Article
We read with interest the series by Bell et al, ‘The maxillary sinus: what the general dental team need to know’.1,2 The series is most informative, and we would like to indicate some other areas of the dental relevance of the maxillary sinus.
The authors discuss the role of trans-alveolar removal of dental roots displaced into the sinus. This is a widely used and accepted technique. However, functional endoscopic sinus surgery (FESS) is a minimally invasive technique for the removal of foreign bodies from the maxillary sinus. Under general anaesthesia, an endoscope is placed in the nostril, and an opening created under endoscopic vision in the inferior meatus. The camera is advanced into the sinus, and grasping forceps used to retrieve the root.
The authors outline the technique of closing an oro-antral communication (OAC) by means of a buccal advancement flap. In cases of chronic oro-antral fistulae, there is evidence that such surgery is combined with FESS to increase antral drainage by creating additional drainage of the sinus via the inferior meatus. Various techniques to close OACs are described, including buccal and palatal advancement flaps.3 In cases of chronic fistulae, the mucoperiosteal flap is augmented with a buccal fat pad flap.3,4 FESS has a complication rate of less than 1%.4
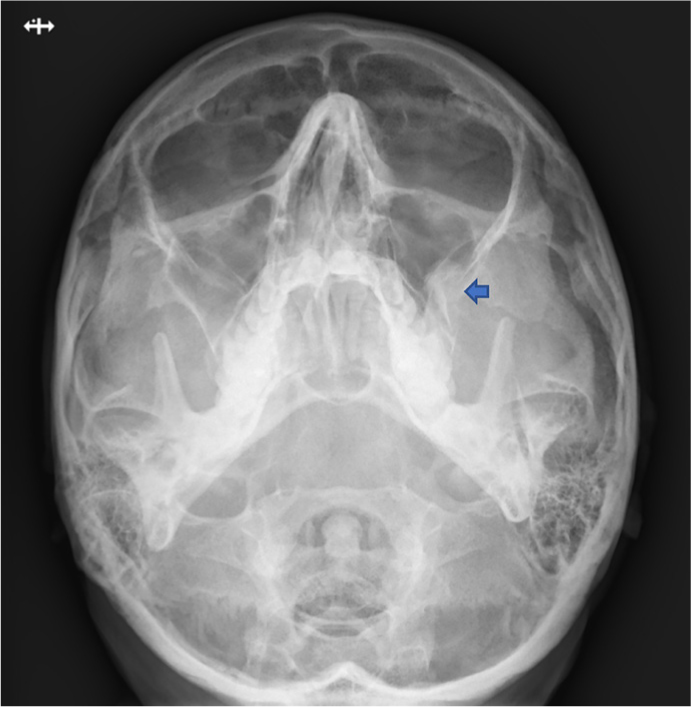
Other findings that we would like to share are the radiographic signs of zygomatic complex fractures, showing as discontinuity of the lateral wall of the maxillary sinus, and air/fluid levels in the sinus. These features can be seen in occipitomental (OM) radiographs, or sometimes on orthopantomograms (Figure 1).5