This article looks at the background to the current changes in primary care dentistry being piloted in England. It looks at the structure of the different elements being piloted, such as the oral health assessment, interim care appointments and care pathways. It also examines advanced care pathways and how complex care will be provided when clinically feasible and beneficial to the patient.
The authors have worked in a Type 1 pilot practice since September 2010.
Clinical Relevance: The NHS contract currently being piloted in England delivers care through care pathways and clinical risk assessments with prevention as an important building block for the delivery of services. There are new measures planned for measuring quality outcomes in primary care. This has implications for how services are delivered, who delivers them and how dentists will be remunerated in the future.
Article
Why is change needed?
The NHS was created in 1948 to provide a health service available to all and financed entirely through taxation. When first established, the oral health needs of the population were very different from today – with high decay rates, routine multiple extractions and denture placement.1 Over the last 60 years, extensive research has helped to determine the aetiology of many dental diseases,2 allowing a large proportion of dental disease to be preventable now. The use of fluoride, coupled with this increased knowledge, has changed the dental needs of today's population – decreasing levels of dental disease have been reported by the Adult Dental Health Survey (2009)3 and the Child Dental Health Survey (2003).4 We now need to move away from simply addressing the problems present, to preventing their occurrence and finding an NHS system which rewards a preventive focus from dental teams rather than one based on activity (ie treatment).1
NHS reforms 2006
The old ‘fee per item’ NHS system was appropriate when the NHS was first introduced but is no longer suited to today's needs. From 1948 to the new reforms in 2006, any dentist who wanted an NHS contract could get one and set up an NHS practice wherever he/she wanted to, subject only to being eligible to be on a dental list. The location of dental practices was market driven rather than based on where services were needed most in terms of oral health needs. In 2006, the NHS reforms were introduced.5 Primary Care Trusts (PCTs) were given power to commission dental services (previously by the NHS), patient registration was removed and the patient charging system was simplified (Table 1) with the introduction of Units of Dental Activity (UDAs). With this system, dentists were paid per course of treatment. The payment system was such that, whether a patient had one or multiple fillings, crowns or extractions, they would pay the same amount – the value for that band of treatment. This was all with the aim of improving access and quality and increasing the focus on prevention.
£49 (whether one or more of the 3 named provided in same course of treatment)
3
3
Crowns, Bridges, Inlays, Onlays, Dentures
£214 (whether one or more of 12 the named provided in same course of treatment)
4
The Health Select Committee Report6 found the new system generally failing to improve access, with many dentists moving away from NHS dentistry, and the number of Courses of Treatment (COTs) decreased. The new simplified patient charges created concerns of overcharging if a patient had only one filling, and undercharging for patients who saved up all their dental problems for one course of treatment. The system encouraged Performers to ‘game’ the contract to maximize the UDAs per course of treatment by splitting courses of treatment artificially rather than providing the entire planned treatment as one course, eg providing RCT in one course of treatment (COT) and claiming 3 UDAs and then 3 months later submitting another COT and claiming 12 UDAs for a crown on that same tooth. The number of root canal treatments (RCTs) decreased by 45% and the number of extractions increased – creating a growing concern that patients were not receiving the quality of care that they needed. It is important to note that there was no pilot system to test out the 2006 NHS reforms. Improvements suggested included:
Reinstating patient registration;
Increasing the number of UDA bands; and
Ensuring the new system was piloted.
There was also the realization of a need to reward dentists with incentives to provide preventive care.
NHS pilots
The NHS pilots have been running since September 2010.7 Their aim is to improve access, quality and oral health. The system and remuneration in these pilots are based on registration, capitation and quality, moving away from the current contracts based on Units of Dental Activity (UDA). There are three types.
Type 1 pilots
These practices have been given the same contract value as the previous year, provided they deliver the same level of NHS commitment as they did the year prior to the start of the pilots. NHS commitment in this context means providing the same number of NHS hours on the same number of patients as had been provided in the previous year. The purpose of the Type 1 pilot is to explore how patients can be cared for when adhering to the new pathway when financial incentives relating to activity levels or numbers of patients seen are removed, and how practices organize themselves as a team to deliver this.
Type 2 pilots
These practices receive their NHS payments based on a model of weighted capitation payments. The practice remuneration is adjusted depending on the pilot's capitation payments, with capitation payments for individual patients varying depending on their age, gender and the deprivation status of their home postcode. The capitation payment in Type 2 pilots relates to all care – preventive, routine and complex treatment. The purpose of the Type 2 pilot is to explore a payment system based on weighted capitation where remuneration is adjusted based on the patient's demographic details (with payments intended to compensate for the average cost of care for an individual in that patient cohort). Therefore, a practice's contract value is effectively dependent on the number of patients for whom care is provided.
Weighted capitation
This is the amount of money contracted to a practice per patient per year and will vary in amount based on the patient's demographic profile, ie age, sex and deprivation score of their residential address.
Type 3 pilots
These practices are also paid based on a model of weighted capitation payments. Remuneration levels are adjusted depending on the pilot's capitation payments, with capitation payment for individual patients varying depending on their age, gender and the deprivation status of their home postcode. With Type 3 pilots, capitation payment is related to preventive and routine treatment only. The element of a Type 3 pilot's contract value associated with complex care (generally ‘Band 3’ treatments requiring laboratory work) is fixed and guaranteed and not subject to any adjustment associated with capitation. The purpose of the Type 3 pilots, like Type 2 pilots, is to explore the impact of applying a remuneration model based on weighted capitation. The aim of the Type 3 pilots is also to explore the impact of separating out the remuneration for complex care.
What is common to all the pilots is the care pathway which commences with a detailed oral health assessment.
Oral health assessment (OHA)
The oral health assessment is the building block of the care pathway and the outcome of the process is to produce an individual risk assessment based on specific patient questions and a clinical examination.
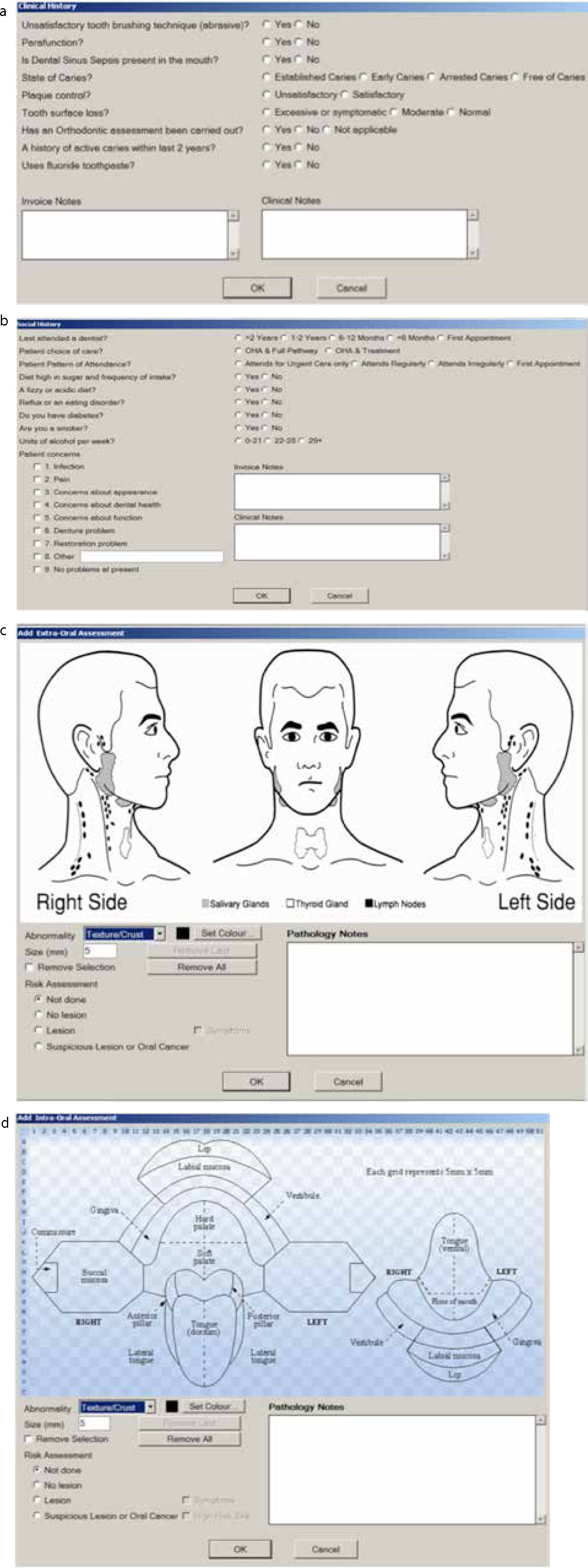
Figure 1 shows the format for ‘software of excellence’ – this varies slightly from system to system in appearance. The oral health assessment follows a standard examination familiar to all clinicians, but additionally software algorithms have been developed to allow a risk status to be assigned to this patient (Red – Amber – Green, RAG). Based on this information, recommended evidence-based preventive treatment and interventions can be provided. The clinician must still use his/her own judgement to decide what treatment, if any, is necessary.
Figure 1. Screen shots of (a) clinical history, (b) social history, (c) extra-oral examination recording, as shown on exact ‘software of excellence’ and (d) soft tissue.
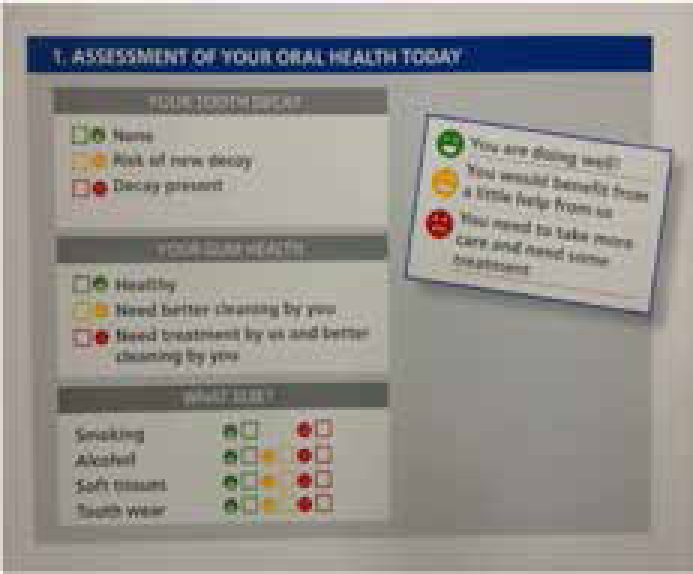
The OHA starts with a variety of questions designed to determine the patient's oral health (Figure 2). The key areas which are mandatory are the medical history, clinical history (eg sugar intake, fizzy drink intake, smoking status and alcohol intake), a Basic Periodontal Examination (BPE) and the clinical examination. Based on the responses provided by the patient and the clinical examination results, the patient is then assigned to one of three oral disease risk level groups: Red (high risk), Amber (moderate risk) and Green (low risk) in each of the following four fields (Figure 3):
Caries;
Periodontal;
Soft tissues;
Tooth surface loss.
Figure 2. Format of oral health assessment.8 Key: SCP – Self Care Plan; RAG – Red/Amber/Green; ICM – Interim Care Management.Figure 3. Self Care Plan showing RAG score.
Once assigned to a risk level, a care pathway with a preventive treatment plan is formulated by the computer software, governed by the age-specific guidelines set in Delivering Better Oral Health.
Practitioners have reported good feedback on the OHA, with the majority agreeing that it encourages self-care, supports communication with patients and enables evidence-based care tailor-made to each individual.9
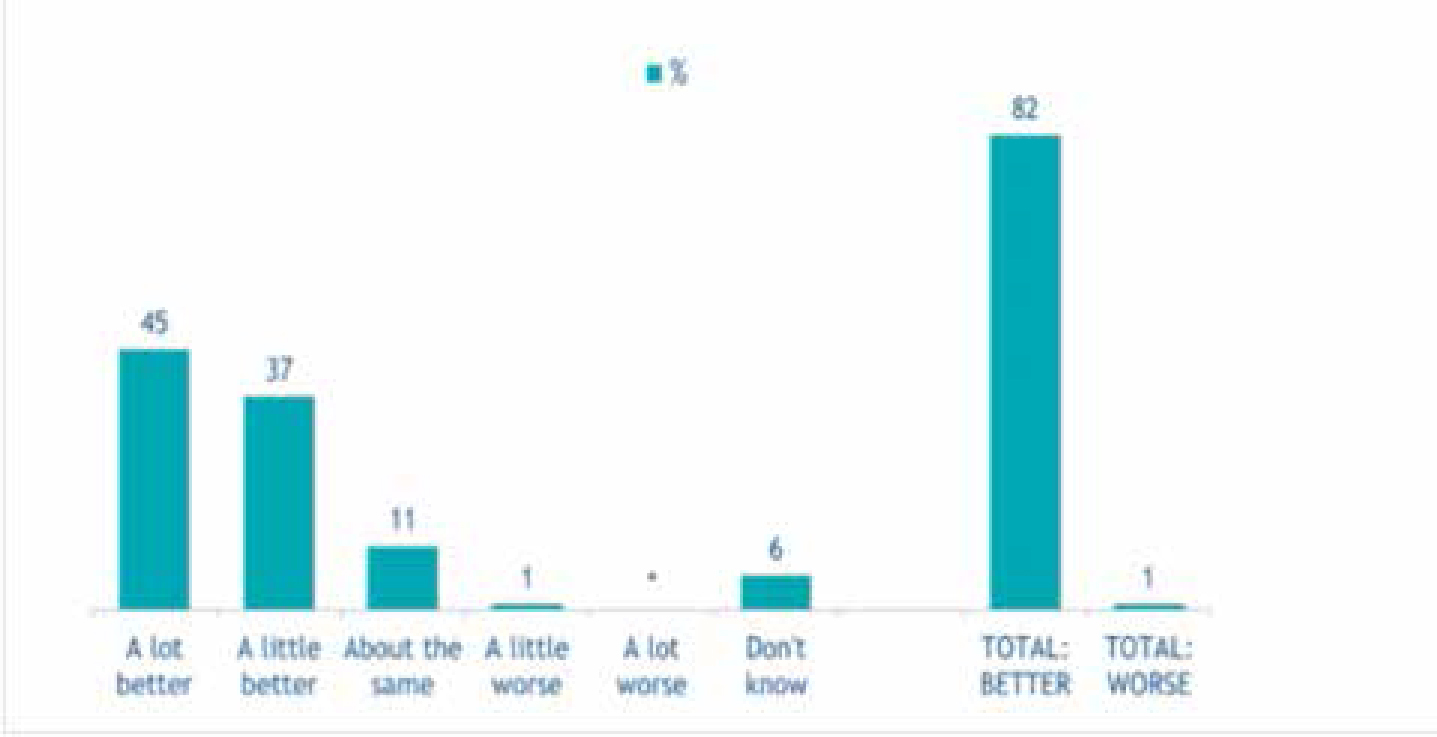
Early feedback on the pilots has shown an increase in waiting time for examination appointments since the start of the pilots (Figure 4). This could possibly be explained by the examination appointments now routinely taking longer at 20–30 minutes, reflecting the thoroughness of the assessments and provision of evidence-based advice and instructions.
Figure 4. Average waiting time for existing patients.8
Interim Care appointments (ICs)
The computer software will also formulate one or more Interim Care appointments (ICs). IC appointments may involve preventive treatment and/or advice, instead of (or as well as) treatment to address dental decay (eg fluoride application, prescription of higher strength fluoride). Each patient is provided with a printed self-care plan showing all these details. A clinical care pathway is formulated at the OHA and a new pathway will start again at the Oral Health Review (OHR) at the determined recall interval.
The response to ICs documented in the Dental Contract Reform Pilots Evaluation (Figure 5) shows patients and practitioners agree that it is helpful in continuing to motivate patients to improve their oral health; however, uptake varies among those who do not value the preventive ethos or have not understood the value of it in their individual cases.
Figure 5. Staff views on whether the OHA enables better care to be provided to patients.13
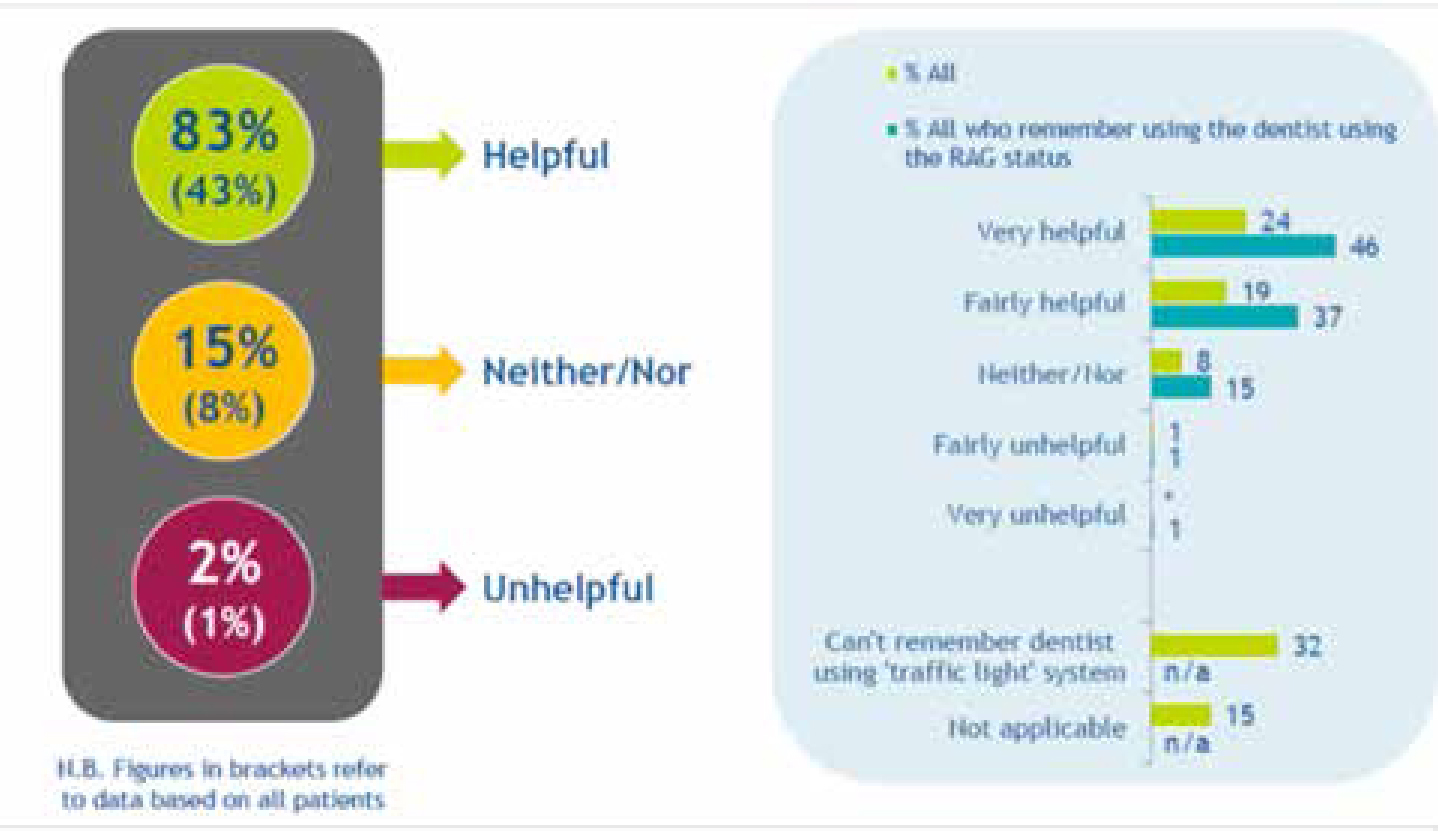
Early feedback from NHS Dental Pilots has, overall, shown a positive response to the new system. The majority of patients report that they now understand more about their oral health and generally find the new RAG system (Figure 6) and self-care plans (SCPs) helpful in understanding the health of their teeth and gums. The practitioner survey showed the majority agree that the pilot approach has the potential to improve the oral health of their patients and the new way of working provides better care for their patients. However, problems were reported with the software causing disruption to clinics in the early stages,9 such as getting used to the new software and information which must be completed before oral health assessment can be completed.
Figure 6. Helpfulness of Red/Amber/Green rating (Patients).8
The ICs and longer OHAs place a large strain on the appointment books. The majority of dentists and practice staff agree that, if the current pilot is implemented, there will be a shift in skill mix in practice. Nurses are currently being trained to carry out extended duties, such as fluoride application and oral hygiene education, and the use of dental therapists to carry out non-complex care for children and adults will increase. This may result in an increase in demand for dental therapists and a decrease in demand for dentists owing to differential labour costs.
Care pathways
Care pathways have been defined as ‘the methodology for the mutual decision-making and organization of care for a well-defined group of patients during a well-defined period’.10 The development of clinical guidelines was recommended to minimize variation in the quality of care. It also allows for ‘determination of thresholds for treatment’. In the NHS Pilots, Delivering Better Oral Health (DBOH)11 has been used as the evidence-based toolkit to formulate the care protocol – an action plan based on national clinical guidelines. The aim of the care pathway is to:
Enhance the quality of care by improving patient outcomes;
Promote oral health;
Increase patient satisfaction; and
Optimize resources (utilizing the whole dental team).
Care pathways have been used as a tool to achieve continuity of care and provide a consistent pathway for given clinical conditions.
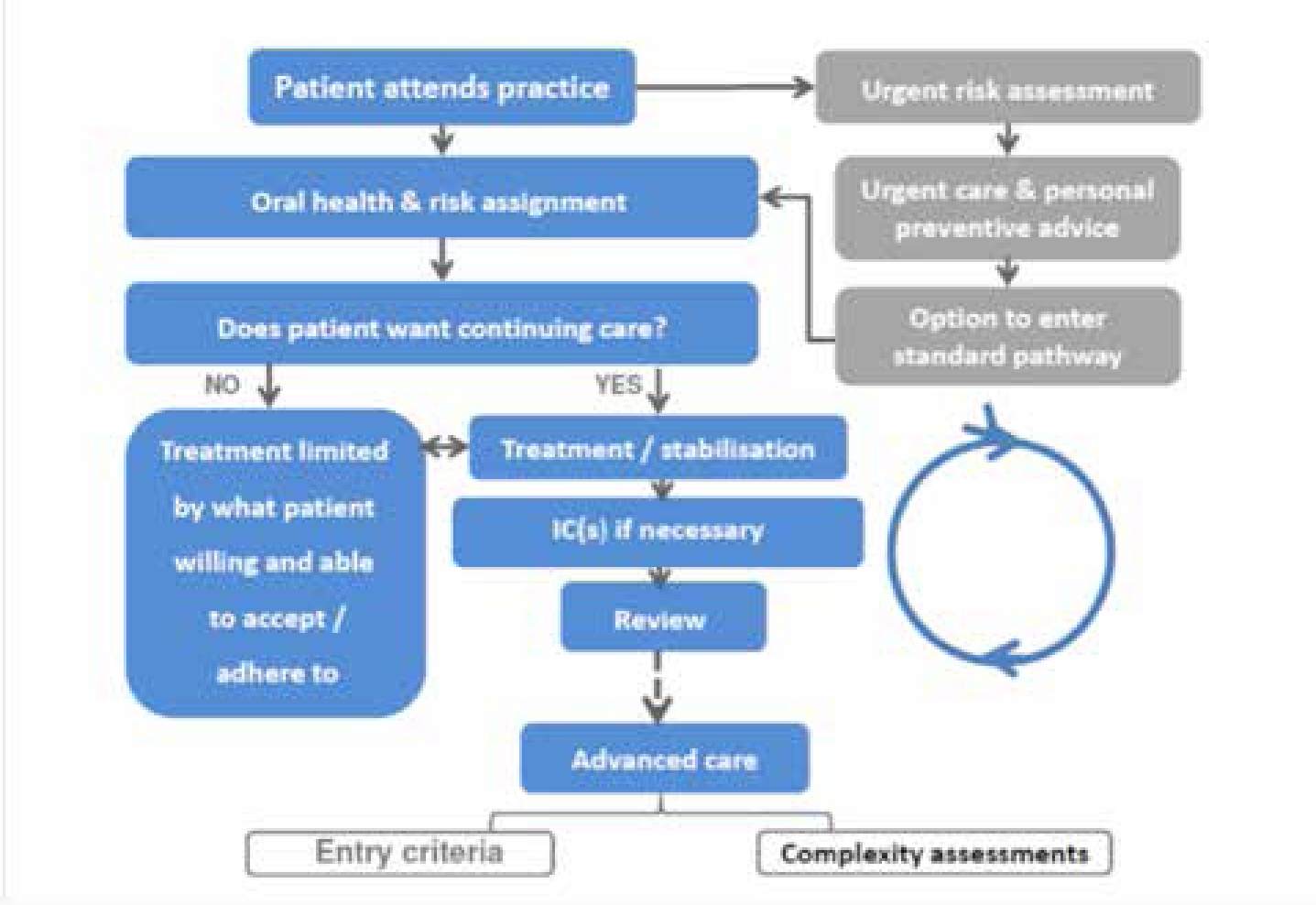
Figure 7 illustrates the flow of a patient through the care pathway. Those patients attending for urgent care are provided with pain relief or stabilization and then offered an oral health assessment. Patients entering the care pathway via the oral health assessment are given an RAG status (as explained earlier). Care protocols are part of the self-care plan. The care protocol for each diagnostic group defines the number and type of each preventive intervention (as recommended by DBOH) and also the recall period (recommended by NICE guidelines).12 These can be over-ridden based on the clinicians’ judgement. The care protocol also specifies that, for patients in the ‘Red’ category, no complex treatment (including root canal treatments, crowns, bridges, cobalt-chromium dentures) can be provided, only stabilization of the active disease. Conversely, any patients in the ‘Green’ category would be entitled to any treatment deemed necessary on the NHS.
Figure 7. Diagrammatic representation of a care pathway.13
Those patients who fall into the ‘Red’ high risk category would be re-assessed at their next recall appointment. If their RAG status improved, they may then be entitled to complex care. In the case of a ‘Red’ patient requiring root canal treatment, who is re-assessed and found not to have improved in RAG status, there are two options, either leave the tooth as it is or extract it.13
Advanced care pathways
Advanced care services are resource intensive treatments, which include indirect restorations, metal-based partial dentures and advanced endodontic and periodontal treatments. It is good clinical practice only to provide these treatments when the maximum benefit in terms of outcome can be achieved for the patient. Evidence suggests that, if they are provided in the presence of active disease, ie periodontal disease and/or dental caries, the outcome is much reduced.14
These pathways were originally devised by clinicians and representatives of the British Society of Restorative Dentistry and the British Society of Periodontology. The pilots are exploring ways of managing the gateway to advanced care by ensuring that the treatment provided fulfils two essential criteria:
The treatment is clinically feasible;
The treatment is beneficial to the patient.
The exercise of clinical judgement is required to decide on how beneficial and feasible the advanced care treatment will be and, whilst no objective criteria or descriptors have been developed so far, this will no doubt be the subject of some debate.
The pilots are also testing how the skill level of the practitioner can be used to ensure the best possible outcome for the patient.
The descriptors of the skill levels are as follows:
Skill level 1: work to be carried out by GDP and set at the equivalent of the Dental Foundation year;
Skill level 2: work to be carried out by GDP who has additional competencies;
Skill level 3: Work to be referred to specialist services.
There are significant long-term infrastructure implications of these proposals, including the commissioning of sufficient Level 3 services, education and training programmes for Level 2 dentists and remuneration models commensurate with the skill level.
Skill mix
More specific care pathways are now being developed, for example, for ‘red caries children’ (children at high risk of developing caries) or ‘red periodontal disease adults’ (adults at high risk of periodontal disease), and as the evidence base in these areas improves the pathway will be modified. Figure 8 shows how the new model may change and favour a greater skill mix in the dental practice.15
Figure 8. Adult amber caries patient.15
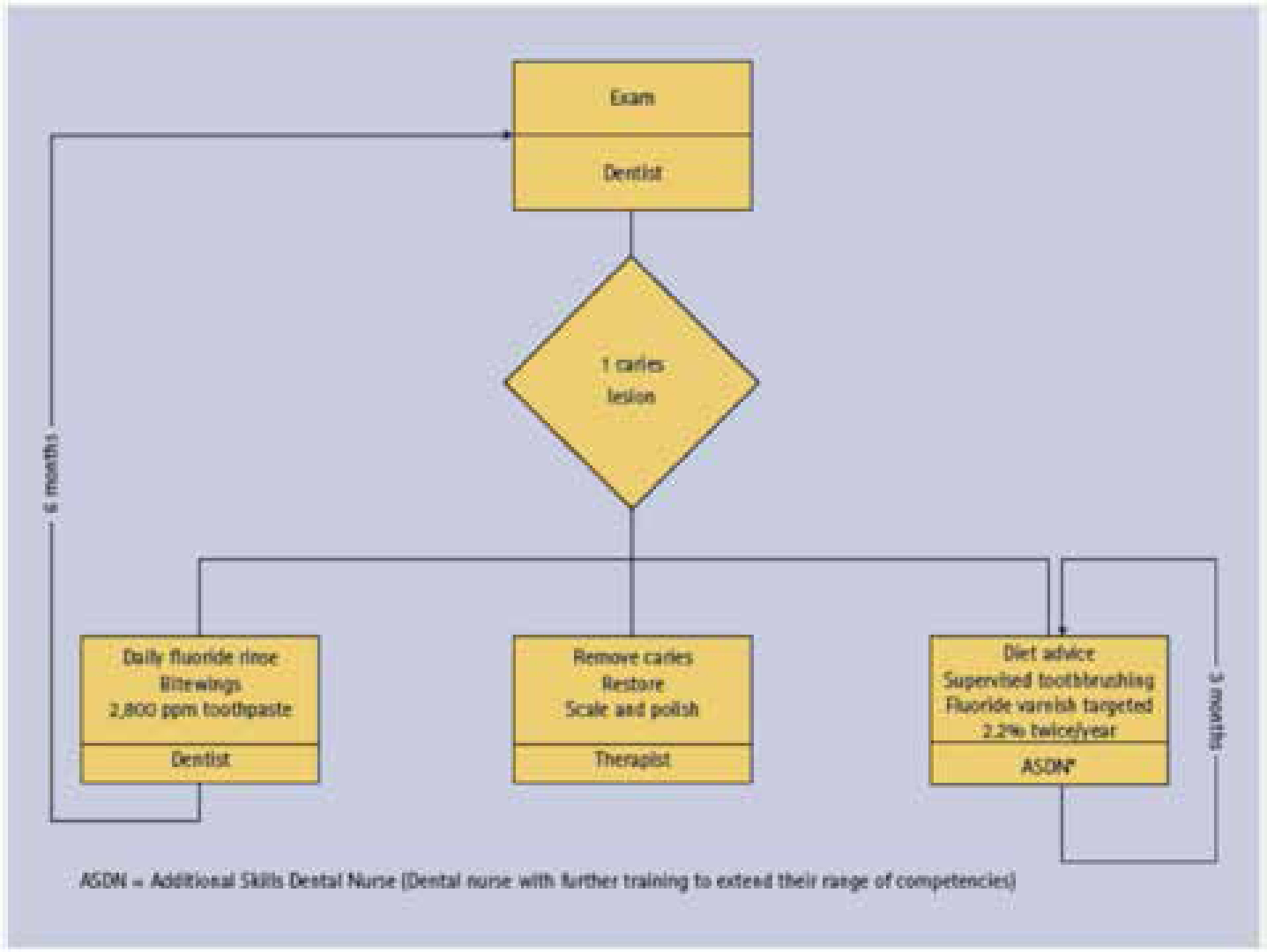
With the focus moving to prevention, more members of the dental team can become part of the care pathway. As shown in Figure 9, a patient with a carious lesion would be diagnosed by the dentist, prescribed high fluoride toothpaste and fluoride mouthwash for prevention, provided with a restoration by the hygiene therapist and more prevention advice and topical fluoride application by an extended duties nurse.
Figure 9. Practice owner views on whether and how to consider changing his/her practice skill mix in future.8
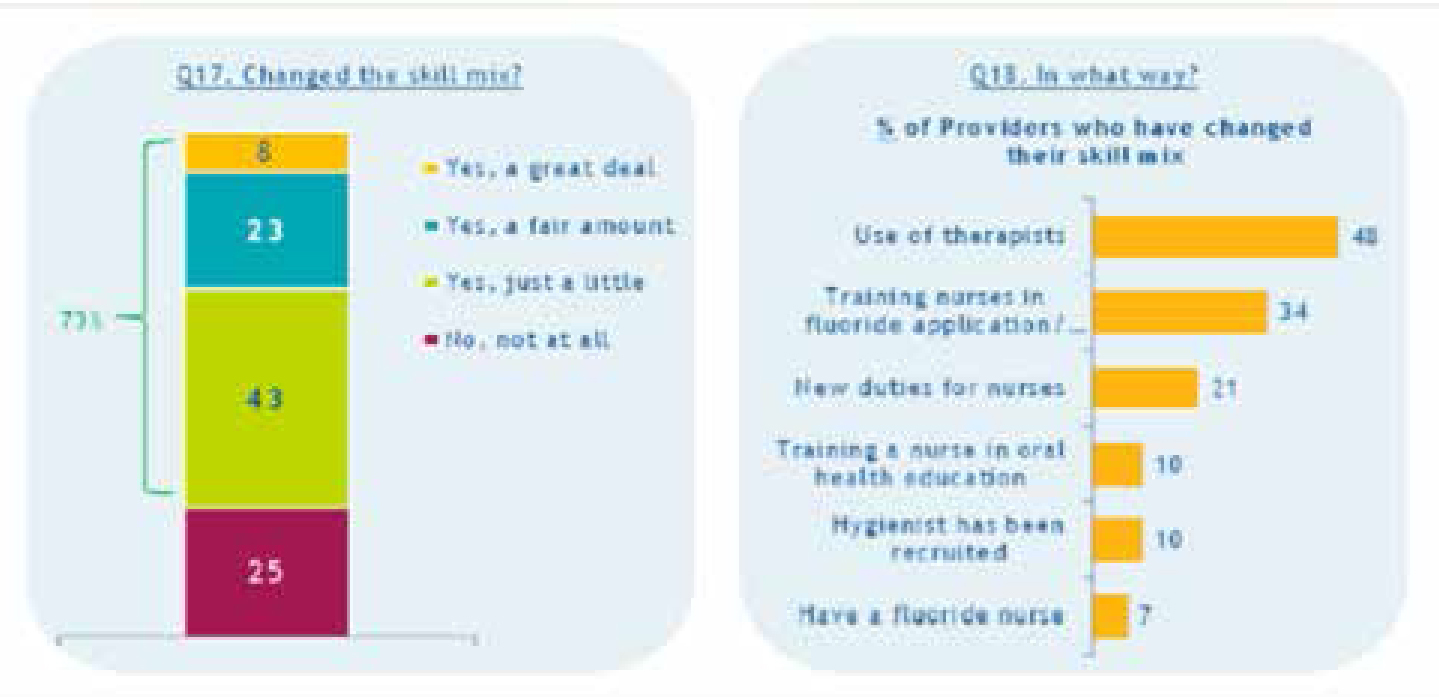
Figure 10 shows how some practices within the pilots have changed their skill mix to meet demands of the new system.8
Figure 10. Changes to the skill mix in the practice as a consequence of the care pathway.8
Quality
The Department of Health is piloting a method of measuring the quality of the work provided by dentists and the clinical outcomes they achieve. This is thought to be a better way of holding dentists to account rather than simply measuring activity.
The Dental Quality and Outcome Framework (DQOF) equates to 10% of the practice's contract value and is weighted as follows:
60% Clinical effectiveness;
30% Patients' experience;
10% Safety.
With clinical effectiveness, the focus is on ensuring that preventive advice that is given is acted upon and results in a measurable difference in a patient's oral healthcare. Table 2 illustrates the measures.
Active decayed teeth (dt) ages 5 years old and under, reduction in number of carious teeth/child50% Under 5s active decay (dt) improved or maintained
150
Active decayed teeth (dt) ages 6 years old and over, reduction in number of carious teeth/child75% over 6s improved or maintained
150
Active decayed teeth (dt) reduction in number of carious teeth/dentate adult75% improved or maintained
150
75% patients with BPE improved or maintained at oral health review
75
50% patients with BPE 2 or more with sextant bleeding sites improved at oral health review
75
It is also interesting to note that a patient's views will be taken into account and form part of the measure that ultimately determines a practice's income at the end of the year. Whilst these are necessarily subjective views, raising quality with patients in mind is an essential part of providing a consistently high quality of care and means that the whole team will be required to deliver on these outcomes.
Summary
There are some concerns which have already been highlighted by the pilots:
Waiting times have increased significantly owing to longer oral health assessments (30 minutes) and the introduction of ICs;
Patient acceptance of a new system. Patients under the current system have become accustomed to receiving treatment at the same appointment as the examination, and being entitled to complex care, even if their oral health is not optimal. The introduction of NICE recall guidelines has proved difficult for patients to accept as they are used to ‘6-monthly check-ups’;
Adapting to new systems – for both dentists and patients. As explained earlier, getting accustomed to the new computer software takes some time, as does explaining the new oral health assessment procedure to patients;
De-skilling of dentists in providing advanced care for high risk patients, as these patients will not be entitled to complex care unless their oral health improves. This may mean dentists are carrying out advanced care less frequently.
Less clinical judgement – the preventive clinical care pathway may become quite prescriptive and, whilst there is an option always to override these, this may trigger exception reports if this is done too often by the dentist.
The new NHS contract will be based on a care pathway principle and the remuneration for practices will be based on a capitation model. Advanced care will be available for patients for whom it is clinically feasible and beneficial and the dental team will become increasingly involved in the delivery of a preventive care pathway. For some this contract will be an opportunity and a chance to develop themselves and their practices, whilst for others it might appear as a worrying challenge. Many details are yet to be finalized, along with statutory regulations, but the direction of travel is now well established.