Drake RL, McBride JM, Pawlina W An update on the status of anatomical sciences education in United States medical schools. Anat Sci Educ. 2014; 7:321-325 https://doi.org/10.1002/ase.1468
Saltarelli AJ, Roseth CJ, Saltarelli WA Human cadavers Vs. multimedia simulation: a study of student learning in anatomy. Anat Sci Educ. 2014; 7:331-339 https://doi.org/10.1002/ase.1429
Krähenbìhl SM, Čvančara P, Stieglitz T Return of the cadaver: key role of anatomic dissection for plastic surgery resident training. Medicine (Baltimore). 2017; 96 https://doi.org/10.1097/MD.0000000000007528
Iwanaga J, Loukas M, Dumont AS, Tubbs RS A review of anatomy education during and after the COVID-19 pandemic: revisiting traditional and modern methods to achieve future innovation. Clin Anat. 2021; 34:108-114 https://doi.org/10.1002/ca.23655
Eve EJ, Koo S, Alshihri AA Performance of dental students versus prosthodontics residents on a 3D immersive haptic simulator. J Dent Educ. 2014; 78:630-637
Al-Saud LM, Mushtaq F, Allsop MJ Feedback and motor skill acquisition using a haptic dental simulator. Eur J Dent Educ. 2017; 21:240-247 https://doi.org/10.1111/eje.12214
Sytek L, Inglehart MR, Ramaswamy V Comparisons of orthodontic residents' performance and attitudes using 2D, 3D, and virtual reality surgical simulation methods. J Dent Educ. 2021; 85:1415-1426 https://doi.org/10.1002/jdd.12598
Mischkowski RA, Zinser MJ, Kubler AC Application of an augmented reality tool for maxillary positioning in orthognathic surgery. a feasibility study. J Craniomaxillofac Surg. 2006; 34:478-483 https://doi.org/10.1016/j.jcms.2006.07.862
Wagner A, Rasse M, Millesi W, Ewers R Virtual reality for orthognathic surgery: the augmented reality environment concept. J Oral Maxillofac Surg. 1997; 55:456-462 https://doi.org/10.1016/s0278-2391(97)90689-3
Aditya PVA, Prasad MG, Nagaradhakrishna A Comparison of effectiveness of three distraction techniques to allay dental anxiety during inferior alveolar nerve block in children: a randomized controlled clinical trial. Heliyon. 2021; 7 https://doi.org/10.1016/j.heliyon.2021.e08092
Baus O, Bouchard S Moving from virtual reality exposure-based therapy to augmented reality exposure-based therapy: a review. Front Hum Neurosci. 2014; 8 https://doi.org/10.3389/fnhum.2014.00112
Raghav K, Van Wijk AJ, Abdullah F Efficacy of virtual reality exposure therapy for treatment of dental phobia: a randomized control trial. BMC Oral Health. 2016; 16 https://doi.org/10.1186/s12903-016-0186-z
K.l.c A, Brown A, Aras I Using virtual technology for fear of medical procedures: a systematic review of the effectiveness of virtual reality-based interventions. Ann Behav Med. 2021; 55:1062-1079 https://doi.org/10.1093/abm/kaab016
Cunningham A, McPolin O, Fallis R A systematic review of the use of virtual reality or dental smartphone applications as interventions for management of paediatric dental anxiety. BMC Oral Health. 2021; 21 https://doi.org/10.1186/s12903-021-01602-3
Yamaguchi S, Ohtani T, Ono S Intuitive surgical navigation system for dental implantology by using retinal imaging display. In: Turkyilmaz I Rijeka, Croatia: InTech; 2011
Kati D, Spengler P, Bodenstedt S A system for context-aware intraoperative augmented reality in dental implant surgery. Int J Comput Assist Radiol Surg. 2015; 10:101-108 https://doi.org/10.1007/s11548-014-1005-0
Lin YK, Yau HT, Wang IC A novel dental implant guided surgery based on integration of surgical template and augmented reality. Clin Implant Dent Relat Res. 2015; 17:543-553 https://doi.org/10.1111/cid.12119
Gardiner S, Hartzell TL Telemedicine and plastic surgery: a review of its applications, limitations and legal pitfalls. J Plast Reconstr Aesthet Surg. 2012; 65:e47-53 https://doi.org/10.1016/j.bjps.2011.11.048
Petcu R, Kimble C, Ologeanu-Taddei R Assessing patient's perception of oral teleconsultation. Int J Technol Assess Health Care. 2017; 33:147-154 https://doi.org/10.1017/S0266462317000319
Bruellmann DD, Tjaden H, Schwanecke U, Barth P An optimized video system for augmented reality in endodontics: a feasibility study. Clin Oral Investig. 2013; 17:441-448 https://doi.org/10.1007/s00784-012-0718-0
Aichert A, Wein W, Ladikos A Imagebased tracking of the teeth for orthodontic augmented reality. Medical Image Computing and Computer-Assisted Intervention. MICCAI 2012. Lecture Notes in Computer Science. 2012; 7511 https://doi.org/10.1007/978-3-642-33418-4_74
Xue C, Xu H, Guo Y Accurate bracket placement using a computer-aided design and computer-aided manufacturing-guided bonding device: An in vivo study. Am J Orthod Dentofacial Orthop. 2020; 157:269-277 https://doi.org/10.1016/j.ajodo.2019.03.022
Barsom EZ, Graafland M, Schijven MP Systematic review on the effectiveness of augmented reality applications in medical training. Surg Endosc. 2016; 30:4174-4183 https://doi.org/10.1007/s00464-016-4800-6
This report introduces the reader to the concepts and applications of augmented and virtual reality in dentistry. Virtual reality (VR) is the computer-generated three-dimensional simulation of a virtual environment accessed through a headset. Augmented reality (AR) is the superimposition of computer-generated imagery or graphics onto the real world, accessed through phones, tablets and headsets. The technology has advanced in recent years with early applications to the medical field revolving around anxiety management, teaching and surgical planning. Uses for surgical orthognathic and other restorative interventions are also in an early phase of development and adoption.
CPD/Clinical Relevance:
VR and AR have promising applications, but more research must be carried out to determine the technology's validity in dentistry.
Article
Before considering its application and history, virtual reality (VR) must be defined. VR is a computer-generated three-dimensional simulation of an environment that immerses the user in an artificial surrounding. This environment is accessed with electronic equipment such as a headset.1 Augmented reality (AR) differs slightly because a computer-generated image is superimposed onto the real world, usually through devices like phones and tablets.2 This enhances the perception of the natural world by providing overlays such as images, objects and information.
The history of VR
The earliest known VR came from panoramic paintings in the 19th century, such as paintings by Franz Roubaud of the battle of Borodino, which depicts the French and Russian forces at Borodino (Figure 1). Another example includes the Racławice panorama in Poland, which is 114 m long and 15 m high. This 360-degree canvas attempts to immerse the viewer in the scenery, much like the definitions mentioned above of virtual reality.
Figure 1. The Battle of Borodino, 1812.3
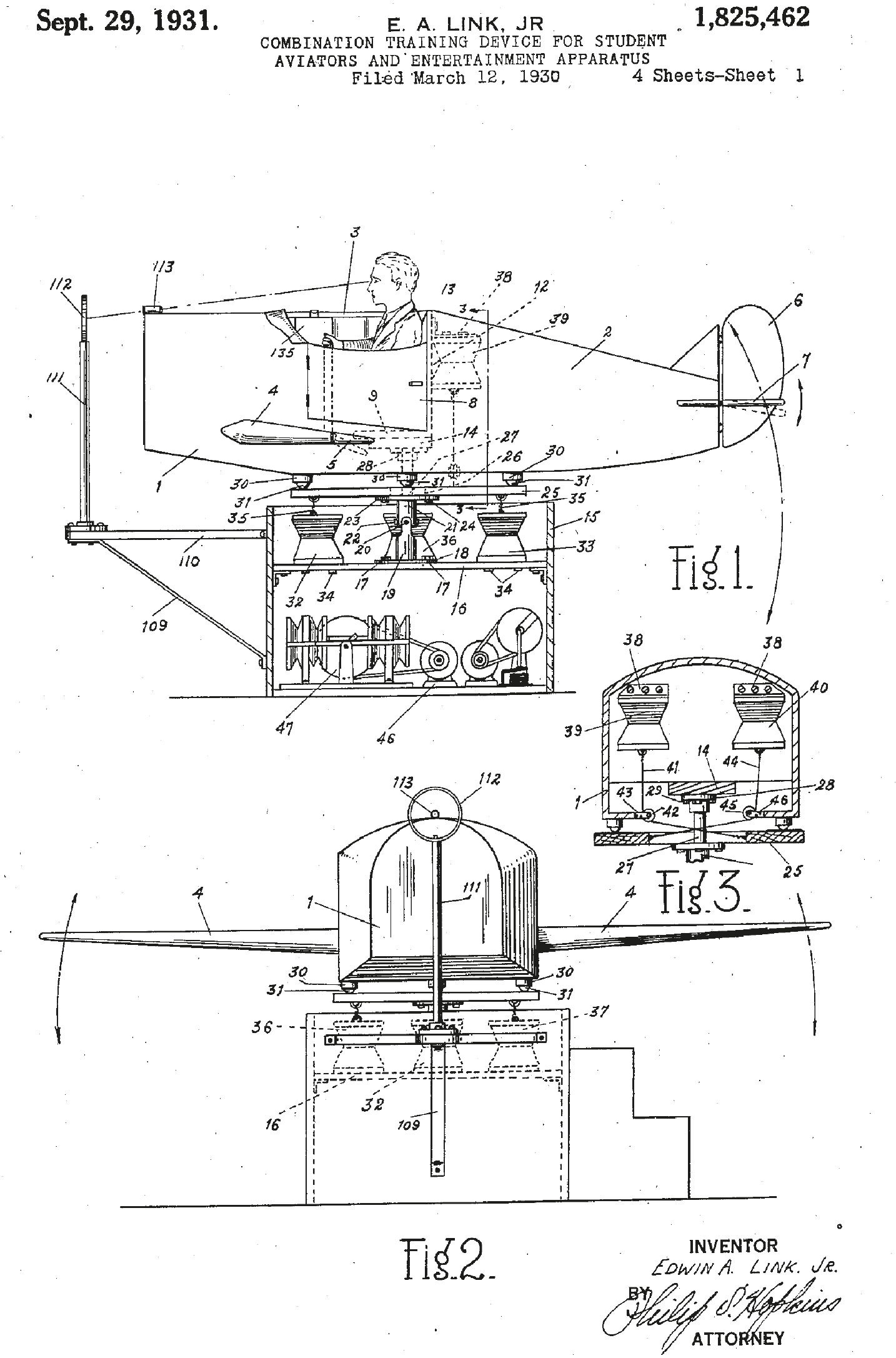
Another example of early VR was the plane simulator developed by Edward Link in 1929 and patented in 1931.4 Link enjoyed aviation, but as it was an expensive hobby, he could not easily afford the cost of plane hire. As his family business developed bellows and air pressure systems for musical instruments, he combined these to make a plane simulator so he could enjoy his pastime (Figure 2). This early immersive VR was realistic for its time and it allowed many people to train to become pilots and was nicknamed the ‘pilot maker’.5
Figure 2. The ‘pilot maker’.
Until this juncture, the notion of what we now recognize as virtual reality remained undefined. It was not until 1965 that Ivan Sutherland introduced the idea of the ‘Ultimate Display,’ a concept capable of mimicking reality so convincingly that individuals would struggle to distinguish it from actual reality. This groundbreaking concept incorporated a virtual realm observed through a head mounted display (HMD), enhanced by augmented 3D sound and tactile feedback, achieving remarkable realism. The synergy of these elements, combined with computer hardware, facilitated the creation and real-time maintenance of the virtual world. Crucially, this conceptual framework enabled users to interact with objects within the virtual environment authentically.6
Ivan Sutherland aptly quoted: ‘with the appropriate programming, such a display could literally be the Wonderland into which Alice walked.’ This visionary statement marked a pivotal moment, laying the foundation for the principles that underpin contemporary virtual reality. The paper outlining these concepts serves as a fundamental blueprint for the expansive realm of virtual reality as we understand it today.
During the subsequent years and with a clear vision, the technology was adapted further for military use. This led to NASA developing VR in 1985 to help train astronauts through their project ‘VIEW’. VIEW was the first VR technology to incorporate a dataglove. With this glove, the user could grasp virtual objects, issue commands with gestures and fly through the environment by simply pointing. The glove allowed for tactile feedback of simulated objects.7
Beyond military development, VR was accelerated by the gaming industry in the early 1990s. Companies such as SEGA and Nintendo started developing and investing heavily in these technologies. Although many were failures, for example the Nintendo Virtual Boy or the SEGA VR headset of 1995 (Figure 3), the groundwork for future developments was laid.8
Figure 3. The Nintendo Virtual Boy or the SEGA VR headset of 1995.
It was not until 2012 that Palmer Luckey developed a VR headset named Oculus, which gave the technology a renewed interest for hobbyists and end consumers. The crowdfunding campaign raised US$2.4 million to fund the project. The Occulus headset had relatively low resolution and was quite chunky, but where other companies had failed, this VR headset sold out and was very popular. The company stopped selling the original version and went into developing a Mark 2 version, which was a significant improvement.9 In 2014, Facebook, now Meta, acquired Oculus. This secured increased funding and resources for the development of VR and AR. This led to a massive influx of companies attempting the technology, further improving it.
In 2023, many companies such as Sony, Meta, Google, and others are improving existing VR and AR systems. Headsets such as the PSVR 2 from Sony, Vive XR Elite by HTC and Meta's Quest Pro are leading the field.
Uses of AR/VR in dentistry
Although VR was available in the 1990s, it was not implemented in the dental industry for three main reasons: cost, size and realism. These issues have largely been overcome and have become more applicable to the dental world, but a summary is below.
New VR technology is much cheaper now due to the rapid advancements in the digital technology industry. This was due to the development and mass production of displays, motion sensors and processing chips. This has allowed a greater implementation of VR devices, as return on investment is always a significant factor in applying new technology to practices.
Early headsets were very clunky and uncomfortable, and thanks to advancements, this is no longer the case. They are hand-held and wireless, ensuring improved patient comfort and experience.
Finally, VR used to have poor graphics and motion tracking, resulting in people experiencing motion sickness and headaches. With improved graphics and motion tracking, a more realistic experience for the user is gained, so it becomes more straightforward to implement without the previous side effects.
In dentistry, there is a greater lean towards AR due to the ability to superimpose helpful information and graphics, which can help with treatment or educational outcomes. VR is still present, but more in an education and teaching setting. Current applications include education, implant placement, maxillofacial surgeries and help with anxiety management.
Although the technology regarding dental applicability is still in its infancy, the rapid pace of technological advancement suggests that many applications will soon unfold. The ensuing paragraphs delve into potential applications and potential emerging benefits.
Education
AR and VR have significant educational benefits for the medical industry, including dentistry. One such benefit is in the way of learning anatomical knowledge, which is the foundation of a healthcare provider.10 Traditionally, dissections of cadavers have been used and have been proven to be invaluable for developing skills.11,12
Further to this, there has been concern over graduating dental students needing more anatomy knowledge because of a lack of exposure to cadavers during training.13 This lack of exposure to cadavers is multifactorial. However, some reasons include reduced cadaver donation and an increased student population, students with religious objections, and the risk of disease spread from cadaver interaction, particularly in light of the recent COVID pandemic.10,14,15 In light of the this, cadaver dissection in dentistry has reduced significantly or been cut out altogether.16 Alternative options, such as interactive digital cadaver tables and VR/AR are being researched.17
One method to help students improve their anatomical knowledge is AR, which can be used to highlight internal structures as an overlay on a person's body. This can be achieved by using a phone or device to see the overlayed graphics while scanning over a body part. This AR creates the illusion that the user can look inside their body while showing text information, medical images, and 3D models of organs that the user can interact with.18 This is greatly important in learning anatomical structures and a powerful tool to aid in learning essential information required of any dental or medical student.14
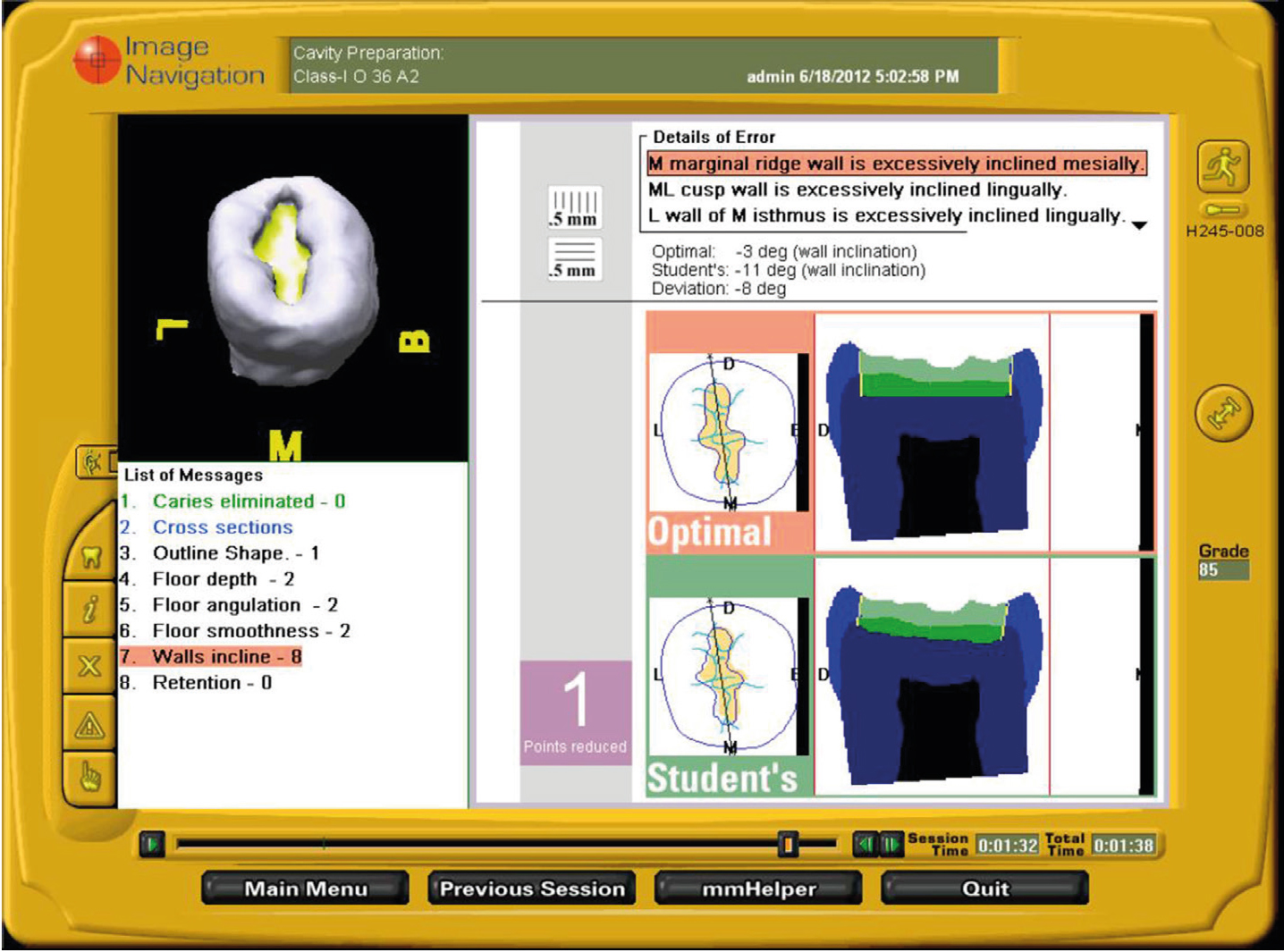
Aside from anatomy, other educational uses have been found, such as the DentSim simulator by Image Navigation. This is specifically designed for restorative dentistry, with university students in mind. DentSim is an augmented reality advanced dental training simulator (Figure 4). While seated at a manikin and preparing a cavity or crown preparation, the movement of the student's handpiece and the typodont-tooth are optically tracked and analysed in real-time.19 This allows for critical analysis of a student's ability but also identifies to the students themselves where they need to improve, resulting in targeted and efficient learning. Not only this, but it allows teachers a better grasp of which students need greater level of attention and mentorship.20
Figure 4. The DentSim simulator.10
The difference between knowledge and skills learned between traditional methods of learning and AR/VR have yet to be studied extensively, and therefore, no definitive conclusion can be made on the extent of any benefits, but some early studies do show benefits to AR in some aspects of skill gain, efficiency, and improved dexterity.21,22,23
Treatment planning and maxillofacial surgery
Historically, oral maxillofacial surgeons, prosthodontists and orthodontists would have to plan orthognathic surgeries from tracing paper of lateral cephalogram radiographs. The limitation was that this could only be achieved in the 2D view, so the results were unpredictable. This changed with digital radiographs, CT scans and programming, allowing for digital manipulation in the horizontal, vertical and transverse dimensions. These advancements improve surgery outcomes and treatment predictability.
Beyond this, a need to visualize structures has developed beyond profile views. The need for a high-fidelity patient model that simulates orthognathic surgeries for educational purposes has helped develop the virtual reality patient model (VRPM).24 Using the Oculus Rift head-mounted device, the user can be immersed in a simulated environment to aid in treatment planning and visualization. This technology is currently limited to the educational setting regarding treatment planning rather than treatment for real-world patients.25
The results demonstrate that simulation methods of increased fidelity (3D and VR) are appropriate alternatives to 2D conventional orthognathic surgical simulation methods when combined with traditional records.25 This demonstrated the validity of the technology and its use in orthognathic surgery. X-scope, an augmented reality tool for computer-assisted surgery, allows visual tracking of real anatomical structures in superposition with volume-rendered CT or MRI scans and thus can be used for navigated translocation of bony segments. One study found that X-Scope could accurately control the maxilla's translocation after Le Fort I osteotomy to within 1 mm. This programme was also used in tandem with conventional methods to reduce the risk of surgical failure.26 Although this technology is used for trauma cases, it could be translated to use in orthognathic surgeries, though more evidence is needed to determine the evidence for its use.
In the example of osteotomies of the facial skeleton, augmented reality has been proven helpful in helping in such surgeries. This worked by partial visual immersion of the surgeon overlaying patient-related virtual data, allowing continuous observation of the operating field and visual access to invisible anatomy.27
Anxious patients
Dental phobia is a fear of dentistry and dental situations, which can elicit a fight-or-flight response. While most phobias are irrational or excessive, in some situations, what is termed ‘dental phobia’ may be based on a previous bad or traumatic experience.28 It is estimated that 53% of adults suffer from fear and anxiety when visiting the dentist.29 This can be a barrier to treatment and prevent significant scores of people who need treatment from accessing the care they need.
The incorporation of AR and VR in helping manage anxiety in dentistry and the medical–dental field has been seen with great interest due to technology's advancements in portability, cost and increased realism. VR can be a distraction technique for those patients undergoing an inferior Alveolar nerve block (IANB). VR was found to have a significant positive effect on reducing dental anxiety in children when compared to no distraction.30 This would be exceptionally useful when creating a positive experience at the dentist.
Another use of VR is exposure therapy in VR form. This allows the patient to get used to the dental environment slowly, making them less anxious when attending appointments. Virtual reality exposure therapy (VRET) allows patients to face their fears in a controlled and safe environment. Patients may not feel the anticipated fear of getting hurt as they are aware of the fact that these simulations can be stopped, paused, and repeated if necessary.31,32
A systematic review of the effectiveness of VR interventions found that these interventions may reduce the anxiety and fear that patients experience during medical treatments.33
The literature has demonstrated the successful use of VR and AR to distract patients perioperatively and also to prepare patients for medical treatments. However, it must be noted that VR in dentistry has few studies; therefore, more research is required to determine its effectiveness.34
Dental implants
AR has been introduced and trialled for dental implant placement, and much of the research revolves around surgical accuracy and the use of retinal displays to aid in implant placement.35
During implant placements, there are often large amounts of information ignored when the available information is too much to process by the surgeon at that given time. AR can help with this in dental implant surgery as it can act as an automatic information filter. Information is selectively displayed, which reduces information overflow and offers intuitive image guidance.36
One study aimed to determine the accuracy of a virtually planned augmented reality-based dental implant placement system versus the actual prepared implant site. The study found that the deviation of implant placement from the planned position was significantly reduced by integrating surgical templates and augmented reality technology.37
Teledentistry
Although not explicitly related to dentistry, AR/VR has been used in teleconsultation and communication in cranio-maxillofacial surgery. This has resulted in improved surgical outcomes.38
Beyond the possible benefits in surgical outcomes, remote consultations for patients who have limited ability to travel could improve access to dentistry as a whole. The success of teledentistry hinges significantly on patients' willingness to embrace it and clinicians themselves. The absence of direct, face-to-face communication might amplify concerns among patients regarding the effective conveyance of their dental issues to the dentist. While addressing these challenges may require time, there is a growing trend toward increasing acceptance of telemedicine, with teledentistry gaining daily traction. Emerging evidence suggests a gradual rise in acceptability among patients and healthcare providers for teledentistry.39
VR could accelerate the acceptance rate among patients due to the virtual in-face meeting capabilities and help build rapport and trust for patients. There are yet to be any studies to determine the validity of this claim, but as the technology improves, more and more research is being carried out.
Wider dental applications
An additional application within the endodontics field involves using augmented reality for the automated real-time detection of root canal orifices. While the available data are currently limited, this application holds promising implications for enhancing treatment outcomes.40
Furthermore, a study in orthodontics demonstrated the use of augmented reality for guided bracket placement.41 This application in orthodontics enhances the precision of bracket placement, thereby contributing to more predictable treatment outcomes.42
As technological advancements continue to unfold, further applications are anticipated to emerge across all dental specialities. The ongoing evolution of technology is poised to introduce additional opportunities for innovative applications within the broader spectrum of dental practices
Discussion
Over the past two decades, virtual reality (VR) and augmented reality (AR) have undergone rapid development, resulting in a proliferation of applications. Notably, major corporations such as Google and Meta, endowed with substantial financial resources, have played a pivotal role in advancing the sophistication and refinement of these technologies. VR has found extensive application in education and anxiety management, leveraging its immersive experience. In contrast, AR has demonstrated utility in surgery and restorative dentistry, primarily attributed to its benefits in graphic and information overlay.
The promising applications of VR and AR extend notably to education, surgery, restorative dentistry and anxiety management. Nevertheless, the literature specific to dentistry remains limited, given the recent emergence of these technologies within the field.
Conclusion
Presently, evidence-based recommendations for AR/VR in dental applications are limited, and clinical protocols remain in their infancy. Nonetheless, there is a growing fascination with AR/VR applications, particularly in dental education, offering interactive learning experiences with round-the-clock accessibility and objective evaluation. In maxillofacial surgery and restorative dentistry, AR/VR technology emerges as a promising tool for intricate procedures, contributing to the delivery of predictable and safe therapeutic outcomes.
Future research should prioritize establishing technological standards characterized by high data quality. Developing approved AR/VR devices intended for routine clinical and educational use is crucial for advancing the field. Only then can its validity and effectiveness be determined, which will undoubtedly revolutionize the digital landscape.43