Ozkan Y, Varol A, Turker N Clinical and radiological evaluation of cherubism: a sporadic case report and review of the literature. Int J Pediatr Otorhinolaryngol. 2003; 67:1005-1012 https://doi.org/10.1016/s0165-5876(03)00179-4
Kannu P, Baskin B, Bowdin S Cherubism. In: Adam MP, Feldman J, Mirzaa GM (eds). Seattle, WA, USA: University of Washington, Seattle; 2018
Ghawsi S, Schwartz K, Korsgaard N, Thorn JJ Non-familial cherubism: a rare case report with long-term clinical and radiological follow-up. J Oral Maxillofac Surg Med Pathol. 2022; 34:195-199 https://doi.org/10.1016/j.ajoms.2021.09.006
Edwards PC, Fox J, Fantasia JE Bilateral central giant cell granulomas of the mandible in an 8-year-old girl with Noonan syndrome (Noonan-like/multiple giant cell lesion syndrome). Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 2005; 99:334-340 https://doi.org/10.1016/j.tripleo.2004.08.021
Battaglia A, Merati A, Magit A Cherubism and upper airway obstruction. Otolaryngol Head Neck Surg. 2000; 122:573-574 https://doi.org/10.1067/mhn.2000.103534
Ricalde P, Ahson I, Schaefer ST A paradigm shift in the management of cherubism? A preliminary report using imatinib. J Oral Maxillofac Surg. 2019; 77:1278.e1-1278.e7 https://doi.org/10.1016/j.joms.2019.02.021
Kaugars GE, Niamtu J, Svirsky JA Cherubism: diagnosis, treatment, and comparison with central giant cell granulomas and giant cell tumors. Oral Surg Oral Med Oral Pathol. 1992; 73:369-374 https://doi.org/10.1016/0030-4220(92)90137-f
Tekin AF, Ünal ÖF, Göksel S, Özcan İ Clinical and radiological evaluation of cherubism: a rare case report. Radiol Case Rep. 2020; 15:416-419 https://doi.org/10.1016/j.radcr.2020.01.003
Carvalho Silva E, Carvalho Silva GC, Vieira TC Cherubism: clinicoradiographic features, treatment, and long-term follow-up of 8 cases. J Oral Maxillofac Surg. 2007; 65:517-522 https://doi.org/10.1016/j.joms.2006.05.061
Chen Wongworawat Y, Jack D, Inman JC Regional lymph node enlargement in clinically severe cherubism. Clin Pathol. 2019; 12 https://doi.org/10.1177/2632010X19861107
Misra SR, Mishra L, Mohanty N, Mohanty S Cherubism with multiple dental abnormalities: a rare presentation. BMJ Case Rep. 2014; 2014 https://doi.org/10.1136/bcr-2014-206721
Von Wowern N Cherubism: a 36-year long-term follow-up of 2 generations in different families and review of the literature. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 2000; 90:765-772 https://doi.org/10.1067/moe.2000.108438
Hernández-Alfaro F, Arenaz Búa J, Mareque Bueno J, Badía C Orthognathic surgery in cherubism. J Oral Maxillofac Surg. 2011; 69:541-545 https://doi.org/10.1016/j.joms.2010.07.065
Yilmaz B, Ozan O, Karaagaclioglu L, Ersoy AE A prosthetic treatment approach for a cherubism patient: a clinical report. J Prosthet Dent. 2006; 96:313-316 https://doi.org/10.1016/j.prosdent.2006.09.014
Cherubism is a skeletal dysplasia limited to the maxilla and mandible, affecting children and adolescents. A 13-year-old male patient was referred to the Oxford University Hospitals Oral and Maxillofacial Surgery Department, by his orthodontist, following an incidental finding of bilateral multilocular radiolucencies of the mandible. This led to multiple clinical, radiographic, histopathological, genetic and biochemical investigations involving various medical and dental specialities. The multidisciplinary approach led to the successful management of this patient. Even though cherubism is self-limiting, long-term radiographic and clinical surveillance is required.
CPD/Clinical Relevance:
Dentists should understand the clinico-radiographic presentation of cherubism and have an awareness of how the possible functional and aesthetic complications associated with the condition are managed.
Article
Cherubism is a rare and non-neoplastic condition, limited to the maxilla and mandible. It is a type of skeletal dysplasia characterized by multilocular, bilateral and symmetrical fibro-osseous lesions, causing painless expansions of the jaws. The pathogenesis is commonly attributed to a mutation in the gene encoding for SH3-binding protein 2 (SH3BP2), which leads to the localized degradation and replacement of bone with fibrous tissue.
Cherubism has a childhood onset, with lesions first appearing between the ages of 2 and 7 years, and progressing until puberty. It is self-limiting, and there is regression and involution of the bone lesions during pubertal bone remodelling.2 The phenotypic symptoms range from a normal appearance to gross bilateral maxillomandibular deformities. These can lead to a rounded facial appearance, retraction of the lower eyelids leading to increased scleral show, drawing resemblance to a cherub.3 There are a plethora of differential diagnoses for cherubism. These include but are not limited to odontogenic or non-odontogenic cysts of the jaw, odontogenic tumours and giant-cell lesions.2
Although typically an isolated condition, aggressive cherubism can result in secondary respiratory, ocular, and dental anomalies.4 It is pertinent to have an understanding of the clinical and radiographic features observed in patients with the disease because it is often first detected by a patient's general dental practitioner (GDP). This case report outlines how an incidental finding by a patient's orthodontist led to a medical and dental multidisciplinary investigation to diagnose and treat cherubism in a paediatric patient.
Case report
A 13-year-old medically fit and well male patient was referred to the Oxford University Hospitals Oral and Maxillofacial Department, by his Orthodontist, following an incidental finding of bilateral multilocular radiolucencies of the mandible. The patient presented with no concerns and was asymptomatic. On examination, extra-oral examination was unremarkable with no obvious facial asymmetry. Intra-orally, the mandibular rami were symmetrical with no obvious cortical expansion. No paraesthesia or dysaesthesia was noted.
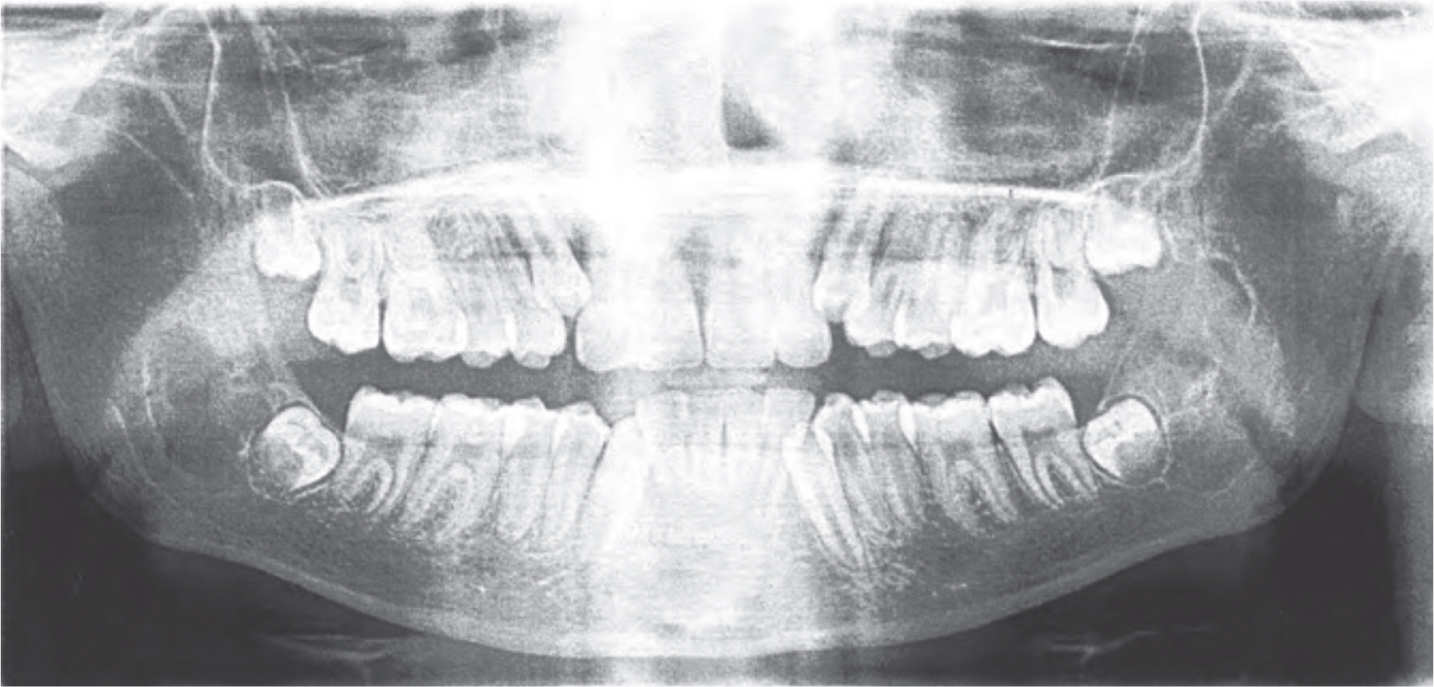
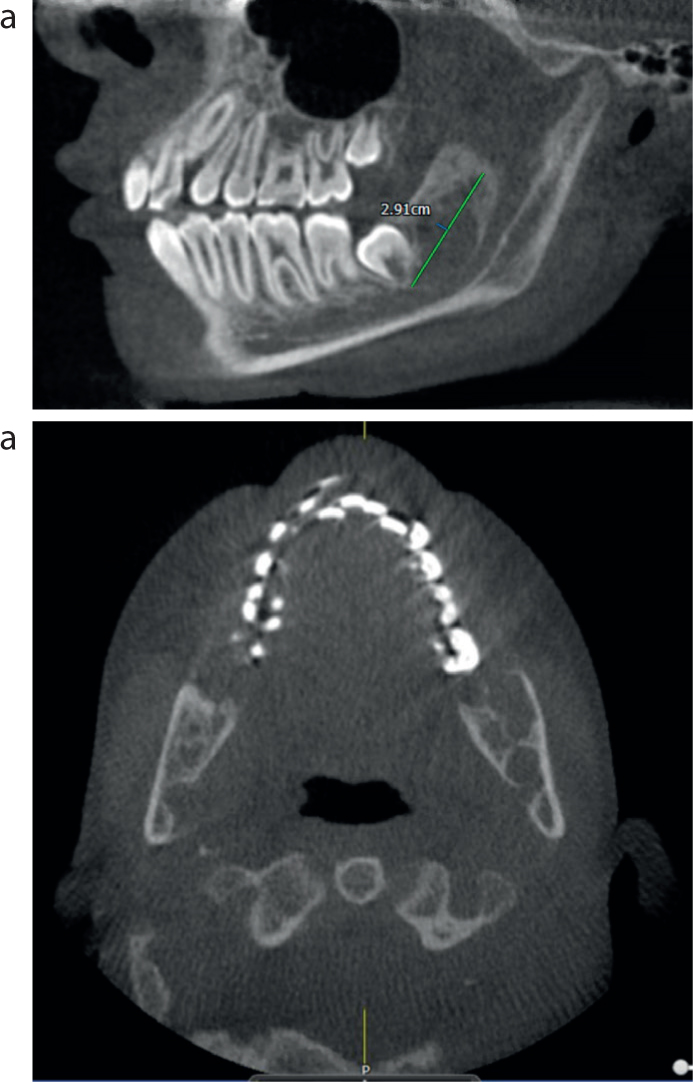
The orthopantomogram (OPG) radiograph (Figure 1) showed multiple multilocular radiolucent lesions in the mandible and a cone beam CT scan (Figure 2) showed expansile lytic lesions. Multiple differential diagnoses were considered, all of which typically present radiographically as multilocular, soap bubble appearances. These included ameloblastoma, giant cell tumour, odontogenic myxoma and odontogenic keratocyst, with particular suspicion of the latter owing to its more commonly bilateral and multifocal presentation. To aid a diagnosis, the firstline recommended treatment was the bilateral enucleation of the cysts under general anaesthesia for histopathological analysis and genetic testing.
Figure 1. OPG September 2017 (sent with referral). An OPG radiograph showing bilateral, expansile multilocular lucencies of the mandible.Figure 2.
(a,b) CBCT scan from January 2018. This showed bilateral, expansile multilocular lucencies within the angle and ramus of the mandible, extending into the coronoid process on the left, approximately 2.9 cm antero-posteriorly. There was significant bilateral cortical thinning of the lingual and buccal cortices and a close association with the apical portions of the third molar teeth and inferior alveolar nerve canals bilaterally.
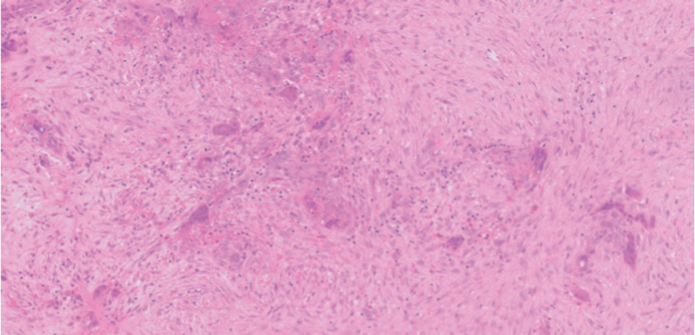
Histological examination of the enucleated lesions showed a proliferation of spindled fibroblasts set within a lightly collagenous stroma with admixed osteoclast-like giant cells and extravasated red blood cells (Figure 3). The fibrous component appeared waterlogged, a feature reported to distinguish cherubism from other giant cell jaw lesions. There was mild perivascular cuffing, which again supported this diagnosis.
Figure 3. Histology from the enucleated left mandibular lesion showing moderately cellular fibrous tissue with clusters of multinucleate giant cells. Extravasated erythrocytes and capillary vessels are also present (H&E, 200x).
Following the clinical and histopathological findings, a working diagnosis of cherubism was formed. Genetic testing was then undertaken to check for a mutation in the SH3BP2 gene, which is linked to cherubism, and subsequently to a panel of genes related to skeletal dysplasia. The results of genetic testing were negative to mutations in the SH3BP2 but positive to a mutation in the PTPN11 gene. This gene is associated with a group of conditions known as RASopathies and autosomal dominant syndromes such as Noonan syndrome, the latter of which can cause considerable morbidity if not treated appropriately.5 Familial genomic testing deemed the patient's mother to also have this mutation. The patient did not have typical features of RASopathies or Noonan syndrome, despite the genetic mutation.
The outcome from the rheumatology and clinical genetics multidisciplinary team meeting was that further paediatric cardiology and ophthalmology investigations were required. This was to rule out the presence of any other underlying PTPN11 mutation-related complications. The subsequent cardiac and ophthalmology results were unremarkable.
Upon the geneticist's recommendation, follow up with further investigations will be required. Labels of syndromes are usually not given with genetic sequences alone, but require positive results to screening investigations before a definitive diagnosis can be confirmed.6 Therefore, it was determined that the mandibular giant cell lesions were likely to be a manifestation of the PTPN11 genetic mutation, but the patient was not diagnosed with a syndrome typically associated with this mutation. It should be noted that outside RASopathies, the giant cell lesions would be termed cherubism. Therefore, the working diagnosis of cherubism remained, but it was acknowledged that the genetic mutation linked to the development of the bony lesions was not typically the one associated with cherubism.
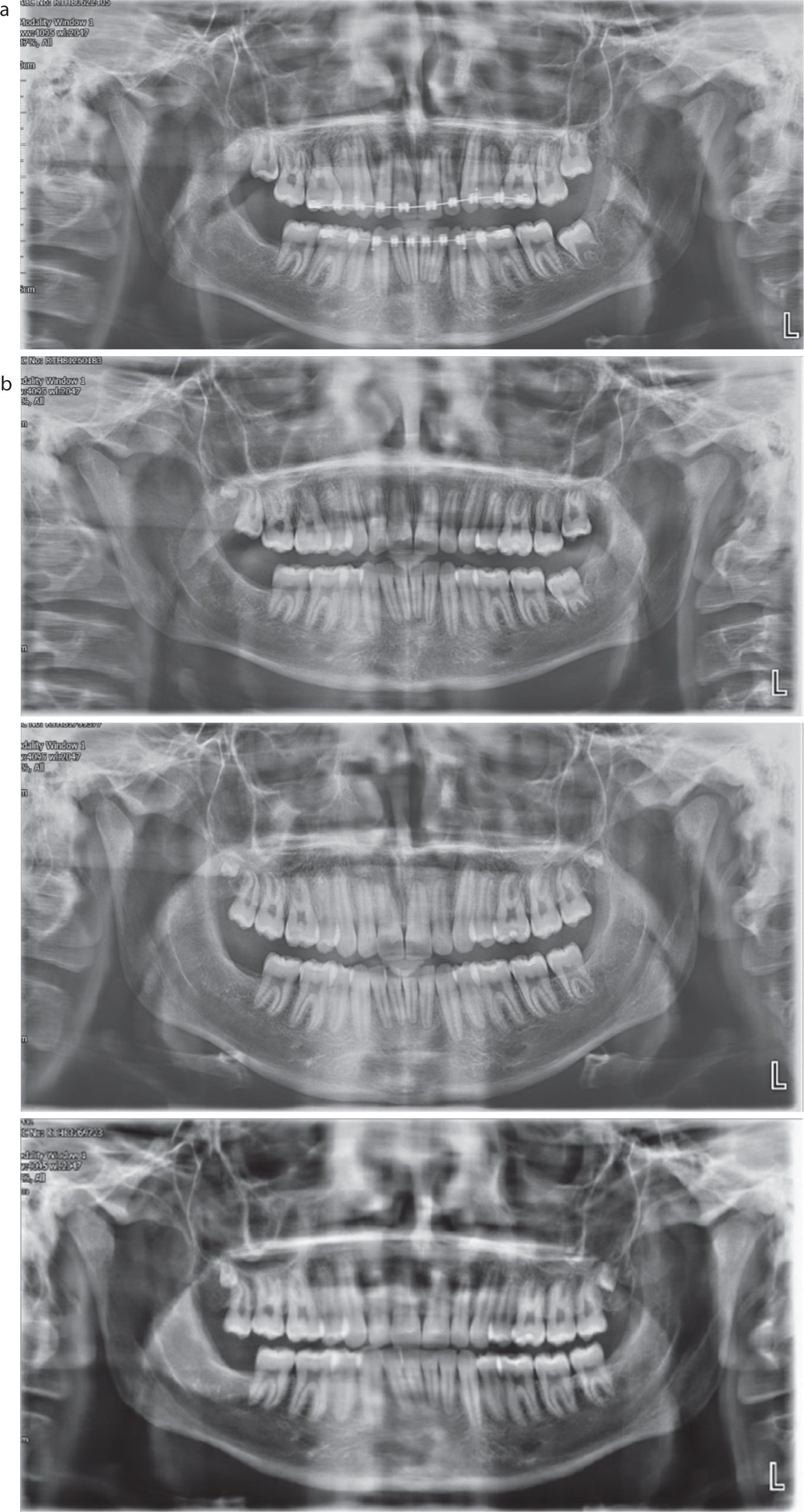
Further annual radiographic follow up were provided post-operatively, showing good bony infill in the areas of excision, no sign of recurrence and remission of the disease in line with puberty (Figure 4). The patient was therefore discharged back to the continued care of his general dental and medical practitioners.
Figure 4. Post-operative OPG radiographs showing involution of the lesions and remission of the bony lesions in line with puberty. (a) November 2018; (b) November 2019; (c) November 2020; (d) February 2023.
Discussion
In this case report, the initial clinical working diagnosis was that of cherubism following on from the clinical presentation, radiological and histopathological findings, which were consistent with this condition. However, this case highlights the need for a multidisciplinary approach, using findings from clinical, radiographic, histopathological, genetic and biochemical investigations, in order to confirm a diagnosis. Despite the fact that cherubism is most commonly associated with a mutation in the SH3BP2 gene, it cannot be excluded if this particular mutation is not found, owing to the possibility of genetic heterogeneity.4 Thus, patients may need to be tested for other genes implicated, mutations in which can be linked to several complications for which further follow up is required, as seen in this case.
Initially, the patient's multilocular radiolucencies were an incidental finding suspected to be cherubism owing to their bilateral expansile nature. Indeed, it is reported that in milder cases, cherubism may not be clinically evident and found incidentally. On the other hand, individuals with progressive forms of the disease may have several symmetrical mandibular lesions or multi-lesion involvement of both the maxilla and mandible, leading to severe facial abnormalities and enlargement.4 As a result, they may have complications with functional, social and psychological development.7
The complications associated with cherubism include problems with respiration and vision, functional challenges with speaking and swallowing, pain and psychosocial implications.2 Dental complications are also common and are discussed later. Respiratory complications can occur as a result of upper airway obstruction from the backward displacement of the tongue.8 This can lead to mouth breathing, snoring, chronic nasal infection and obstructive sleep apnoea.9 Ocular involvement can occur in conjunction with maxillary involvement. Individuals may experience lower lid retraction, proptosis, diplopia, globe displacement and loss of vision.10 Jaw enlargement is also reported to lead to challenges with chewing and swallowing, and pain upon eating.2
The psychosocial wellbeing of individuals with cherubism may be affected by the facial disfigurement they can experience. In addition, the individual may have concerns related to the genetic risk to future offspring or implications for other close family members. Familial genetic testing can be conducted to ascertain whether the mutation was inherited. If found to be inherited, genetic testing can then be extended to the patient's siblings, who may require subsequent investigations and management.
There are currently no standardized treatment protocols for cherubism. Depending on the severity, functional and aesthetic complications, maxillofacial surgical management is planned according to the individual's development of the disease.4 Therefore, the holistic and long-term rehabilitative management of a patient with cherubism often includes collaboration between primary care practitioners, paediatric dentists, orthodontists and maxillofacial surgeons. Within medicine, rheumatologists, geneticists, pathologists, cardiologists and ophthalmologists often play a significant role too.
Cherubism is considered to be a self-limiting condition because bone remodelling and regression occurs after puberty. Thus, in the second and third decade of life, complete resolution of the facial abnormalities is often seen.2 Therefore, a ‘watch and wait’ approach with regular observation and follow up is often adopted.7 Surgical intervention is indicated in severe cases involving nasal obstruction, deteriorated swallowing and respiratory functions, proptosis or gross facial deformity.11 Given the potential for new bony lesions to spontaneously re-occur or established lesions to enlarge up until puberty, surgical management is considered after growth completion.12 Corrective surgical procedures include tooth extractions in or around the bony lesions, partial resection, contour resection and curettage. It is recommended to conduct annual clinical and radiographic examination with follow up every 2–5 years as regression is reported well after adolescence.13
Relevance to GDP
Cherubism is known to be associated with multiple dental anomalies. The GDP should be aware of the extra- and intra-oral manifestations of the condition, and what types of dental interventions may be required at different stages of the condition. In an undiagnosed individual, the GDP may be the first person to incidentally notice clinico-radiographic features associated with the condition, playing a key role in the diagnosis of cherubism. For patients with cherubism, careful monitoring of the development of the dentition is required. This may involve solely longitudinal observation in milder cases that do not require dental intervention. In more severe cases, the GDP may be able to provide dental interventions for individuals with dental anomalies or post-surgery dental rehabilitation and surveillance.
General dentists should be aware of the abnormal radiographic presentation associated with cherubism. The bony lesions seen in cherubism tend to have well-defined, often corticated, borders that surround irregular trabecular bone. Radiographically, these can appear as expansive multilocular radiolucencies with thin cortices. This bony structure can lead to teeth being situated within an area of minimal supporting bone and radiographically, they can appear as ‘floating teeth’. 14 In these cases, the teeth may require extraction.
Alongside the extra-oral findings already discussed, lymph node enlargement has been reported in the early stages of cherubism. Enlarged submandibular nodes may be seen when the lower part of the face has swollen, which gives rise to a fuller appearance to the lower face.15 The enlarged nodes may be picked up in an extra-oral examination by the GDP and are described as feeling discrete, non-tender on palpation and mobile.16
Intra-oral anomalies seen in individuals with cherubism can range in type and severity depending on when the condition first affects the individual and the extent of the bony lesions. In the deciduous dentition, teeth may exfoliate prematurely and there may be a delayed eruption of the permanent teeth.16 In the permanent dentition, teeth may be impacted or crowded.14 Hypodontia is also reported, with the permanent molars being most commonly affected.17 Other dental findings include altered tooth morphology, ectopic eruption, partially resorbed roots and displaced teeth.14 The latter may be as a result of bony destruction occurring around the erupting permanent teeth. Impacted, ectopic teeth may require extraction.4 The potential dental anomalies can lead to individuals experiencing malocclusions of different severities, for which further orthodontic input may be required. This should be started once the patient's growth is completed and the bony lesions quiesce. Orthognathic surgical intervention has been reported in the literature as a feasible option for managing adolescents with severe skeletal deformities.18
The discrepancies in the maxillomandibular relationships, abnormal bone structures, hypodontia and tooth malposition can be prosthetically treated by use of removable prostheses. These can help to improve functional and aesthetic outcomes during craniofacial development.19 However, these prostheses may require adjustment over time as the individual grows, or the jaws undergo bony changes. This would include modifications including relining, rebasing or replacing the prostheses. Implants have also been reported to successfully restore the dental arch in a small number of cases; however, there is uncertainty as to the timing and long-term functional success of jaws previously compromised by cherubism.7
Conclusion
Clinicians should be aware of the potentially significant impact that cherubism poses to the craniofacial development, daily function and psychosocial wellbeing of paediatric patients affected by the condition. The diagnosis and management of individuals with cherubism requires input from multiple medical and dental specialties, most likely in a secondary or tertiary care setting. However, despite the specialist input required, initial suspicions of the condition are often detected incidentally in primary care.
In many cases, clinical and radiographic observation and surveillance without a need for surgical or other intervention is required. However, severe cases can require surgery to treat significant facial deformity, systemic complications and dental anomalies that can impact upon function and aesthetics. To ensure the success of treatment and absence of disease recurrence, long-term clinical and radiographic follow up is required.