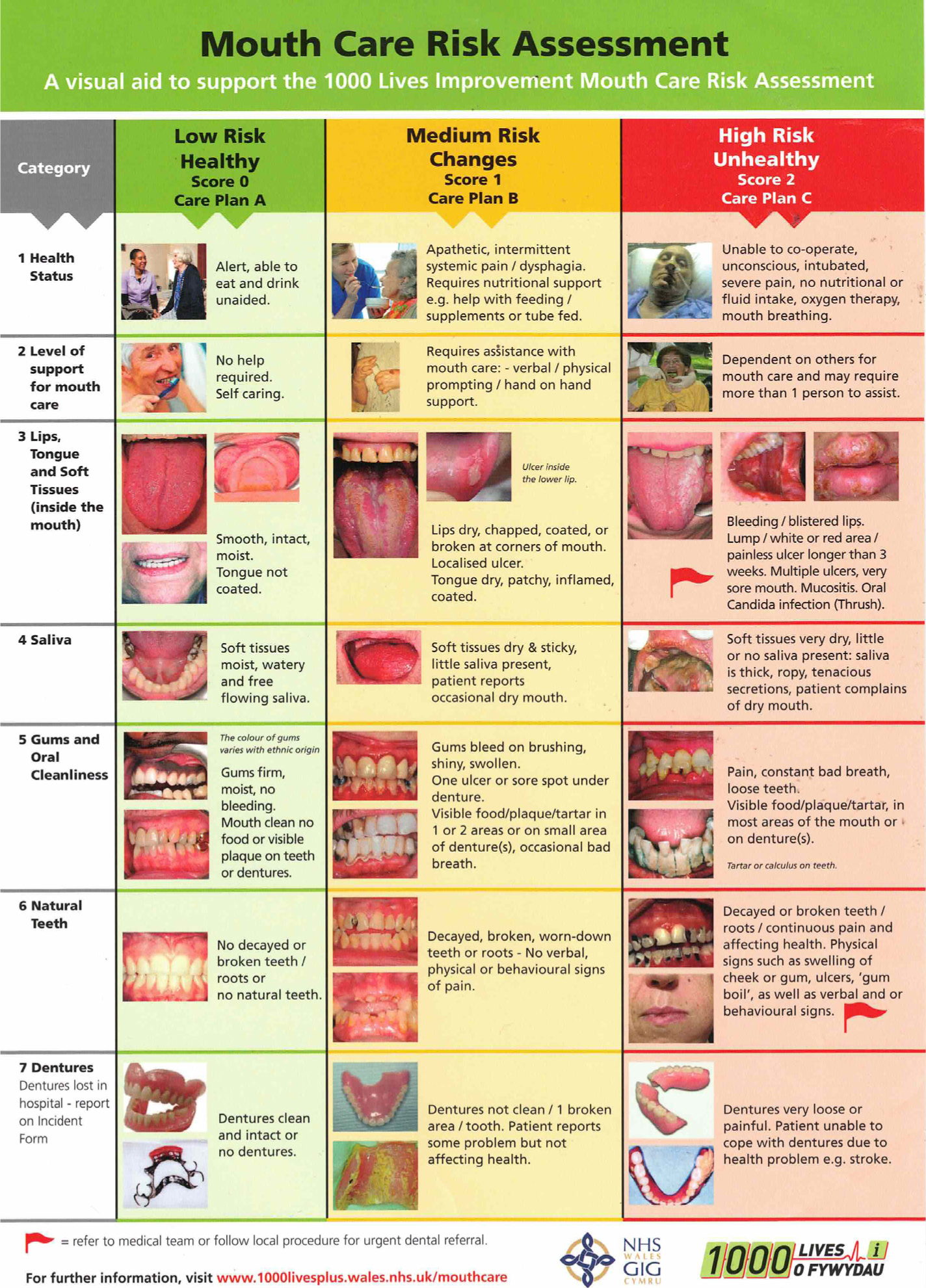
Following the release of a health circular by the Welsh Government in 2015,17 the Gwên am Byth (Smiles Forever) oral health programme was developed. This includes training of care home staff to provide appropriate oral care support and to identify when a dental professional is required. To assist with this, a mouth care risk assessment poster was made available (Figure 7). Funding for this programme was extended to allow the programme to be rolled-out fully to all care homes in Wales during 2020–2021. NHS Health Scotland have also developed the Caring for Smiles programme with similar aims.18
Figure 7. 1000 Lives Mouth Care Risk assessment poster.
In 2016, the National Institute for Health and Care Excellence published the guideline NG48 with the aim of maintaining and improving the oral health of care home residents and ensuring their timely access to dental treatment.19 It was followed up with a three-statement quality standard:20
Residents to have their mouth care needs assessed on admission to the home;
Mouth care needs to be recorded in their personal care plans;
Residents to be supported with teeth and denture cleaning.
In 2019, the CQC identified that care home residents were still not being supported to maintain and improve their oral health.21 This demonstrates that a significant amount of work is still required to make a sustainable success of the oral health improvement programmes running in care homes.
Legislation to consider when providing domiciliary dental care
A number of Acts have been introduced in the past 15 years that have implications for domiciliary dental care and are summarized in Table 1. Other points to consider are:
When a series of visits is required, such as for making a new denture, then extra effort is required to ensure the plan is recalled by the patient at each visit;
The discovery of a lack of capacity may only arise over time while discussing treatment plans and checking a patient's understanding of options and consequences;
All members of the dental team should be vigilant for any signs that could suggest the patient, or anyone else in the property, could be at risk from any form of abuse. Dental team members should receive regular safeguarding training to enable them to be confident in raising any concerns.22
Ensure that dental services are offered that do not discriminate2
Make improvements to the dental practice or, when not possible, make alternative arrangements for domiciliary dental care to be provided
Mental Capacity Act 2007
It must be assumed that a dental patient has the capacity to make a decision unless proved otherwise
It is best to avoid undertaking irreversible or expensive treatment without being certain of the patient's capacity
Confusion or short-term memory loss should not be confused with a lack of capacity
Discussion with their LPA or the possible involvement of an independent mental capacity advocate (IMCA) may help the patient with any decisions that may need to be made
The Health and Social Care Act 2008 (Regulated Activities) regulations 2014
Regulations 9–13 cover patient-centred care, treating patients with dignity and respect, obtaining consent for any intervention, providing safe care and treatment and safeguarding patients from abuse
Places a duty of candour on the dental team (regulation 20) to act in a transparent way regarding dental advice and care provided, especially if an adverse incident occurs
Summary
Dental care provided on a domiciliary basis can be a rewarding experience. Reaching out to those least able to receive care in a dental practice is often gratefully received by patients and their families. It is important to treat domiciliary patients with the same level of care, consideration and planning as patients seen in a clinical practice, while also maintaining an awareness of the less obvious challenges that can arise during domiciliary visits. Adaptability to react to changing conditions as they arise is also important.