Article
A fit and well 28-year-old gentleman was referred to the Oral Surgery department at Ealing Hospital by his general dental practitioner for a specialist opinion regarding his upper 2nd and 3rd molar teeth. His GDP had taken periapical radiographs during the root canal treatment of the 1st permanent molars and noted that the 2nd molars were in fact unerupted.
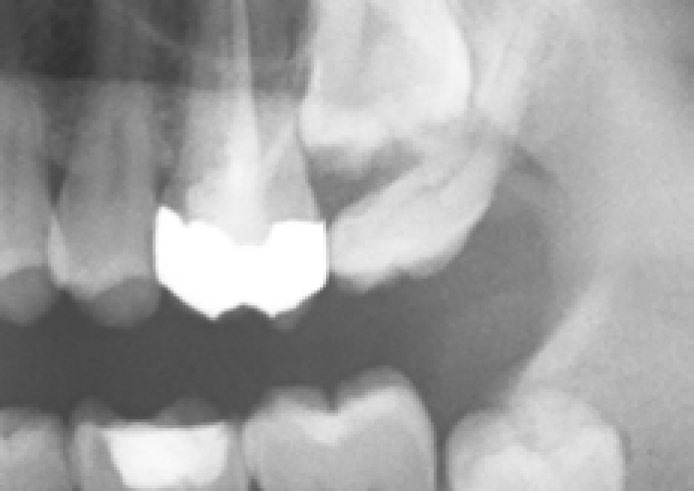
At presentation the patient's only complaint was of mild generalized temperature sensitivity and, upon examination, no abnormalities were detected extra- or intra-orally. Upon review of an OPG radiograph (Figures 1 and 2) it was noted that both upper 2nd molar teeth are fully formed and completely unerupted. Both 3rd molar teeth are fully erupted and mesially angulated to such a degree that they contact the upper 1st molars.

A more focused clinical examination of the upper 3rd molars showed them to have good interproximal contacts with the upper 1st molars and good occlusal contacts with the lower 2nd molars by virtue of the selective attrition of the disto-occlusal surfaces, with exposed dentine, compensating for their mesial angulation. This wear, along with the wider than normal embrasures, were the only indication that the last standing molars were in fact 3rd molars.
Owing to the lack of any pathological or functional issues, the patient was keen to avoid treatment; the only treatment advised was topical fluoride preparations, desensitizing toothpastes and resin sealers to reduce the sensitivity of his exposed dentine. With regards to the elective extraction of his upper 3rd molars, the probability of spontaneous eruption of the upper 2nd molar teeth is very low; this is because of his age and the fact that the teeth are fully formed, which results in very little eruptive potential, but also because the most likely cause of their original absence, prior to their impaction against the upper 3rd molars, was primary failure of eruption.
It is important, upon the discovery of such an abnormality, that we remember always to act in our patient's best interests; however, with such an unusual presentation, seeking a second opinion about any possible intervention was appropriate.