Irinakis E, Aleksejuniene J, Shen Y, Haapasalo M. External cervical resorption: a retrospective case-control study. J Endod. 2020; 46:1420-1427 https://doi.org/10.1016/j.joen.2020.05.021
Ahmed HMA, Versiani MA, De-Deus G, Dummer PMH. A new system for classifying root and root canal morphology. Int Endod J. 2017; 50:761-770 https://doi.org/10.1111/iej.12685
Wolf TG, Anderegg AL, Yilmaz B, Campus G. Root canal morphology and configuration of the mandibular canine: a systematic review. Int J Environ Res Public Health. 2021; 18 https://doi.org/10.3390/ijerph181910197
Patel S, Mavridou AM, Lambrechts P, Saberi N. External cervical resorption – part 1: histopathology, distribution and presentation. Int Endod J. 2018; 51:1205-1223 https://doi.org/10.1111/iej.12942
Patel S, Foschi F, Mannocci F, Patel K. External cervical resorption: a three-dimensional classification. Int Endod J. 2018; 51:206-214 https://doi.org/10.1111/iej.12824
Bourguignon C, Cohenca N, Lauridsen E International Association of Dental Traumatology guidelines for the management of traumatic dental injuries: 1. Fractures and luxations. Dent Traumatol. 2020; 36:314-330 https://doi.org/10.1111/edt.12578
Krastl G, Weiger R, Filippi A Endodontic management of traumatized permanent teeth: a comprehensive review. Int Endod J. 2021; 54:1221-1245 https://doi.org/10.1111/iej.13508
Marotti M, Ebeleseder KA, Schwantzer G, Jauk S. A retrospective study of isolated fractures of the alveolar process in the permanent dentition. Dent Traumatol. 2017; 33:165-174 https://doi.org/10.1111/edt.12325
Lauridsen E, Gerds T, Andreasen JO. Alveolar process fractures in the permanent dentition. Part 2. The risk of healing complications in teeth involved in an alveolar process fracture. Dent Traumatol. 2016; 32:128-139 https://doi.org/10.1111/edt.12229
Patel S, Foschi F, Condon R External cervical resorption: part 2 – management. Int Endod J. 2018; 51:1224-1238 https://doi.org/10.1111/iej.12946
Heithersay G. Invasive cervical resorption. Endod Topics. 2004; 7:73-92
Andreasen JO, Farik B, Munksgaard EC. Long-term calcium hydroxide as a root canal dressing may increase risk of root fracture. Dent Traumatol. 2002; 18:134-137 https://doi.org/10.1034/j.1600-9657.2002.00097.x
Debelian G, Trope M. The use of premixed bioceramic materials in endodontics. Giornale Italiano di Endodonzia. 2016; 30:70-80
Mao L, Liu J, Zhao J Effect of micro-nano-hybrid structured hydroxyapatite bioceramics on osteogenic and cementogenic differentiation of human periodontal ligament stem cell via Wnt signaling pathway. Int J Nanomedicine. 2015; 10:7031-7044 https://doi.org/10.2147/IJN.S90343
Management of a Case of External Infection-related (Inflammatory) Root Resorption in Communication with the Root Canal System Shakil Umerji Fadi Jarad Dental Update 2025 50:9, 787-791.
Resorption is a physiological or pathological process resulting in the loss of dental hard tissue with or without bone loss. We present the case of a 19-year-old patient who presented with a discoloured and symptomatic mandibular canine tooth with complex root canal morphology. The tooth was located at the site of a previous alveolar fracture. Delayed presentation had led to severe external infection-related (inflammatory) root resorption. The protocol and rationale for non-surgical management of the case in a multi-visit approach is outlined.
CPD/Clinical Relevance: The aetiology and presentations of external root resorption is useful information for clinicians
Article
Resorption is a physiological or pathological process resulting in the loss of dental hard tissue with or without bone loss. It can affect the internal or external root surfaces and occurs in both primary and secondary dentitions. The process in the permanent dentition is pathological1 and can be attributed to infection, dento-alveolar trauma, orthodontic treatment, impacted teeth or expanding pathological lesions, tooth whitening, iatrogenic damage or even idiopathic development. Resorption is initiated as a result of injury to the protective layer of either cementum (external resorption) or predentine (internal resorption) and progresses via a stimulating factor. Stimulating factors may include the presence of bacteria and toxic chemicals, such as whitening agents.2
In external inflammatory root resorption (EIRR), this stimulation is most commonly from bacterial infection of the root canal system. External cervical resorption (ECR) develops at the cervical margin below the epithelial attachment of the tooth.3 Aetiology of ECR is inconclusive; however, both inflammatory and infective processes have been suggested.2 The most common predisposing factors reported for ECR include dento-alveolar trauma, orthodontic treatment, non-vital bleaching, periodontal treatment, as well as idiopathic cases.3
History
A 19-year-old male patient was referred to a dental hospital for root canal treatment of LR3, the lower right canine. The patient reported an incident of trauma, an assault (punch to the face) that resulted in a right parasymphyseal fracture 4 years previously. This was treated with open reduction internal fixation (ORIF) in an oral and maxillofacial surgery department. Since the previous year, the LR3 had discoloured and there had been intermittent pain. The patient's general dental practitioner made a diagnosis of EIRR and initiated treatment with an extirpation of the pulp and a calcium hydroxide dressing.
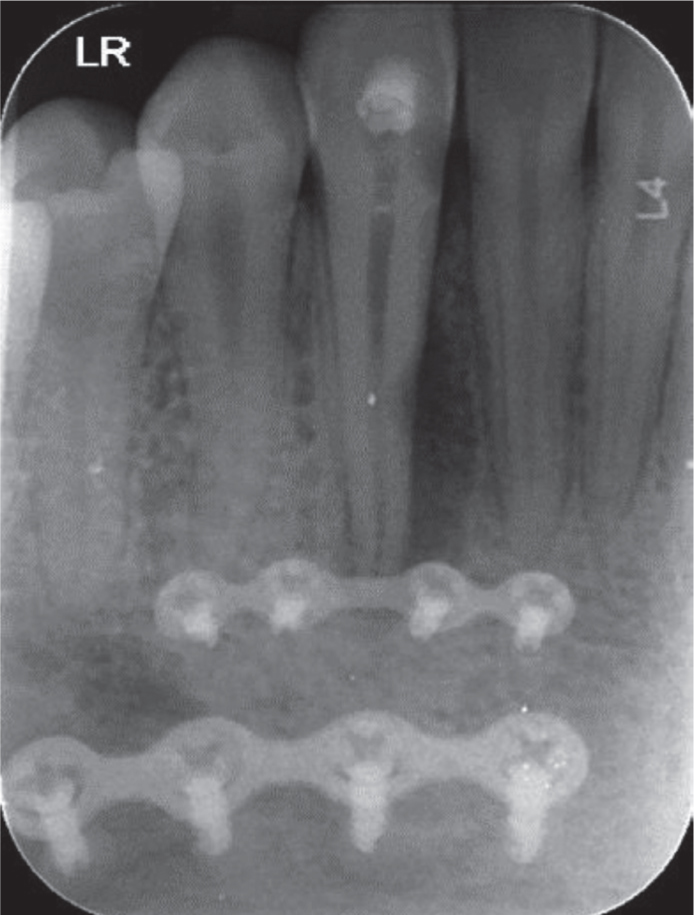
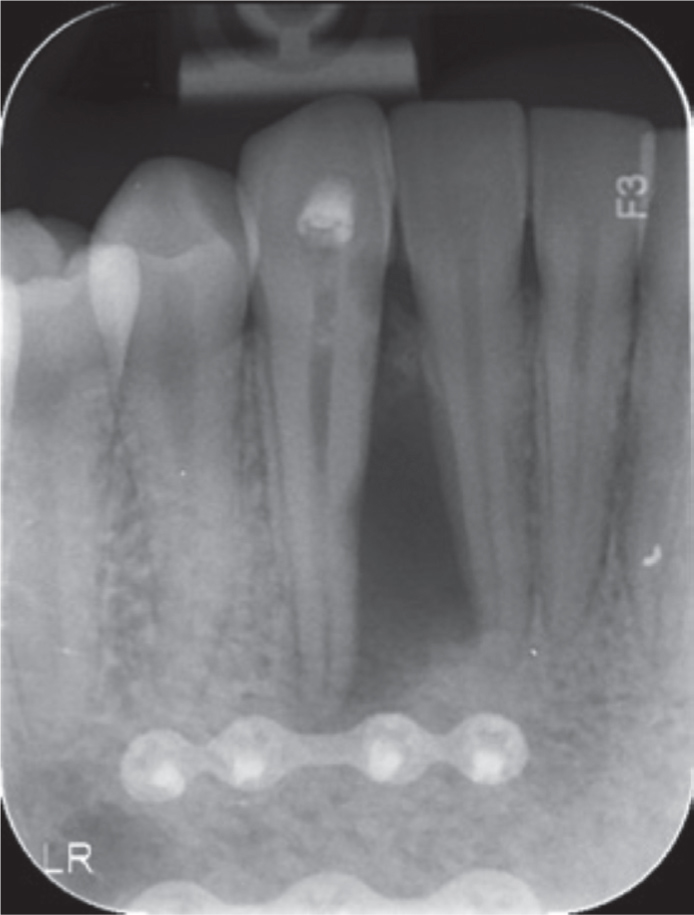
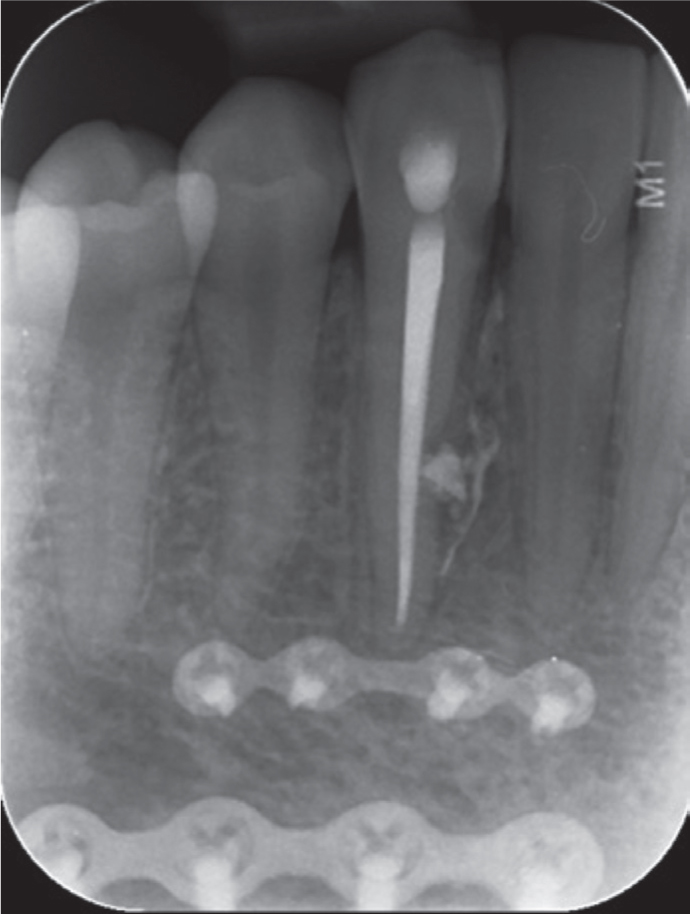
Figure 1. Pre-operative peri-apical radiograph taken at the initial assessment in May 2018.Figure 2. Pre-operative peri-apical radiograph taken in July 2019.Figure 3. Peri-apical radiograph taken at 13-month review in 2021.Figure 4. Intra-oral view highlighting the patient's chief complaint of discolouration.
Assessment
In addition to the initial diagnosis of EIRR in the middle third of the root, resorption was also identified at the mesio-cervical root surface. This could either have been a distinct resorptive lesion (ECR), or an extension of the EIRR to affect the mid-third of the root. The latter would be more consistent with the history of trauma: the alveolar fracture was located mesial to LR3. Injury to the PDL along the mesial root surface at the time of trauma, as well as during fracture reduction, would be likely to have contributed to the initiation of the resorptive process.
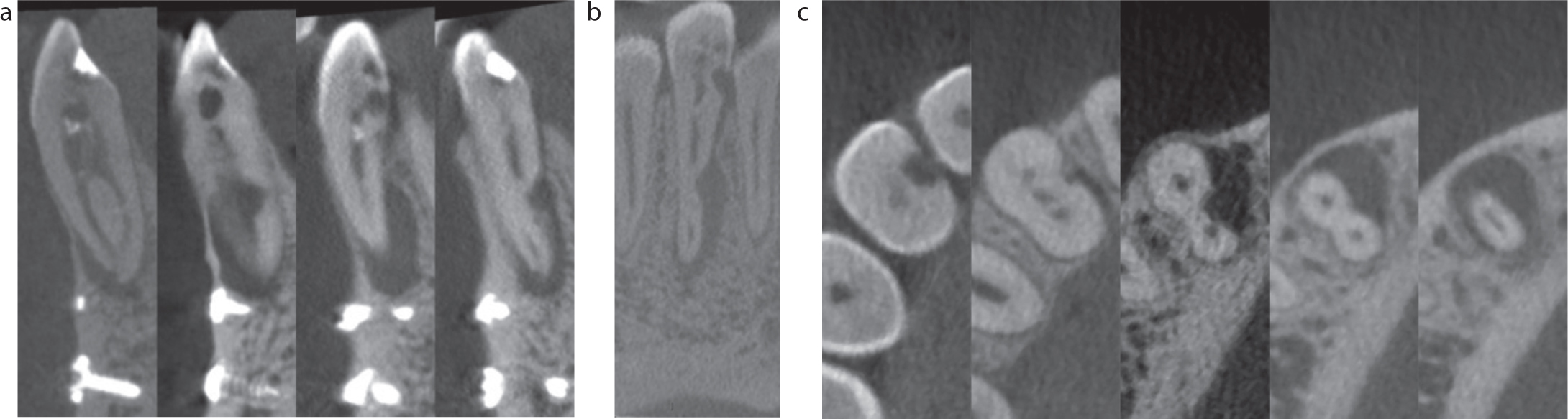
Cone beam computed tomography (CBCT) was prescribed (Figure 5) to assess the extent of resorption and inform the management strategy. A bifurcation of the root canal was identified in the mid-third of the root. This canal morphology could be described as a ‘Type III (1-2-1)’ using the commonly used Vertucci (1984) classification.4 Whereas, using the more extensive Ahmed (2016) classification, the tooth would be noted as ‘1431-2-1’.5 This would indicate a single-rooted mandibular right canine, with one orifice and one canal initially which then bifurcates into two independent canals and merges again and terminates in one canal at the apical foramen. This pattern has a prevalence of 0.9–20% in the literature for mandibular canine teeth.6 The CBCT scan also identified a communication of the lingual canal with the resorptive lesion in the middle third of the root. This indicated advanced progression because the protective pre-dentine layer had been perforated.
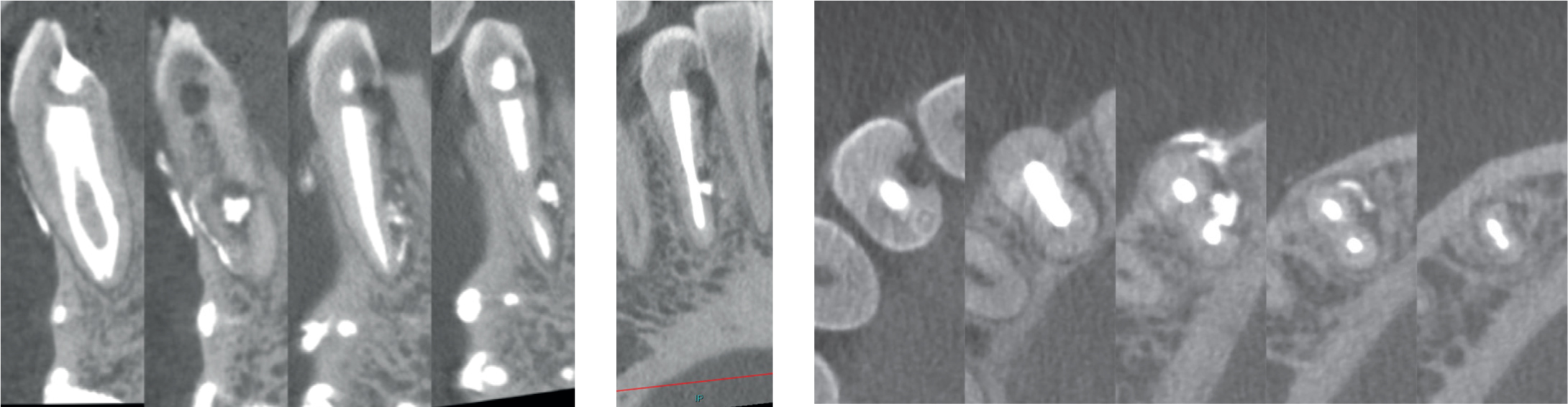
Figure 5. CBCT scan with (a) sagittal (b) coronal and (c) axial views. The scan hightlights a Vertucci Type III (1-2-1) or Ahmed Class 1431-2-1 canal morphology,6 as well as the extent of both resorptive areas. The mid-apical third resorptive lesion has perforated the lingual canal space. Surgical access for the cervical lesion (‘ECR’ 3D Patel Classification: 3Ad)8 would be unfeasibly destructive.
The more cervical resorptive lesion was located proximally and entirely sub-crestally. The resorptive pattern was not consistent with ECR, which typically has a more invasive pattern of spread than that seen in this case.3,7
Management
Treatment was significantly disrupted because of missed appointments, leading to disease progression. Root canal treatment was eventually commenced 1 year later and completed over two visits.
The peri-radicular radiolucency had significantly progressed since the initial assessment. Instrumentation of the root canal system was completed using a rotary NiTi system (ProTaper Next, Dentsply Sirona; master apical files: labial canal X2 and lingual canal X2), and 1% NaOCl was used for irrigation. Passive ultrasonic irrigation was also implemented for irrigant activation. Non-setting calcium hydroxide (Ultracal, Ultradent, USA) was used as an intracanal medicament.
There was a further 6-month delay after the first visit owing to limited patient availability. The patient reported the tooth to be asymptomatic, and a dressing review radiograph was taken, which showed favourable healing and stabilization of the resorption. Therefore, treatment was completed at the second visit. The canals were irrigated once again with 1% NaOCl and activated using passive ultrasonic irrigation; 17% EDTA was also used as a penultimate rinse. Obturation was completed using Gutta Percha and a calcium silicate sealer (TotalFill BC Sealer, FKG Dentaire, Switzerland) with warm vertical compaction to the canal bifurcation, a modified hydraulic condensation technique.
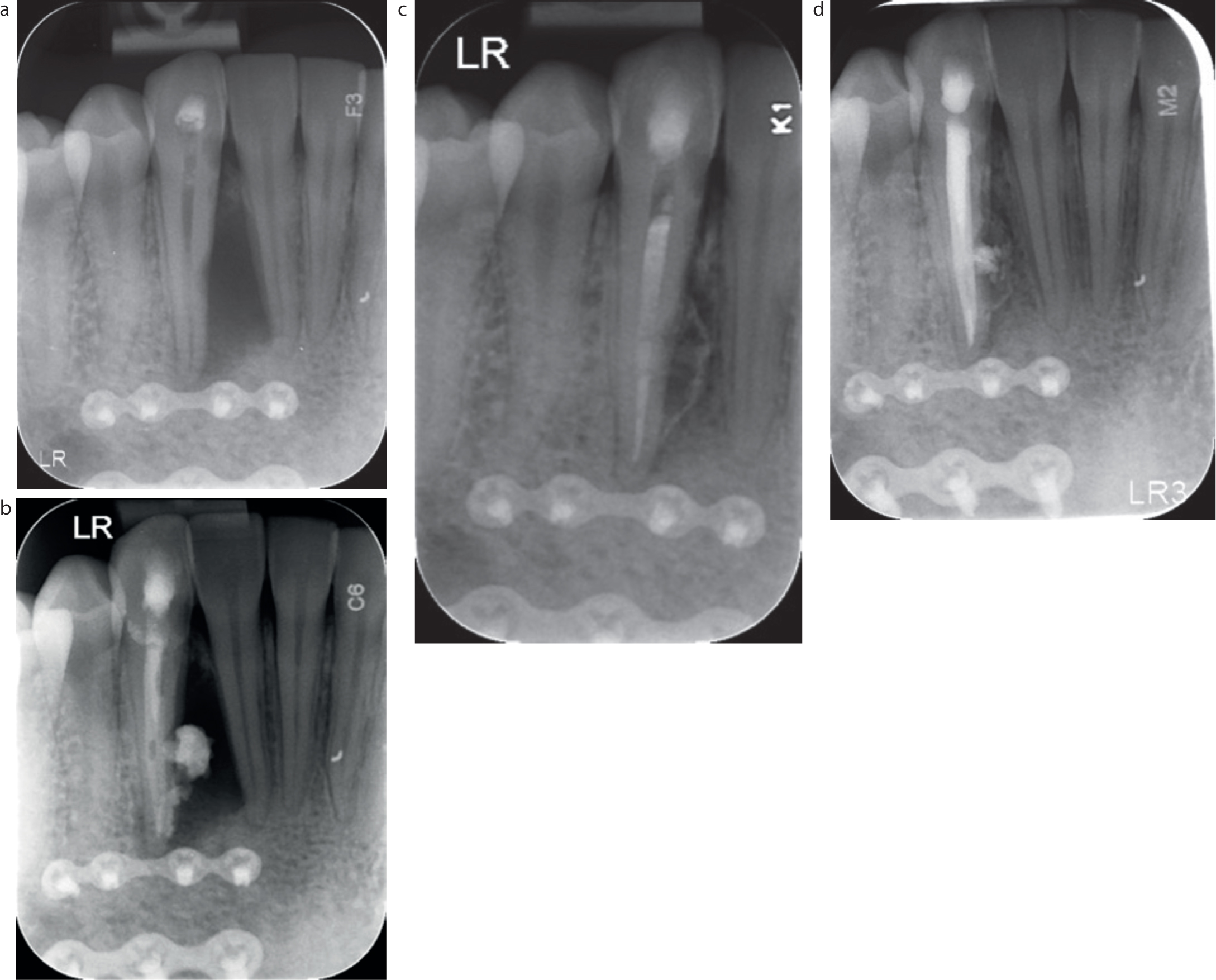
Figure 6. Peri-apical radiographs at each stage of treatment; (a) Pre-operative status at the first treatment visit (July 2019), (b) Post-operative radiograph after dressing with non-setting calcium hydroxide (July 2019), (c) Radiograph taken at the second treatment visit (January 2020) to review healing after an extended dressing period of 6 months due to patient availability, (d) Post-operative radiograph following obturation at the second treatment visit (January 2020).
The merits of surgical repair for the cervical resorptive defect were also considered. However, because the lesion was located proximally and entirely sub-crestally, access for surgical management would have been challenging, but also destructive. It was therefore more appropriate to keep the lesion under review, particularly because the resorption was deemed to be infection related (EIRR) rather than invasive in nature (ECR).
Outcome
At the 6-month review, the peri-radicular radiolucency had completely resolved. The patient was also reviewed at 8 and 13 months post-operatively (initial delay due to COVID-19 pandemic). The patient reported to be asymptomatic and radiographic review showed no progression of resorption. In line with the International Association of Dental Traumatology guidelines,9 monitoring of the patient annually for up to 5 years was planned.
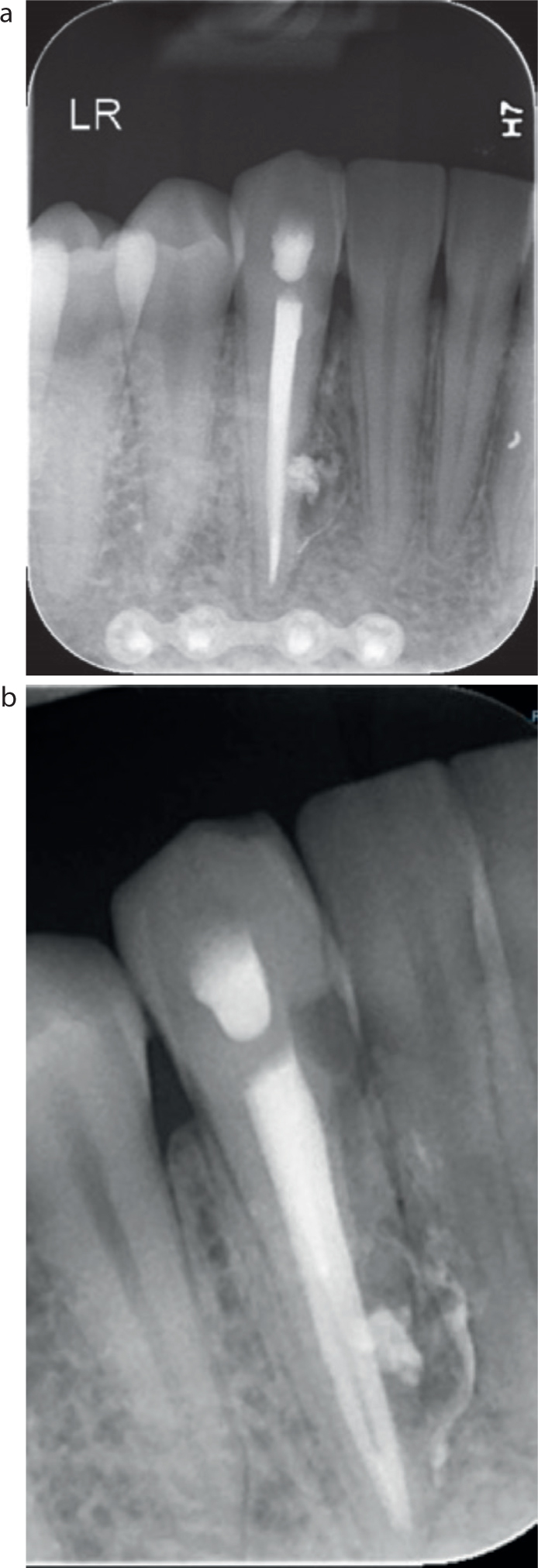
Figure 7. Peri-apical radiographs taken with (a) parallel and (b) mesial cone shift views at the 8-month review.Figure 8. Peri-apical radiographs taken at the 13-month review (February 2021).Figure 9. A CBCT scan was carried out at the 13-month review to check for resorption progression. The resorptive defects had not progressed and appeared to be stable. Furthermore, complete radiographic healing of the peri-apical lesion was evident.
Discussion
The prognosis of teeth located at the site of an alveolar fracture line is determined by the type of concomitant dental trauma rather than the alveolar injury itself.10 It was historically advocated for teeth located at fracture sites to be extracted to reduce the risk of osteomyelitis or impaired fracture union.11 However, it is now accepted that teeth located at the site of an alveolar fracture have no significant impact on alveolar healing, and extraction should be avoided without further indication.10,11 Furthermore, when managed conservatively, teeth located at the site of an isolated alveolar fracture line have a good prognosis.12 However, there is a 2.5–7.2% reported risk of developing infection-related resorption.12,13 Swift intervention is crucial to remove the source of inflammation and limit disease progression. Adequate imaging is also required to assess the severity and extent of resorptive lesions to inform treatment planning.
It is debatable whether this case involves true external cervical resorption. As noted earlier, the cervical defect could have been diagnosed as EIRR, that is the same pathological process resulting in the resorptive defect visible at the mid-third of the root. As a definitive diagnosis was not possible, the treatment strategy considered both possibilities. Management of ECR usually involves a pro-active approach of surgical intervention to treat and restore the resorptive defect.14 Periodic review may also be undertaken, with isolated case reports of self-limiting cases with evidence of ‘repair’ via replacement resorption.15,16 However, this approach should be reserved for untreatable cases.14 It would otherwise be a high-risk strategy and should be avoided where possible, given that progression can render the tooth unrestorable. Treatment planning decisions are informed based on the balance of risk versus benefit.
In this case, if the lesion had been attributed to ECR, owing to the unfavourable access for surgery, conservative management of the lesion with regular monitoring, including a CBCT review at 1 year was decided. Furthermore, if as suspected, the diagnosis of the cervical lesion was EIRR rather than ECR, then surgical intervention was not indicated, given that endodontic treatment had removed the infected pulp, the stimulating factor for progression.
Although the short-term outcome was favourable, the long-term prognosis for the tooth should still be regarded as uncertain. Should the cervical lesion progress, the tooth would be unrestorable. Additionally, although the patient's initial complaint included discolouration, non-vital bleaching was contraindicated given the associated risk of stimulating ECR.
Biomaterials are advantageous in managing resorption. Calcium hydroxide has been shown to inactivate osteoclastic activity and thus cease progression. However, dressing for as long as 6 months is not recommended owing to the increased susceptibility of root fracture with prolonged Ca(OH)2 dressings.17,18
Calcium silicate-based (bioceramic) sealers also release calcium hydroxide on setting,19 in addition to promoting cementogenesis and osteogenesis.20 As well as being biocompatible, their use in a hydraulic condensation technique makes for a simplified and predictable obturation in the presence of communicating resorptive defects.
Conclusion
This case demonstrates the importance of a meticulous assessment in the diagnosis of external infection-related root resorption. With an appropriate diagnosis, conservative management of dental trauma-related complications may be considered and advocated.