Alvarez S, Schultz JH. A communication-focused curriculum for dental students – an experiential training approach. BMC Med Educ. 2018; 18 https://doi.org/10.1186/s12909-018-1174-6
Botelho MG, Lee UYA, Luk KYC. An exploration of clinical communication needs among undergraduate dental students. Eur J Dent Educ. 2023; 27:707-718 https://doi.org/10.1111/eje.12859
Rollnick S, Butler CC, Stott N. Helping smokers make decisions: the enhancement of brief intervention for general medical practice. Patient Educ Couns. 1997; 31:191-203 https://doi.org/10.1016/s0738-3991(97)01004-5
Akuagwuagwu C, van der Pol M, Boyers D. UK general population willingness to pay for scale and polish, and detailed and personalized oral hygiene advice. Community Dent Oral Epidemiol. 2022; 50:233-242 https://doi.org/10.1111/cdoe.12657
Williams KA, Mithani S, Sadeghi G, Palomo L. Effectiveness of oral hygiene instructions given in computer-assisted format versus a self-care instructor. Dent J (Basel). 2018; 6 https://doi.org/10.3390/dj6010002
National Institute for Health and Care Excellence. Oral health promotion: general dental practice. NG30. 2015. www.nice.org.uk/guidance/ng30 (accessed January 2025)
National Institute for Health and Care Excellence. Tobacco: preventing uptake, promoting quitting and treating dependence. NG209. 2023. www.nice.org.uk/guidance/ng209 (accessed January 2025)
Tomar SL, Asma S. Smoking-attributable periodontitis in the United States: findings from NHANES III. National Health and Nutrition Examination Survey. J Periodontol. 2000; 71:743-751 https://doi.org/10.1902/jop.2000.71.5.743
Scottish Dental Clinical Effectiveness Programme. Prevention and treatment of periodontal diseases in primary care. 2024. www.periodontalcare.sdcep.org.uk/ (accessed January 2025)
Delgado-Lobete L, Montes-Montes R, Vila-Paz A Individual and environmental factors associated with tobacco smoking, alcohol abuse and illegal drug consumption in university students: a mediating analysis. Int J Environ Res Public Health. 2020; 17 https://doi.org/10.3390/ijerph17093019
Li J, Wang H, Li M Effect of alcohol use disorders and alcohol intake on the risk of subsequent depressive symptoms: a systematic review and meta-analysis of cohort studies. Addiction. 2020; 115:1224-1243 https://doi.org/10.1111/add.14935
Boniface S, Shelton N. How is alcohol consumption affected if we account for under-reporting? A hypothetical scenario. Eur J Public Health. 2013; 23:1076-1081 https://doi.org/10.1093/eurpub/ckt016
LoConte NK, Brewster AM, Kaur JS Alcohol and cancer: a statement of the American Society of Clinical Oncology. J Clin Oncol. 2018; 36:83-93 https://doi.org/10.1200/JCO.2017.76.1155
Hashibe M, Brennan P, Chuang SC Interaction between tobacco and alcohol use and the risk of head and neck cancer: pooled analysis in the International Head and Neck Cancer Epidemiology Consortium. Cancer Epidemiol Biomarkers Prev. 2009; 18:541-550 https://doi.org/10.1158/1055-9965.EPI-08-0347
Kaner EF, Beyer FR, Muirhead C Effectiveness of brief alcohol interventions in primary care populations. Cochrane Database Syst Rev. 2018; 2:(2) https://doi.org/10.1002/14651858.CD004148.pub4
Mudhar O, Bradley N, Samuel M. What's the deal? The importance of asking about recreational drug use in dental settings. Dent Update. 2023; 50:589-594 https://doi.org/10.12968/denu.2023.50.7.589
Watt RG, Steele JG, Treasure ET Adult Dental Health Survey 2009: implications of findings for clinical practice and oral health policy. Br Dent J. 2013; 214:71-75 https://doi.org/10.1038/sj.bdj.2013.50
BDS, MA (Hons), GMBPsS, PG Cert Med Ed, MFDS (RCS ENG), MFDS, RCPS (Glasg), FHEA, Clinical Lecturer (Scholarship), Institute of Dentistry, University of Aberdeen
Good communication between dentist and patient is essential. The ability to communicate with patients about sensitive topics can also improve patient outcomes and help facilitate positive behaviour change. This article reviews ways in which sensitive topics, including oral health, smoking, alcohol use, recreational drug use and diet, can be approached by dental professionals. Dental professionals are well placed to give comprehensive advice concerning oral health. Other topics can be approached using brief interventions that can be carried out within the limited time available to dental practitioners. Brief intervention is an approach to assess and increase patients' motivation or readiness to change unhealthy behaviours. Self-help materials that patients can be given and signposted to are also highlighted.
CPD/Clinical Relevance: Structured approaches are available to assist dental clinicians to have conversations with patients around sensitive topics.
Article
Former US president, Gerald R Ford, is quoted as saying: ‘Nothing in life is more important than the ability to communicate effectively.’ Being able to communicate is vital for the dental profession.1 The General Dental Council (GDC) deems communication with patients so important that ‘Communicate effectively with patients’ is the second principle of the ‘Standards’ for the dental team.2
Communicating with patients pervades many areas of a dental professional's working life. This runs from communicating with potential patients, gaining consent, discussing treatment options and financial matters, to taking a comprehensive history. Generally, the public attends the dentist even when well, making GDPs ideally suited to provide healthcare messages to those not often in contact with other practitioners.
Dental professionals are required to record and act on information obtained through a comprehensive history, which requires good conversational skills. Some topics are sensitive, but the information gleaned can be essential to inform of risk, allow patients to make informed decisions regarding their health, for oral health assessment and for the formation of long-term care plans. Additionally, guidance exists regarding what should be recorded.3 Failure to do so may result in medico-legal consequences.
The natural ability to talk to patients varies between individual clinicians. A study by Botelho et al found that undergraduate dental students had low confidence regarding communicating with patients and, if communication skills have not been mastered as an undergraduate, opportunities to learn such skills dwindle in the often-isolated primary care environment.4
John Powell, a film composer, noted that: ‘Communication works for those who work at it.’ However, knowing how to start can be daunting for those who are more reserved.
Conversations between the dental professional and the patient must be about more than the weather and holidays. The focus of this article is to examine some of the essential, but more sensitive, conversational topics and present existing tools or models to help provide a framework for some of the more challenging conversations.
Medical history to start conversation
Discussions are best initiated from the questions in the medical history form, which should incorporate sensitive topics. Patients should be made aware that these questions are asked of all patients and that they have not been singled out for such questioning.
The questions may prompt the patient to think about their lifestyle choices, which can lead to discussion on risk. Others may be in denial or be ashamed of their oral hygiene, alcohol consumption or drug use and expect judgement. Patients may omit to give these details as they believe that dental professionals have access to the same systems as GPs.
Including such topics in the medical history form allows for their regular review and Faculty of General Dental Practice guidelines suggest medical history forms be completed at every recall and verbally before any invasive treatment.3 It is important to revisit the forms as patients' circumstances, and thus risk, may change.
Patients may question why dental professionals would require specific information about their lifestyle habits and choices and be resistant to discussing these topics. It can be useful to explain to patients, as you work through these topics on the medical history, why the questions are relevant to dentistry and their oral care.5 It is important to link these topics to any specific clinical findings, effects or barriers to treatment and why the information helps develop a tailored oral health plan. It is also essential to know where to direct patients should high risk be identified and the patient require further support.
Brief interventions
Brief interventions are opportunistic discussions on sensitive lifestyle choices that should take 5–10 minutes. They are opportunities to assess and increase a patient's motivation or readiness to change, educate, encourage and refer.6 They are ideally suited to the dental environment. Brief interventions arise against a background of motivational interviewing, which was developed to enable behaviour change in addiction.7 Characteristics of the ideal brief intervention are set out in Table 1.
Opportunistic advice: intended to trigger quit attempts, not to support
Through discussion, negotiation/encouragement
Should take only 5–10 minutes
Passing on simple, relevant, factual information when the opportunity arises
Assessing the person's readiness to quit
Making the person aware of pharmacotherapy and/or behavioural support that is available locally
Provision of self-help material
Referral to more intensive support from a specialist service
A non-judgemental, empathetic approach must be taken. Ask patients if they feel ready to make a change. If they do not want to engage, accept this and stay neutral and non-argumentative. Advise them that it is your professional responsibility to bring up these subjects and that you will revisit them on their next visit. If they express an interest in making a change, find out their motivation to do so and highlight differences between their current behaviour and where they would like to be. Resist the urge to tell patients what to do as this has paradoxically been shown to reinforce current behaviour.8 Support their wish to change with advice on planning the change in behaviour and referral if necessary to services and support groups. In short, raise awareness, assess motives and support change.
Giving oral health instructions
Providing oral health instruction (OHI) should be where dental professionals are most at ease. However, conversations can be uncomfortable, and the authors have found resistance can occur from patients who find OHI demeaning because it is a skill that is taught in infancy. Results of a recent study indicated that, according to a UK general population online survey (n=1405), more than one-quarter of patients would be unwilling to pay for personalized oral hygiene advice and, of these, just under 10% felt they had no need for this.9 Thus, patients do not always value oral hygiene advice, even though it is essential to their oral care. For those who struggle to provide verbal instruction, evidence supports computer-assisted delivered oral hygiene advice.10 However, the more personalized any such information is, the more likely patients are to follow the advice.11
The Scottish Dental Clinical Effectiveness Programme (SDCEP) guidance includes a framework to provide OHI (Table 2) and is based on the acronym TIPPS: talk, instruct, practice, plan and support.
TALK with the patient about the causes of periodontal disease and discuss any barriers to effective plaque removal
INSTRUCT the patient on the best ways to perform effective plaque removal
Ask the patient to PRACTISE cleaning his/her teeth and to use interdental cleaning aids while in the dental surgery
Put in place a PLAN that specifies how the patient will incorporate oral hygiene into daily life
Provide SUPPORT to the patient by following up at subsequent visits
The TIPPS model not only provides a structured approach to oral hygiene but also supports behavioural change. The model has helpful supporting visual aids to accompany discussion, which are on the SDCEP website.12
Smoking
Patients' smoking history should be known and documented in their notes because smoking has a significant impact on general and oral health.13
Guidance exists on the role of the healthcare worker in relation to smoking.14 This includes the four points outlined below, which can only be achieved through conversation.
Responsibility to educate
Smoking is the number one risk factor for lung cancer and significantly raises the risk of many other cancers including oral cancer. It increases the risk of chronic obstructive pulmonary disease, vision loss, rheumatoid arthritis, heart disease and diabetes, among other conditions. Although the risks of smoking to general health are well known, the risk for oral diseases is less so: 42% of periodontal disease is due to smoking.15 Additionally, smokers have a worse prognosis for periodontal disease, which is combined with a poorer response to treatment.
Additionally, healthcare workers also have a responsibility to advise on the dangers of second-hand smoke.14
Be sensitive to patients
Nicotine, the drug in tobacco, is highly addictive and causes dependency – the most common dependency in the world. Conversations regarding smoking need to be carried out sympathetically and clinical staff must be aware of underlying cultural and social aspects. Difficulties around withdrawal will also affect a patient's desire and ability to stop smoking.
Initiate smoking cessation events
National Institute for Health and Care Excellence guidelines state, ‘At every opportunity ask people if they smoke… and advise them to stop smoking in a way that is sensitive to their preferences and needs’.14 As part of a patient's periodontal screening, SDCEP guidance states: ‘All health and health-related staff should raise the issue of stopping smoking in their day-to-day work with patients and clients and, where appropriate, refer them on to local services to help them stop.’16
Offer help, support, guidance and encouragement
A number of stop-smoking resources are available but may be specific to a patient's location. Smokeline (0800 84 84 84) is a free, confidential helpline staffed by trained advisers who give guidance to those who want to stop smoking and details of how to access local specialist services. Additionally, the NHS Better Health website (www.nhs.uk/better-health/quit-smoking/) is an online resource for smokers who are contemplating giving up.
The five As (Table 3) is an easy to remember structure to approach smoking. The ‘ask’ can be included on the medical history or asked directly. This approach can be considered a brief intervention.17
Ask
About smoking habit
Advise
The smoker to stop
Assess
Motivation
Assist
All smokers who want to stop
Arrange
Follow up, record on notes, relapses
Review progress and support success and failures
Alcohol
Research has shown that the three lifestyle habits of smoking, alcohol consumption and recreational drug use go hand in hand, with alcohol abuse playing a mediating role in the interrelationship.18 All can be highly addictive. Li et al found that alcohol disorders are often comorbid with depressive symptoms, which may then impact personal care and appointment attendance.19 Alcohol consumption should be included in the medical history questionnaire, although the practitioner must be aware that under-reporting of alcohol consumption is common, with one study finding 40% of under-reporting in what patients say they drink in a week.20
Alcohol is a risk factor for cancer, including oral cancer.21 The risk is around 2% for moderate drinkers and 5% for heavy drinkers, with significant synergistic effects if a person both smokes and drinks alcohol.22
In the case of excessive alcohol consumption, a 2018 Cochrane review suggested that brief interventions can be effective and reduce alcohol consumption in hazardous or harmful drinkers.23 One brief intervention for alcohol use consists of IDENTIFY and ADVISE or REFER: identify the amount of alcohol consumed; discuss advised limits; and refer if appropriate.24
Identify
A useful brief screening tool is the alcohol use disorders identification test – consumption (AUDIT C). This is a shortened version of the full alcohol use disorders identification test (AUDIT) consisting of the consumption questions only and is available at: www.gov.uk/government/publications/alcohol-use-screening-tests
It consists of three questions:
How often do you have a drink containing alcohol?
How many units do you drink on a typical day when you are drinking?
How often have you had 6 or more units if female, or 8 more if male, on a single occasion in the last year?
Risk
Risk is scored on a scale of 0–12, with each of the three questions having a maximum score of 4. A score of 0–4 indicates a low risk for harm to health. A score of 5–10 suggests the patient may be drinking at a level that could put their health at risk. A score of 11 or 12 suggests the possibility of alcohol dependency.
Many patients are unaware of what constitutes a unit of alcohol or underestimate how much a unit is. The AUDIT C questionnaire or the alcohol structured advice tool leaflet (available at https://app.box.com/v/CQUIN-structured-advice-tool) include pictures of different drinks to show patients how much a unit is.25
To keep health risks from alcohol to a low level:
Men and women are advised that it is safest not to drink more than 14 units a week on a regular basis;
If as much as 14 units a week is consumed, it is best for it to be spread evenly over 3 or more days;
Have several drink-free days each week and avoid binge drinking (consuming large amounts of alcohol in one session).
It is important to address how and why someone drinks. The ‘how’ is identifying the patient's pattern of alcohol consumption. For example, binge drinking alcohol is classified as more than 6 units for a woman and over 8 units for a man in a single session. The ‘why’ is identifying triggers for drinking. These can be emotions or situations. If someone can recognize when they are at risk from drinking to excess, they have potential to make a change.
Simple advice on how to cut down can be given. For example, in highlighting risks of single-session drinking, NHS England advises to limit how much drink is consumed in one session by:
Drinking more slowly;
Drinking with food;
Alternating alcoholic drinks with water or non-alcoholic drinks.
Alcohol scripts are available to start discussion with patients. Examples are given in Table 4.
General introduction
‘Thank you XXX (Mr/Ms Smith) for completing this form. We're talking to everyone about their alcohol use. Most of us think of drinking as a pretty harmless activity, but all alcohol use carries a level of risk’
AUDIT C score 0–4
‘Your score is X (0–4). This indicates that you are drinking at lower-risk levels and your alcohol use is unlikely to be adding significantly to any health problems’
AUDIT C score 5–10
‘Your score is X (5–10). This means you may be drinking more than is healthy for you and adding to your risk of future health problems such as hypertension, depression and some cancers’
‘I'd encourage you to cut back, even just a little, by drinking less on the days you do drink and/or having more days when you don't drink at all. The chief medical officer has recently issued guidance that, to keep the risk low, both men and women should not regularly drink more than 14 units a week – that's no more than about 7 pints of ordinary beer or 7 regular glasses of wine, spread out through the week’
‘Please take this form* home with you. It contains more information including tips for cutting down, websites and contact numbers if you want to discuss this further’
‘Any questions?’
AUDIT C score 11–12
‘Your score is X (11–12). This means you may be drinking in quite a problematic way that may well be impacting on your health already and is adding to your risk of future health problems. I'd like to refer you to someone who can talk to you in a bit more detail about how your alcohol use might be affecting your health and wellbeing. Would that be OK?’
(Put patient in contact with an alcohol specialist in the hospital or in the community)
‘Please take this form* home with you. It contains more information including websites and contact numbers’
‘Any questions?’
Refer
Patients who are at higher risk can be directed to their GP. There are leaflets that can be printed out for patients such as the structured advice tool: https://app.box.com/v/CQUIN-structured-advice-tool.
This also highlights the NHS drink-free days app at www.nhs.uk/oneyou/apps. This link now forwards to Kickstart your health at: www.nhs.uk/better-health, which has a link to Drink Less at www.nhs.uk/better-health/drink-less.
Patients can also call the national helpline, Drinkline on 0300 123 1110 (weekdays 9am–8pm, weekends 11am–4pm).
Recreational drugs
Recreational drug use is widespread, with the World Health Organization stating that 2.5% of the world's population consume cannabis ,and just under 10% of adults in the UK took an illicit drug in 2023.27,28 Recreational drugs in the UK include, but are not limited to, cannabis, cocaine, MDMA (3,4-methylenedioxymethampheyamine), nitrous oxide and opiates.29
Discussing recreational drug use can be challenging owing to its illegal nature, but this must be attempted because it has implications regarding consent, as well as oral, systemic and drug interactions. Ideally, this would be initially asked about on the medical history form to normalize the question and start a conversation. One of the present authors found that making this enquiry normally led to patients being more open about their HIV or hepatitis C status, enabled discussion with the patient regarding where they were on their methadone journey and allowed the provision of specific, tailored preventive advice. Patients taking recreational drugs can be given brief advice about the general health and dental effects of drug taking. This can include:
Guidance about alcohol and drug misuse can be found at: www.gov.uk/government/collections/alcohol-and-drug-misuse-prevention-and-treatment-guidance. The cannabis health check tool from the UK Health Security Agency can be found under the section ‘Drug and alcohol screening and treatment tools’. This is a useful resource that can be printed off.
The NHS encourages patients to be directed to their GP as their first point of contact.
FRANK (www.talktofrank.com/) is an excellent website to which patients can be directed. There is a 24-hour, 7-days-a-week phone number, text, live chat and email contact;
For those who prefer a self-help approach, UK Narcotics Anonymous has groups throughout the country accessed via their website.
Diet
Conversations about a patient's diet can form an essential part of their oral care. Diet can have a significant impact on a patient's caries experience, tooth wear and weight.
Well-established questions regarding diet affecting caries risk are well documented. Supplemental diet diaries can provide an informative framework for such conversations.
Questioning a patient to elicit information that would suggest or confirm tooth wear can be sensitive as the authors have found that such patients often consider that they have a healthy diet. The WATCH strategy offers a framework of questions to find the aetiology and from there, a means of prevention without being judgemental about lifestyles (Table 5).31Obesity is a growing problem in the UK.32 Implications for general health are wide ranging and well documented, but there are often effects on dental health and care too.
Water
Do you drink enough water?
Drink 1.5 litres of pure water per day
Drink two litres, 2 hours before a game or one litre 1 hour before a game
Acids
Do you drink excess soft or sports drinks containing ascorbic, citric or phosphoric acid?
Avoid acid drinks when dehydrated in sports, work or when drugs shut off salivary protection
Taste
Do you taste enough fresh fruit daily?
Eat a piece of fruit with every breakfast to stimulate saliva
Calcium
Are you getting enough calcium in your diet?
Milk, cheese and yoghurt contain calcium and protect teeth against acids
Health
Do you have a healthy lifestyle and diet?
Healthy lifestyles can be dehydrating
Do you have a health problem?
Excess alcohol is dehydrating and causes gastric acid reflux
Drugs given for asthma, depression, hypertension etc shut off saliva
Obesity is linked to type 2 diabetes, which is a risk factor for periodontal disease and susceptibility to oral disease. Increased weight can result in acid reflux and enamel erosion. Additionally, many dental chairs in the UK are manufactured to support patients of a weight up to 140 kg depending on the manufacturer.
Enquiring about a patient's weight can be carried out discreetly while completing a medical history form. A dentist is obliged to provide advice. The Eatwell Guide is a government document to encourage healthy eating and provides simple messages that dentists can convey to their patients (Table 6).33
Eat at least five portions of a variety of fruit and vegetables every day
Base meals on potatoes, bread, rice, pasta and other starchy carbohydrates, choosing wholegrain versions where possible
Have some dairy or dairy alternatives (such as soy drinks); choose lower fat and lower sugar options
Eat some beans, pulses, fish, eggs, meat and other proteins (including two portions of fish every week, one of which should be oily)
Choose unsaturated oils and spreads and eat in small amounts
Drink 6–8 cups or glasses of fluid a day
If consuming foods and drinks high in fat, salt or sugar, have these less often and in small amounts
Anxiety
Almost half of the adults in the UK have some form of fear of the dentist, with 12% experiencing extreme dental anxiety.34 Non-attenders are unlikely to discuss their fears and phobias, thus figures are likely to be higher.35
Management of anxiety and effective pain control are essential components of providing dental treatment. Patients expect it as part of their care, and the GDC states that management of anxiety by dentists is a requirement in the delivery of dental care.2
Expressions of fear and dislike of the dentist are commonplace in a dental practice, but the ability of patients to cope with treatment can be wide ranging, with patients often masking real phobia. Documentation of a patient's anxiety levels (and treatment preferences) should be included in their clinical records.36
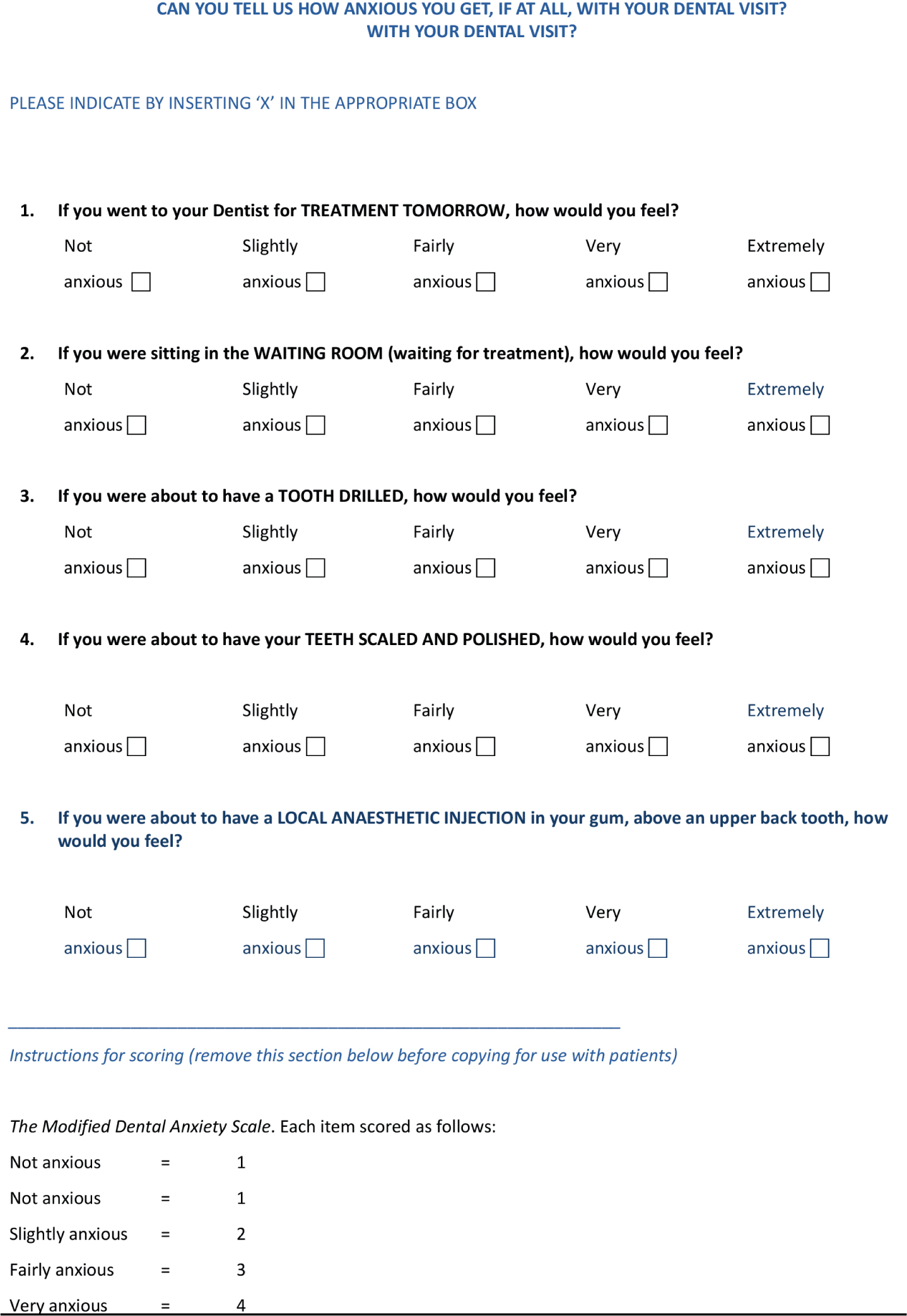
Questionnaires have been developed to assess the level of anxiety. They include specific questions that the patient puts a grade against. The total number at the end gives an indication of where a patients anxiety level lies and may indicate whether appropriate referral is indicated. These instruments include the SDCEP General Anxiety Questionnaire (Figure 1) and the Modified Dental Anxiety Scale (Figure 2).36,37
For patients who can be managed in primary care, other questionnaires can help pinpoint techniques and open conversations about suitable behavioural management techniques.
General strategies for communication
Stein et al conducted a literature search for communication strategies with older patients in the dental setting, a group that, because of the effects of age on cognitive, physical and psychological changes, may bring communication challenges.38 They found the strategies in Table 7 were effective. These strategies can be applied to any patient group for communicative success, and using the information provided in this article as a base to begin for the more sensitive but essential conversations.
Prepare an agenda before the appointment
Exhibit warm, nonverbal behaviour
Listen attentively
Ask open-ended questions
Use simple language, presenting one point at a time
Provide patients with written instructions
Conclusion
Conversations around lifestyle choices need to be made in the dental setting. Initiating such sensitive conversations can be challenging, particularly given the time available to the busy practitioner.
The strategies suggested above can be drawn upon for patients as indicated, often following on from responses contained within the medical history form. Having the resources available can develop conversations. Additionally, having such strategies to hand should make conversations efficient, as dental professionals often work under significant time constraints and and are not remunerated for implementing such strategies.