Dentistry is a profession in which both clinicians and patients hope that mistakes never occur. Unfortunately, mistakes are inevitable in our profession, whether the outcomes are inconsequential or not. Adverse incidents that result in harm to a patient can have long-term repercussions for both the patient and the clinician involved. For clinicians, this could involve litigation from the patient, as well as reprimand from healthcare regulators and colleagues. In addition, the negative psychological implications associated with causing harm or detriment to a patient under our care should not be underestimated. Despite this, there is a risk that our profession focuses on a blame culture when errors occur in our clinical practice, rather than understanding the role of human factors in contributing to such events. This two-part article explores the role of human factors in dentistry, why things go wrong, and how we can learn from mistakes within the profession, providing worked case examples and highlighting 2020 national guidance on human factors in dentistry.
CPD/Clinical Relevance: There may be merit in the dental profession moving away from the blame culture when things go wrong..
Article
The study of ‘human factors’ involves understanding that errors do not happen by accident. Rather, it is the appreciation that a multitude of factors have contributed to that particular outcome. It is imperative that our profession acknowledges and recognizes the role of human factors in our daily practice, and that we use this understanding of human factors to support clinicians when inevitable adverse incidents occur in our careers.
During undergraduate dental school, a great deal of the curriculum focuses on fundamental oral conditions, such as plaque-related diseases, and the management of these conditions. However, the concept of ‘human factors in dentistry’ is also a core topic of relevance, that in the author's opinion is not always given the necessary importance, both at an undergraduate and a postgraduate training level.
Dental Protection and the Medical Protection Society both report that 80% of litigation from patients is due to human factors. Yet, many dentists are not even aware of what this term is, let alone what it means. How can dentists reduce the risk of errors if there is a lack of awareness of this issue in the first instance? As an undergraduate dental student, open discussion about ‘clinical errors’ or ‘mistakes’ that are likely to occur once dentists become qualified are seldom discussed. During the author's training, the topic of human factors in dentistry was not taught as an undergraduate lecture or a workshop seminar in any capacity. The premise that a qualified dentist could make the unfortunate mistake of extracting the wrong tooth, separate an endodontic file during root canal treatment or cause a lip laceration during a crown preparation would be inconceivable to both the general public, as well as most unqualified dentists. However, it would be naïve among our profession to believe that a BDS degree comes with a ‘no-mistakes’ insurance clause. Unfortunately, in all aspects of healthcare, mistakes are very much a part of the profession. In hospital medicine, monthly debrief meetings are held to openly discuss mistakes in ‘morbidity and mortality meetings’ to allow clinicians the opportunity to improve outcomes and reduce errors. Historically, the field of dentistry has not adopted the same attitudes towards mistakes as the medical profession. Thus far, our profession has failed to regard the learning opportunities, with open discussion of mistakes, with the same level of importance, and often our errors are kept quiet for fear of reprimand from our healthcare regulators, such as the General Dental Council, as well as from our colleagues and patients. That is not to say that clinical incompetence in dentistry is something that should be accepted or condoned in any way. What should be addressed is how mistakes are handled within dentistry, both individually, and as a profession. Instead of blame and shame, mistakes should be openly discussed among colleagues so that lessons can be learned, not only from what happened, but, more importantly, to understand why it happened so that it can be prevented from happening again. This learning process should be of greater importance than the previous rationale within the NHS of blaming and fault finding of the clinician. The focus should be driven towards raising awareness of one's own behaviours and interactions with others within the working environment for the benefit of patients, the team and the clinician's own personal wellbeing. However, until the stigma of clinical mistakes in dentistry being equated to clinical incompetence is stopped, the profession will continue with the fallacy that we are acting in our patient's best interests by hiding our mistakes.
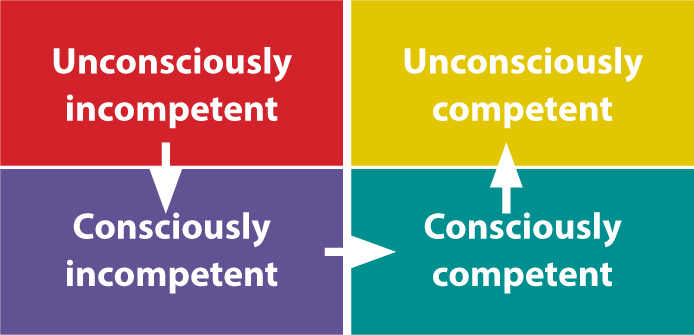
In dentistry, there is no such thing as ‘no risk’. Dentists are humans who provide care for other humans. They are not infallible and are capable of making errors irrespective of how many years they have been practising. From the ‘unconscious incompetence’ of an undergraduate in training to the ‘unconscious competence’ of the qualified and experienced dentist, the same clinical error can occur, although the reasons for the error may be very different (Figure 1). Clinical knowledge and skills in dentistry can be taught, practised and executed hundreds of times to perfection, but that does not mean that an error will not occur with the next patient having that procedure in the dental chair.
Figure 1. The progression of clinical knowledge and skills in dentistry from undergraduate training to an experienced dental clinician over many years.
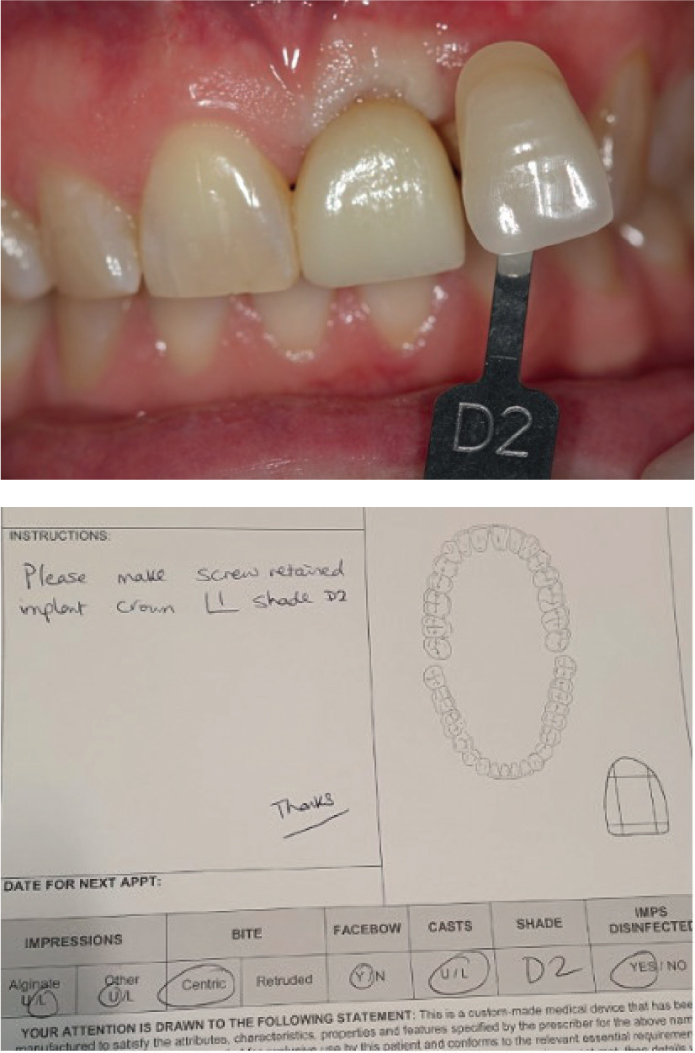
In the author's opinion, all clinicians have made, and will continue to make, mistakes throughout their careers. Sometimes, they are small and inconsequential errors, such as an incorrectly prescribed laboratory docket (Figure 2). At other times, the mistakes are more substantive, such as an extraction from the wrong site, and there is a need to reflect on why such mistakes have occurred. Dentists will often make a mental note to avoid making the same mistake again or at the very least, to minimize the effects of the mistakes causing harm. However, there needs to be a culture shift in dentistry away from blame and fault finding, and instead a move towards learning lessons and mitigating adverse outcomes to improve the profession and outcomes for our patients.
Figure 2. (a) Clinical photograph showing poor shade match for implant crown UL1 owing to poor shade taking and inadequate information on laboratory docket for technician. (b) Laboratory docket lacking information regarding shade. Because the laboratory work does not match with the clinician requirements, the implant crown needs to be re-made, resulting in additional costs and time spent in the chair for the patient, clinician and laboratory staff.
National guidelines for human factors
In 2018, the National Advisory Board for Human Factors in Dentistry (NABHFD) was set up at the suggestion of the General Dental Council after registrants felt that patient safety and the role of human factors should be highlighted to the dental team. In June 2020, the NABHFD1 published a position paper highlighting the importance of multiple ‘human factors’ that influence the quality and efficiency of the dental care provided in the UK, and a novel approach to promote learning from incidents in an open, transparent manner. This move was fundamental in moving dentistry in the right direction, shifting away from the outdated blame culture and under-reporting of errors for fear of reprimand from healthcare regulators.
What are ‘human factors’?
One definition of human factors (HF) in healthcare from NHS England is: ‘Enhancing clinical performance through an understanding of the effects of teamwork, tasks, equipment, workspace, culture and organization on human behaviour and abilities and application of that knowledge in clinical settings.’2
What does this definition mean in real terms? Those working within the NHS are acutely aware that every area of the NHS is under constant strain on a daily basis to balance the provision of high-quality patient-centred care against financial and operational challenges. Issues of inadequate staffing levels and equipment shortages are a constant phenomenon within the NHS (Table 1). These challenges can compromise the quality of care provided, and potentially compromise the outcomes of care to our patients. Often, clinicians and support staff are left to compensate for the inadequacies of these shortcomings. For example, many staff will work unpaid overtime to complete the unfinished tasks caused by staff shortages. Rather than complain about the things that are lacking within the working environment, the sense of duty of those working within the NHS means that the job will be done, and there is an acceptance of the shortcomings brought about by NHS underfunding. Since the inception of the NHS in 1948 by Aneurin Bevan, the NHS has run on the ‘good will’ of staff to do whatever is needed to ensure patients are seen and given the best care possible. However, with the ever-increasing pressures of medical litigation for NHS staff, and the historical ‘blame culture’ within NHS organizations, staff may feel less compelled to continue this good will in the future. Furthermore, with advances in technology, most errors within healthcare are now due to human factors as opposed to structural or operational inadequacies.
Table 1. Current issues faced by NHS dentists.
Staff shortages
Equipment shortages/lack of equipment
Lack of time
Staff burnout/overworked/underpaid
Financial restraints in UDA fee structure
Where did the concept ‘human factors’ come from?
In 2005, a 37-year-old mother was due to have a routine surgery in a private hospital within the UK. Unfortunately, catastrophic brain damage resulted, and she died. Her husband, who was an airline pilot, did not blame the NHS. Instead, he used the events leading to his wife's death as a catalyst for the urgent need for an open and transparent independent investigation to find the root cause of what had led to his wife's death. Using his years of experience within the aviation industry, and the need to identify the HF and reasons behind why this outcome had occurred, he brought about a change in the way the NHS handled adverse outcomes to ensure that mistakes could be learned from and prevented in the future. There has been a greater uptake into the philosophy of human factors and the interaction with outcomes in medicine. The dental profession also needs to look at how mistakes are handled.
In the aviation industry, through analysing HF, risks are mitigated or minimized, improving safety. Within dentistry, there is limited awareness of the concept of HF. In both aviation and dentistry, mistakes do happen, often unexpectedly, and the consequences can be significant.
In 1993, Gordon Dupont, President of the Pacific Aircraft Maintenance Engineers Association created a list of the ‘Dirty dozen errors in maintenance’, which outlined the 12 most common human error conditions/pre-conditions that can lead to accidents, or incidents, and result in people making mistakes.3,4 This dirty dozen list is now used in HF training worldwide, and is applicable to dentistry (Table 2).
Table 2. Gordon Dupont's ‘Dirty Dozen list’.
Dirty dozen list
Issue
How to improve
Lack of communication
Only 30% of verbal communication is remembered by patients – usually what is said at the start and end of a conversation
Say the most important information to a patient at the start and end of appointments
Write a letter to the patient after your first appointment outlining the treatment plan, risks, benefits, costs, time expected, and alternative treatment options to gain informed consent
Repeat important statements to the patients, and ask them to repeat information to improve memory
Distraction
Not paying full attention to the task at hand
Minimize sources of distraction within the working environment
Avoid interruptions from other people entering the room during procedures
Lack of resources
Short staffed, equipment lacking, inadequate time to complete tasks
Audit your current resources. Discuss with line managers if there are equipment shortages/frequent equipment breakages/inadequate nursing staffing levels
Stress
Physical, chemical or emotional factors
Support staff who are under stress, offer counselling, offer short breaks when needed, seek NHS help for stress management
Complacency
Becoming over-confident when repeating a procedure multiple times
Be alert during treatment. Expect to find something new each time
Lack of teamwork
Failure to work with others to fully use everyone's skills
Debrief between the dentist and the dental nurse at the start of the morning and afternoon clinical session to highlight any patients/procedures that will require special attention.
Have a short debrief before each appointment to ensure everyone understands and agrees what needs to be done and how to do it.
Also, discuss any potential patients who require more support during appointments.
Delegate appropriately to team members if others can help support your clinical workload.
Pressure
Real or perceived pressure on staff
Communicate with all staff members
Ask for help when needed
Put safety of patients and staff first
Lack of awareness
Failure to recognize what is happening in a situation and anticipate the outcome
Be prepared for clinical tasks, and have good background knowledge of the procedure and equipment beforehand
Speak with senior colleagues on how to problem-solve interpersonal issues or clinical concerns that you may have
Attend courses on interpersonal skills
Lack of knowledge
Inadequate training, lack of experience
Ask for advice, mentoring, support from a senior colleague in the workplace or another dental practice
Use phantom head plastic teeth to practise procedures
Attend courses, up-skill training
Read dental journals/textbooks
Fatigue
Physical or mental exhaustion results in poorer work performance
Look for symptoms of fatigue in yourself and others – take scheduled breaks at regular intervals
Lack of assertiveness
Failure to voice concerns or document concerns about others
Have an open and transparent approach to raising concerns within the working environment
Regular team meetings to discuss issues and raise concerns
Appraisals annually to raise issues with line manager in a positive, productive way
Norms
Code of conduct not followed, e.g. safety protocols, negative attitudes within the workplace
Encourage a positive working environment
In 2008, Dr Atul Gawande highlighted the importance of safety checklists during general anaesthetic operations to improve communication among team members and reduce morbidity and mortality outcomes used from the World Health Organization surgical checklist.5 There are over 250 factors that contribute to causing an error, so one might assume that by identifying some of these factors, one could minimize the risk of errors. Unfortunately, introducing checklists alone does not mitigate for all human factors leading to adverse incidents.
In the aviation industry, Standard Operating Procedures (SOPs) have existed for many years to minimize the chances of human error causing fatal errors. In dentistry, we are starting to adopt SOPs, for example, when carrying out procedures such as extractions, implant placements and surgical procedures. With the COVID-19 pandemic, SOPs were created for all facets of dentistry and they do work to a certain degree to reduce operational risks. However, unlike the aviation industry, healthcare cannot be run in the same manner owing to the variability and reduced predictability compared to aeroplanes and air traffic controllers. Dentistry has the added dimension of dealing with patients who present with their own values, beliefs and HFs that must be respected when providing healthcare. Therefore, while SOPs have some value in reducing the chances of errors in dentistry, for example by reminding clinicians to check an immediate denture has the correct tooth replacement before carrying out the extraction, the addition of SOP paperwork as a tick box exercise has limited added value and may in fact create additional sources of stress, time pressures and fatigue to already busy clinicians. Instead of completing more paperwork, time may be better spent communicating more effectively with patients and nurses prior to commencing irreversible procedures to improve informed consent, ensure procedures are carried out as intended and give clinicians adequate time to complete treatment.
Why are human factors important?
Readers will be aware of the Mid Staffordshire Hospital scandal between 2005 and 2009 that led to the publication of the Francis Report in 2013.6 The hospital was found to have a fundamental flaw in the way that concerns were raised, and that there was a lack of openness, transparency and candour. Since then, there has been a greater focus in all areas of the NHS to promote the ethos that all staff, irrespective of their job role, have the freedom to speak up when there is a concern. Following the Mid Staffordshire inquiry, the National Quality Board (NQB) set up a concordat of multiple national organizations that are responsible for ensuring quality within the NHS, along with patient representatives and experts, with the principle aim of ensuring that the NHS does the right treatment for the right patient at the right time.2
Across the NHS, it is quoted that one in every 10 patients is harmed, which means that 90% of the time, we get things right.7 However, the dental profession rarely studies how and why things go right. It is the understanding of this 90% of things we get right that will help us to minimize harm. Unfortunately, just as dentistry is about treating existing dental disease and not about promoting oral health, we spend the majority of time investigating when things go wrong and not investigating when things go right to understand how we can replicate those circumstances. It is not a coincidence that dentists have a better working day when they are working with an experienced, competent and confident dental nurse compared to an inexperienced nurse. This relationship is fundamental in outcomes of patient care, yet it is not something routinely discussed or researched.
Conclusion
In summary, understanding HFs is important because it works on the premise that by understanding human limitations, the chances of causing an error can be minimized in healthcare, and that a cultural change can occur by learning from mistakes, putting systems in place to mitigate against repeating mistakes. Historically, the NHS has tended to adopt a blame culture when things go wrong. This has led staff to often feel ashamed to raise issues or concerns, preventing growth and learning from mistakes. By openly discussing mistakes and human factors, our profession can use these errors as opportunities for individual personal growth and growth among the dental profession for the best interests of ourselves, our patients and our profession overall.