Martin IC, Langtry JAA Cutaneous lesions of the maxillofacial region. In: Ward Booth P, Schendel SA, Hausamen JE (eds). St Louis: Churchill Livingstone; 2007
Kerawala C, Newlands COxford: Oxford University Press; 2010
Telfer NR, Colver GB, Morton CA Guidelines for the management of basal cell carcinoma. Br J Dermatol. 2008; 159:35-48
Motley R, Kersey P, Lawrence C Multiprofessional guidelines for the management of the patient with primary cutaneous squamous cell carcinoma. Br J Dermatol. 2002; 146:18-25
Roberts DLL, Anstey AV, Barlow RJ, Cox NH UK Guidelines for the Management of Cutaneous Melanoma. Br J Dermatol. 2002; 146:7-17
Dyer TA, Robinson PG General health promotion in general dental practice – the involvement of the dental team. Part 2: A qualitative and quantitative investigation of the views of practice principals in South Yorkshire. Br Dent J. 2006; 201:45-51
Lecturer and Specialty Registrar, Division of Oral and Maxillofacial Surgery, School of Oral and Dental Science, University of Bristol, Lower Maudlin Street, Bristol, BS1 2LY
Professor and Consultant in Oral and Maxillofacial Surgery, Division of Oral and Maxillofacial Surgery, University of Bristol, Lower Maudlin Street, Bristol, BS1 2LY, UK
The incidence of skin cancer in the United Kingdom is increasing and is associated with an ageing population and increasing lifetime exposure to sunlight. The three most common types of skin cancer are basal cell carcinoma, squamous cell carcinoma and malignant melanoma, all three of which may present on the skin of the face. The dental team are, therefore, well-placed to recognize suspicious lesions and arrange for further advice or assessment. This paper outlines the epidemiology, important clinical features and principles of modern management of facial skin cancers to aid dental practitioners in the recognition of suspicious lesions. In addition, some of these treatments have side-effects which have the potential to affect a patient's oral health or its management and these aspects are also discussed.
Clinical Relevance: The dental surgeon is ideally placed to recognize malignant or potentially malignant lesions on patients' faces and to advise on seeking further advice or refer for assessment, as appropriate. Dental practitioners will increasingly encounter patients who have undergone surgical or non-surgical management of facial skin cancer and should understand the potential oro-facial side-effects of such treatment.
Article
The incidence of skin cancer in the United Kingdom is increasing. Skin cancers are grouped into two categories: malignant melanomas and non-melanoma skin cancers (NMSCs). The melanomas are the least common but most lethal, whilst the much more common NMSCs generally have a better prognosis providing that they are treated appropriately at an early stage. Of the NMSCs, basal cell carcinoma (BCC) and squamous cell carcinoma (SCC) are the most common types and are the only two that will be discussed in detail in this paper.
A knowledge of the basic anatomy of the skin helps illustrate the pathophysiology of skin cancer. The skin is made up of the renewable outer epidermis and the deeper dermis that gives strength and flexibility to the skin. Like the oral mucosa, the epidermis is made up of several cell layers, the most superficial of which is the stratum corneum and the deepest, the basal cell layer. Between the epidermis and dermis is a basement membrane. In addition, skin contains hair, sebaceous and sweat glands and various specialized nerve endings.1 The skin cancers discussed in this paper arise from cells within the epidermis and their relative mortality rates reflect their propensity to breach the basement membrane to cause regional and distant disease.
The three most common facial skin cancers will be discussed in turn, highlighting the key clinical features that should alert the dental practitioner to their diagnosis. The management of facial skin cancers may involve surgery, topical medical treatment in the form of creams or ointments, radiotherapy or a combination of strategies. The treatment modality selected depends on many factors including:
The type and site of the cancer;
The general health of the patient; and
Patient preferences.
The general principles of treatment of the common cancers will be illustrated followed by a discussion of the potential oro-facial side-effects of skin cancer treatment.
Basal cell carcinoma (BCC)
Epidemiology
As a group, the NMSCs are far more common than cutaneous melanomas and there were more than 98,000 cases in the UK in 2008.2 Indeed, BCC is the most common cancer in humans and 80% of these present in the head and neck region. These lesions occur most commonly in people aged over 60 years and have a very low propensity to metastasize. There is a genetic predisposition to the development of BCC in patients with Gorlin syndrome (basal cell naevus syndrome; the features of which include multiple BCCs at a young age and keratocystic odontogenic tumours).
Clinical features
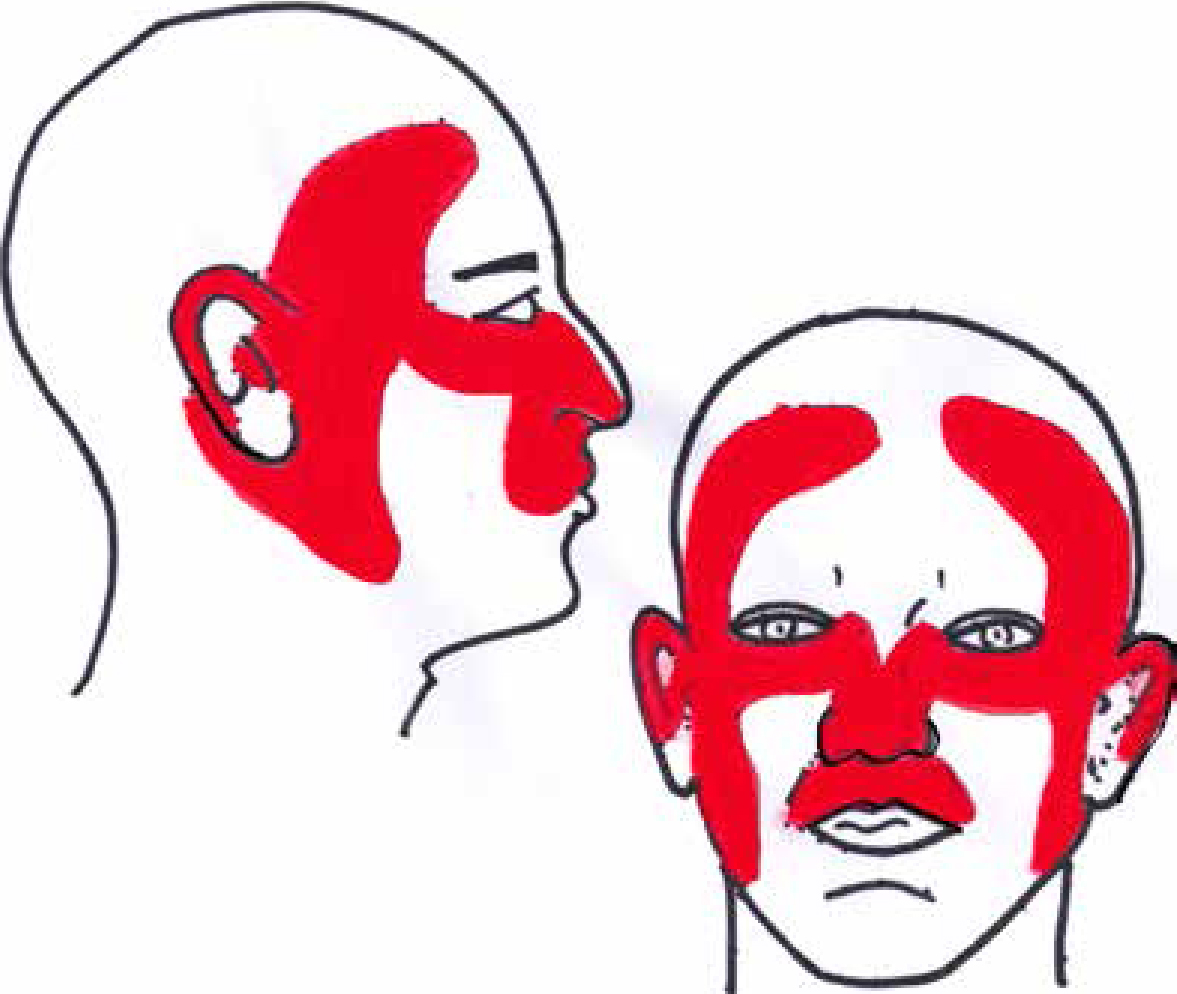
Basal cell carcinomas (also known as rodent ulcers) are derived from the basal cell layer of the epidermis and over 90% occur on sun-exposed areas, including the face and scalp. Figure 1 shows the high-risk areas for the development of BCCs on the face. BCCs usually present as slowly-growing, nodular lesions with a pearly raised edge with telangiectasia. There may be a central ulcer if necrosis has occurred (Figure 2). Less commonly, BCCs present as tense, cystic lesions or as an ill-defined, plaque-like morphoeic form (which occur most frequently on the face). BCCs are usually less than 1cm in diameter but, left untreated, will grow and can be locally invasive, with the potential to cause destruction of bone and adjacent organs. However, they only very rarely metastasize to lymph nodes or distant organs.3,4,5
Figure 1. Diagram showing areas at high risk of development of BCC and SCC on the face.Figure 2. Nodular BCC on lateral aspect of nose showing rolled, pearly edges and central ulceration.
Management
The majority of BCCs are treated surgically. Surgery aims to remove the entire lesion plus a margin of normal tissue peripheral and deep to it. The size of this margin is determined by the type and site of the lesion, as well as the presence of adverse histological features indicative of a risk of aggressive behaviour. For example, a nodular basal cell removed with a 4 mm margin will result in a cure in 95% of cases.6 Surgical excision may be followed by primary closure (for small lesions and where the skin can be closed without tension), local skin flaps or skin grafts. Figure 3 shows surgical excision for a BCC of the nose where the surgical defect has been reconstructed with a rotation flap. Figure 4 shows a larger BCC of the nose where the resultant defect has been corrected using a full thickness skin graft.
Figure 3.
(a) Basal cell carcinoma on right side of nose. Resection margins marked in dotted line. The solid line indicates the outline for a local ‘bi-lobed’ flap for reconstruction. (b) Immediate post-operative image. The defect has been closed using rotation of local skin. (c) Image at one month post-surgery showing excellent cosmetic result.Figure 4.
(a) A large basal cell carcinoma of the left side of the nose. The dotted line marks the edges of the lesion. The required surgical margins are marked in solid ink. (b) The resultant large surgical defect. (c) The defect was reconstructed using a full thickness skin graft harvested from behind the ear. This image shows the result at 3 months after surgery.
An alternative to surgical excision for BCCs are the less destructive techniques, including curettage and cautery, and cryosurgery. The obvious limitation of these techniques is the inability to determine the surgical margin and there is, therefore, evidence of higher rates of recurrence for lesions treated in this way.
If patients are unwilling or unable to tolerate surgery, or if the lesion is in an anatomical area that would make surgical reconstruction very difficult, radiotherapy is often the treatment of choice. Complications include damage to adjacent normal skin and other organs (including the eye).
Squamous cell carcinoma (SCC)
Epidemiology
Like BCC, cutaneous SCC occurs mostly in people aged over 60 years. With an ageing population and a steadily increasing incidence, these lesions are a growing health problem in this country. Exposure to sunlight is the main risk factor for the development of non-melanoma skin cancers. Having a history of one of these lesions increases the likelihood of another. In addition to sunlight, smoking pipes or cigars is a risk factor for developing SCC of the lower lip. Whilst BCCs have a very low propensity to metastasize, the cutaneous SCCs may do and around 500 people die each year from this disease in the UK.2 It is important to emphasize that, in terms of metastatic potential and overall prognosis, SCC of the facial skin has much more favourable outcomes when compared with SCC of the oral cavity.
Clinical features
Squamous cell carcinomas arise from keratinocytes in the epidermis and are also commonly found on sun-exposed areas of the skin. On the face, the high-risk areas are the same as for BCCs (Figure 1) but, in addition, pipe and cigar smoking is associated with SCC of the lip.3 SCCs present as slow-growing lesions of variable morphology and they may arise in an area of actinic keratosis. Actinic keratosis is a potentially malignant lesion that presents as flat or thickened, scaly or reddened areas that represent abnormal skin cell development due to UV radiation. The risk of SCC occurring within an area of actinic keratosis is 10–15%.5 SCCs may also present as nodules or as ulcerated lesions (Figure 5). In contrast to intra-oral mucosal SCCs, those appearing on the skin metastasize much less commonly. Approximately 5% of skin SCCs metastasize and this is most likely if the original SCC was on the lip or ear.5 A dental practitioner noticing a lesion suspicious for cutaneous SCC on the face should, therefore, examine the neck for lymph node involvement. Two important differential diagnoses are worth mentioning here. The first is the keratoacanthoma, which is a common, rapidly-growing lesion with a central keratin plug that resembles SCC clinically. The difference between keratoacanthoma and SCC is that the former will spontaneously involute with time. However, most such lesions will, at least, be biopsied to exclude SCC. The other important differential is the Merkel cell carcinoma which arises from specialized neuro-endocrine cells. These present as painless lesions which may ulcerate. The importance of these lesions is the high mortality rate of around 30%. Figure 6 shows an example of a keratoacanthoma.
Figure 5. Ulcerated SCC on the upper lip.Figure 6. Keratoacanthoma of the upper lip showing characteristic keratinization.
Management
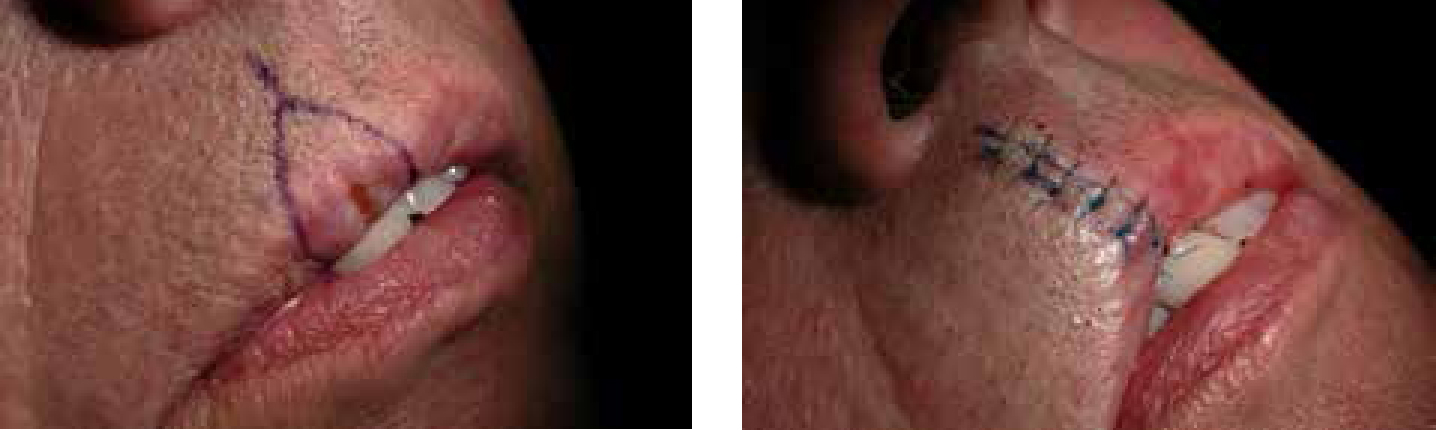
As for BCCs, the treatment of choice for cutaneous SCC is surgical excision and reconstruction, where possible. The peripheral margin taken at resection is determined in part by the size of the lesion and usually ranges from 6 mm to 1 cm.7 In addition to excision of the primary lesion, the presence of lymph node metastasis may necessitate the removal of lymph tissue by neck dissection. Figure 7 demonstrates the surgical excision of a SCC from the upper lip and primary closure allowed by the natural laxity of the lip tissue.
Figure 7.
(a) Squamous cell carcinoma on upper lip. Surgical ‘wedge’ resection margins marked. (b) Immediate post-operative image showing successful primary closure with minimal cosmetic or function deficit.
In some patients, it is not possible or desirable to perform surgery. For certain types of skin cancer (including BCCs, some SCCs and pre-malignant lesions like actinic keratosis), topical chemotherapy creams or ointments may be used. Examples of such agents include Imiquimod and diclofenac sodium, which are generally applied to the lesion daily for a number of weeks. These drugs are particularly useful where there is widespread skin change, for example, on the scalp of bald men. In addition, radiotherapy has a role in the management of cutaneous SCC.
Malignant melanoma
Epidemiology
Cutaneous malignant melanomas are the least common of the skin cancers but, in the past 30 years, the incidence in the UK has increased four-fold. In 2008, there were just under 12,000 new diagnoses and it is now the sixth most common cancer in both sexes in this country. The disease affects women more commonly than men, but more men die from it. Whilst the majority of cases are in people over the age of 65 years, one-third of patients are under 55 and, in 2008, there were more than 900 cases in those aged between 15 and 34 years. In men, the most common sites affected are the chest and back, whilst the legs are the most common site in women. Overall, between 14 and 22% of malignant melanomas present in the head and neck region. In contrast to many cancers, the incidence of malignant melanoma is higher in more affluent populations and, in the UK, the highest incidence is found in the South-west of England.2
The most important risk factor for the development of malignant melanoma is exposure to sunlight. Factors which further increase the risk include:1
Fair skin and blue eyes;
Having many freckles or moles, particularly large or shaped moles;
A history of sunburn, especially occurring at a young age;
Use of sunbeds (especially in younger people);
Having a close relative who has a history of a skin cancer.
Clinical features
Melanomas develop from melanocytes in the epidermis, but only a minority arise in a pre-existing naevus (mole). In a small proportion, there may be no obvious skin lesion, and the presenting feature may be of lymph node (including in the neck) or distant organ metastasis (usually lung, liver or brain). There are several clinical sub-types of cutaneous melanoma, the most common of which is the superficial spreading type (Figure 8). Other types include nodular and amelanotic (ie lacking pigment) melanomas. Lentigo maligna is a pre-malignant lesion that arises in sun-damaged skin, often on the face, and usually needs treatment as a proportion of these lesions will become invasive. As with any new lesion presenting in the face or mouth, it is important to examine the lymph nodes of the neck thoroughly for possible metastatic involvement.3,4,5
Figure 8. Malignant melanoma on the bridge of the nose showing classic clinical features.
When assessing a suspicious pigmented lesion, the ‘ABCDE’ approach is useful (Table 1).5
A – Asymmetry in the outline of the lesionB – Border irregularity (eg ragged or blurred)C – Colour variation (eg different shades of brown and black or white, red or blue coloration)D – Diameter of >6 mmE – Evolving changes in the lesion over time (eg ulceration or bleeding)
Management
Once a patient has been referred to a specialist for assessment of a suspicious skin lesion, the first step in the majority of cases will be an incisional biopsy to ascertain the histology. However, this differs for a suspected melanoma where excision of the mole is recommended as this allows for assessment of the depth of the lesion (also known as the Breslow thickness or Clark level). This depth is crucial in determining the margin with which a melanoma is excised and also has prognostic significance. As with the non-melanoma cancers, surgical exicision is the treatment of choice for cutaneous melanoma. However, the surgical margins required to maximize cure are generally much wider, ranging from 1–4 cm depending on the depth of the cancer.8 The potential functional and cosmetic consequences of resection of a large melanoma on or around the face are factors requiring careful discussion with the patient before surgery is carried out. There are no proven benefits of adjuvant therapies for cutaneous melanoma but chemotherapy may be used in the setting of a clinical trial.
The main features of facial skin cancers are summarized in Table 2.
Basal cell carcinoma
Squamous cell carcinoma
Malignant melanoma
Site
Sun-exposed areas of face and scalp including forehead, lips, nose, ears, cheek prominence.
Sun-exposed areas of face and scalp including forehead, lips, nose, ears, cheek prominence. Lip lesions not related to sun exposure seen in pipe and cigar smokers.
Potentially any area of the head and neck skin.May present as lymph node metastasis in the absence of an obvious primary lesion.
Typical lesion
Nodule with pearly, raised edge and fine telangiectasia +/- central ulcer. May bleed when crust falls off.May present as indistinct flat lesion.
Ulcerated or nodular lesion with rolled edges. May bleed.
Asymmetrical pigmented lesion with irregular border. May bleed or itch. History of increasing size.
Pre-malignant lesion
None recognized
Actinic keratosis – presents as dry, scaly, red area of skin often on face or scalp (eg bald, older men).
Lentigo maligna – presents as a flat, often large, pigmented lesion and frequently on the face of older patients.
Involvement of cervical lymph nodes or distant metastasis
Extremely rare
Uncommon but occurs in up to 10% of ulcerating lesions.
More common than for the other skin cancers.
The role of the dental team in detecting suspicious skin lesions
The dental team may notice suspicious skin lesions during routine treatment or check-up consultations and patients may seek the advice of their dental practitioner about a lesion, particularly if it is on or around the lips. As with intra-oral lesions that are suspicious for cancer, it is not appropriate for these skin lesions to be biopsied in primary dental care, but it is appropriate for the dentist to discuss his/her findings with the patient and advise on seeking further assessment or, alternatively, refer the patient. Options include:
Referring the patient to the local oral and maxillofacial surgery (OMFS) unit for assessment of the lesion. Most OMFS units now offer a skin cancer treatment service for BCCs and SCCs and some deliver a melanoma service also. Members of the OMFS team will also be happy to provide advice to the dental team over the telephone.
Advise the patient to consult with his/her general medical practitioner, who may then arrange further referral if appropriate. If the lesion is suspicious for malignant melanoma, the dental practitioner may, with the patient's permission, discuss the case with the GMP, who can then see the patient and arrange fast-track referral for assessment in a specialist clinic, if required.
In addition, it is well recognized that preventive measures will be key in helping to combat the steadily-increasing incidence of skin cancers. The dental team can help in this effort by providing prevention advice posters and leaflets in surgery waiting rooms, although there is evidence that dental practitioners do not feel adequately trained or funded to provide verbal advice on skin cancer prevention.9
Impact of skin cancer treatments on oral health and dental treatment
Although the majority of treatments for facial skin cancers will not directly impact on the oral health or dental treatment, there are potential relevant side-effects, as summarized in Table 3. The dental team have an important role in screening the oral tissues of patients before chemotherapy and radiotherapy and in maintaining good oral health during and after these treatments. Figure 9 illustrates a large peri-oral surgical resection, but with relatively limited long-term structural compromise resulting from use of local flaps that maximize the relaxed skin tension lines.
Potential oro-dental effects
Surgery
Surgery for lip cancers may:
Reduce the size of the mouth complicating access for oral hygiene, dental treatment or insertion of dentures. However, even with large wedge excisions of the lower lip, this usually improves over time.
Result in devitalized areas of the lip. Again, with time, this should resolve to some degree.
Radiotherapy
Radiotherapy to a wide field that may include the salivary glands or jaws carries the risk of:
Xerostomia and subsequent caries and periodontal disease;
Mucositis and ulceration;
Trismus;
Osteoradionecrosis;
New or recurrent cancers in the field of radiation.
Chemotherapy
Systemic chemotherapy for any cancer may cause oral side-effects including:
Mucositis and ulceration;
Haematological side-effects which may have implications for dental treatment (eg low platelets complicating extractions; neutropenia increasing infection risk).
Figure 9.
(a) Intra-operative image showing outline of a large squamous cell cancer on the upper lip (dotted line). Also shown are the resection margins and further incisions required to allow advancement of local tissue to close the defect. (b) Despite extensive peri-oral resection, the effects on function and aesthetics at three months post-operation are minimal.
Summary
The dental team should have an awareness of facial skin cancer as an important, growing health problem in the United Kingdom. In this paper we have outlined the main epidemiological and clinical features of the most common skin cancers and provided a brief overview of their management. In addition, this article has highlighted potential oro-dental implications of treatments for skin cancer. It is hoped that dental professionals will recognize potentially cancerous lesions on the faces of their patients and feel confident in advising patients on seeking further advice or, if appropriate, referring the patient for specialist assessment. In addition, there is increasing interest in the role of the dental team in the prevention of disease in general, and it may be that dentists can contribute to public health messages about skin cancer by, for example, stocking information leaflets in practice waiting rooms.