Sarode GS, Sarode SC, Maniyar N Oral cancer databases: a comprehensive review. J Oral Pathol Med. 2018; 47:547-556 https://doi.org/10.1111/jop.12667
Tosheva G, Siderova M, Encheva E, Malinova D Thyroid metastasis of a squamous cell carcinoma of the tongue – a rare case report. J IMAB Annu Proc. 2021; 27:3564-3467 https://doi.org/10.5272/jimab.2021271.3564
Struller F, Senne M, Falch C Primary squamous cell carcinoma of the thyroid: case report and systematic review of the literature. Int J Surg Case Rep. 2017; 37:36-40 https://doi.org/10.1016/j.ijscr.2017.06.011
Deulkar S, Meena P, Radhika P Thyroid metastasis of squamous cell carcinoma in an unsuspected patient. J Cytol Histol. 2019; 10:(3)
Sapalidis K, Anastasiadis I, Panteli N Primary squamous cell carcinoma of the thyroid gland. J Surg Case Rep. 2014; 2014 https://doi.org/10.1093/jscr/rju133
Vatsyayan A, Mandlik D, Patel P Metastasis of squamous cell carcinoma of the head and neck to the thyroid: a single institution's experience with a review of relevant publications. Br J Oral Maxillofac Surg. 2019; 57:609-615 https://doi.org/10.1016/j.bjoms.2019.05.012
Syed MI, Stewart M, Syed S Squamous cell carcinoma of the thyroid gland: primary or secondary disease?. J Laryngol Otol. 2011; 125:3-9 https://doi.org/10.1017/S0022215110002070
Korovin GS, Kuriloff DB, Cho HT, Sobol SM Squamous cell carcinoma of the thyroid: a diagnostic dilemma. Ann Otol Rhinol Laryngol. 1989; 98:59-65 https://doi.org/10.1177/000348948909800113
Ai QYH, So TY, Hung KF, King AD Normal size of benign upper neck nodes on MRI: parotid, submandibular, occipital, facial, retroauricular and level IIb nodal groups. Cancer Imaging. 2022; 22 https://doi.org/10.1186/s40644-022-00504-z
Macpherson LM, McCann MF, Gibson J The role of primary healthcare professionals in oral cancer prevention and detection. Br Dent J. 2003; 195:277-281 https://doi.org/10.1038/sj.bdj.4810481
Metastatic Oral Cancer and the Importance of a thorough Neck Examination Prateek Biyani Jimmy Xu Mohammed Anabtawi Robert Orr Dental Update 2025 51:8, 550-554.
Authors
PrateekBiyani
BDS (Hons), MFDS RCPS(Glasg), Cert Med Ed, FHEA,
Specialty Doctor in Oral and Maxillofacial Surgery, Chesterfield Royal Hospital, Chesterfield
Squamous cell carcinomas (SCC) account for over 90% of oral cancers. Over the last few decades, there has been a significant increase in the number of cases. Metastasis of oral cancer to the thyroid is extremely rare. Rarer still are tumours metastasizing from the tongue to the thyroid. We present a case of a patient who presented to her dentist with a tongue SCC. Despite radical curative treatment, the tumour metastasized to the thyroid and the patient succumbed to the metastatic disease. We, additionally, highlight the importance of thorough lymph node and neck examination in the dental setting to help identify pathology in patients.
CPD/Clinical Relevance: The importance of a thorough lymph node and neck examination at routine dental check-ups is highlighted.
Article
In the UK, between 2016 and 2018, there were over 12,400 new cases of head and neck cancer, with 37% rise in incidence since the 1990s.1 Squamous cell carcinomas (SCC) account for over 90% of oral cancer cases.2 SCCs of the thyroid gland are extremely rare and may either be primary or secondary tumours, which are through either extension or metastasis of the primary tumour. Metastasis of oral SCC to the thyroid gland is exceedingly rare, with approximately 10 reported cases.3 Furthermore, there are only three reported cases of SCCs originating from the tongue metastasizing to the thyroid.3 The case presented highlights the risks of oral cancer with delayed metastasis. It also highlights the potential for a variety of pathology, including cancer, to present in the neck and the importance of dentists conducting effective lymph node and neck examinations to screen these patients.
Case report
A 60-year-old female was referred to the oral and maxillofacial surgery department by her general dental practitioner (GDP). She was an irregular attender and had been last seen 3.5 years prior to the attendance. She attended with pain, swelling and ulceration of the right side of her tongue. The pain had gradually worsened over a 2-year period, with significant deterioration in the previous 6 weeks. Her speech was also being affected.
She had hypertension and well-controlled type-2 diabetes mellitus. Her medications included metformin, bendroflumethiazide, ramipril and amlodipine. She had no allergies and was a non-smoker who consumed <10 units of alcohol per week.
On examination, there was evidence of a 2 x 3 cm ulcer on the right lateral border of her tongue, with obvious enlargement (Figure 1). This had evidence of rolled margins and contact bleeding. There were no palpable cervical/neck nodes.
Figure 1. Clinical presentation demonstrating a tumour on the right-lateral tongue.
Clinical staging involved imaging, including magnetic resonance imaging (MRI) of the neck, and computed tomography (CT) of the thorax. An incisional biopsy demonstrated a moderately differentiated squamous cell carcinoma (SCC).
The MRI demonstrated a tumour with a size of 38 mm in its maximum dimension, crossing the midline of the tongue and invading into extrinsic muscles. There were also two potential pathological nodes identified at right level I (submandibular/submental region) and level II (upper deep cervical chain), with suspicion of extra-nodal extension. This confirmed the presence of a T4aN2bM0 SCC of the right lateral tongue.
Following multidisciplinary team (MDT) discussion, curative treatment was planned including surgery and adjuvant radiotherapy. In preparation, the patient had a percutaneous endoscopic gastrostomy (PEG) fitted. Her surgery was subsequently carried out and involved:
Tracheostomy;
Bilateral neck dissection;
Subtotal glossectomy;
Reconstruction with an anterolateral thigh free flap.
Post-resection histology demonstrated a moderately differentiated SCC with a maximum diameter of 57 mm and a depth of invasion of 20 mm. It exhibited a discohesive pattern of invasion with extensive perineural invasion. There was one positive level III node on the right, while no node involvement was identified on the left. This confirmed a pathological staging of T4aN1M0 (TNM-7) or T3N1M0 (TNM-8) SCC of the right lateral tongue. Adjuvant radiotherapy was completed.
The patient had a relatively uneventful recovery and attended her routine oncology appointments. She continued to gain weight and demonstrated improving physical fitness, including walking up to 10 miles per day.
Two years later, she attended complaining of increasing shortness of breath (SOB) that had developed over the previous 2 weeks. She had been prescribed salbutamol and becotide inhalers by her general medical practitioner with limited benefit. She had also noticed her voice becoming husky and was having to sleep on three pillows owing to breathing difficulties. On clinical assessment, there was a marked inspiratory wheeze and flexible naso-endoscopy demonstrated laryngeal oedema with left vocal cord palsy. There was also asymmetry of her neck.
An MRI (Figure 2) demonstrated a new, ill-defined left thyroid nodule invading strap muscles and pushing on the trachea. She was prescribed dexamethasone to help manage the swelling and biopsies were taken.
Figure 2. Axial view of MRI demonstrating the patient's encased and narrowed trachea.
The biopsies indicated a poorly differentiated SCC. Following MDT discussion and correlation with clinical and radiological findings, it was determined that this was a metastatic SCC from the original tumour. This was determined unsuitable for surgical removal owing to multiple factors, including the size and extension of the tumour into surrounding structures. A surgical airway was not deemed feasible because the tumour had encased and compressed the trachea (Figure 2), with no method of access without navigating through tumour. Palliative treatment, including chemotherapy, was proposed to the patient and, during an accident and emergency (A&E) department attendance owing to SOB, a ‘do not resuscitate’ (DNR) form was signed. She was given an emergency drug kit of midazolam and morphine in case of an airway emergency.
She attended A&E with worsening SOB and reduced consciousness a few months later. Sadly, she passed away the following day owing to the metastatic disease.
Discussion
SCCs involving the thyroid are extremely rare. Primary SCCs account for less than 1% of all primary thyroid cancers.4 Metastasis of SCCs to the thyroid are more common than a primary thyroid SCC, with an incidence of up to 1.1%.5 However, tongue SCC metastasizing to the thyroid is considerably rarer, with the number of reported cases in single digits.3 The aetiology of oral cancer is well understood, with major risk factors including tobacco, alcohol and, more recently, human papillomavirus.6 However, the aetiology behind the development of SCCs in the thyroid is not fully understood. For primary SCCs, there are numerous theories, including the embryonic nest theory that suggests remnants of the thyroglossal duct or thymic epithelium may lead to the development of the SCC.7 Generally, the thyroid is resistant to metastatic tumour development owing to its abundant and fast blood flow, the high iodine content and the hyperoxic environment. Secondary involvement of the thyroid could be a result of direct invasion, lymphatic or haematogenous spread.5 Additionally, it has been suggested that metastasis is more likely in an already abnormal thyroid, where blood flow is slowed.8 Our patient had no history of thyroid pathology and re-staging scans did not identify any other tumours.
Clinical presentation of metastatic SCCs to the thyroid can vary. As in our patient, extra-orally, there may be nothing significant to note. Some patients may present with an obvious thyroid nodule or lymph node involvement, hence the importance of a thorough neck examination as discussed later.5 Symptoms of more aggressive disease include dysphagia, dyspnoea, stridor and hoarseness of voice.8 Diagnosis is typically achieved through a combination of clinical findings, biopsy and imaging. Fine needle aspiration of the thyroid can be carried out to determine the nature of the mass. If malignant squamous cells are identified, then metastasis should initially be suspected over a primary thyroid SCC.5 Ultrasound is beneficial as primary imaging to help differentiate between a benign or malignant lesion.8 CT and MRI scans can be used in conjunction to help identify the extent of the thyroid mass and its association with surrounding anatomy.
Treatment of metastatic thyroid SCC is poorly documented, extremely challenging and outcomes are generally very poor, although the prognosis is poorer with primary thyroid SCCs.9 Surgical resection is the mainstay of management. However, much like our patient, many of these patients have a history of radiotherapy to the head and neck. This leads to severe fibrosis of the tissues in the treatment field, with vital structures adhering to each other. Subsequently, surgical resection becomes technically difficult.8 In our case, the disease was too aggressive and too advanced for this to be an option. There is a lack of evidence with regards to the use of chemotherapy or radiotherapy in this scenario. Despite this, studies do demonstrate that the thyroid is relatively radio-resistant and has a poor response to chemotherapy.7 This would suggest that currently these treatment modalities would have only a limited benefit, if any. Radiotherapy and chemotherapy may provide some palliative benefits; however, these too are extremely limited.8
For primary thyroid SCCs, survival rates are extremely poor with a median survival of 12 months or less.9 The data on survival relating to metastatic disease to the thyroid, particularly based on tumour site and size, is not as substantial, but suggests potentially more favourable survival rates.9 When specifically looking at tongue-related metastasis, there are only two studies showing median survival of 62 and 182 months.8,9 The more favourable survival rates may be associated with the secondary tumours being more radio-sensitive than primary tumours.10 Aside from routine oncology follow-up for these patients, dental appointments are often the only other regular healthcare contact they have. As part of a routine dental examination, it is increasingly important that dentists complete a thorough lymph node and neck examination. The National Institute for Health and Care Excellence (NICE) has extensive guidelines on diagnosing neck lumps, which includes a systematic method to assess a patient's neck.11 Additionally, the NICE guidelines highlight the array of causes for neck lumps in patients, including the variety of benign causes.11 Examples of causes for neck lumps include, but are not limited to:
Lymphadenopathy;
Benign tumours, for example of the submandibular glands;
Thyroid pathology;
Cysts, for example branchial cleft cysts;
Congenital and developmental lumps.
As dentists, we should not just aim to look for malignant lumps in the neck, but also try to identify any other pathology that may be present. By following a quick and systematic neck examination, GDPs may be able to identify primary or metastatic cancers presenting in the neck, including the thyroid, as well as other benign pathology. Effective assessment of the neck starts with thorough visual examination for any swellings, deformities or asymmetries. Following this, thorough palpation of the neck is vital, as outlined by the NICE guidance.11
Assess the anterior triangle of the neck: this is from the midline of the neck, to the anterior border of the sternocleidomastoid and the body of the mandible. The thyroid is partly situated in this triangle.
Assess the posterior triangle of the neck: this is bordered by the posterior border of the sternocleidomastoid, trapezius and clavicle.
Assess the midline of the neck, which includes the bulk of the thyroid gland.
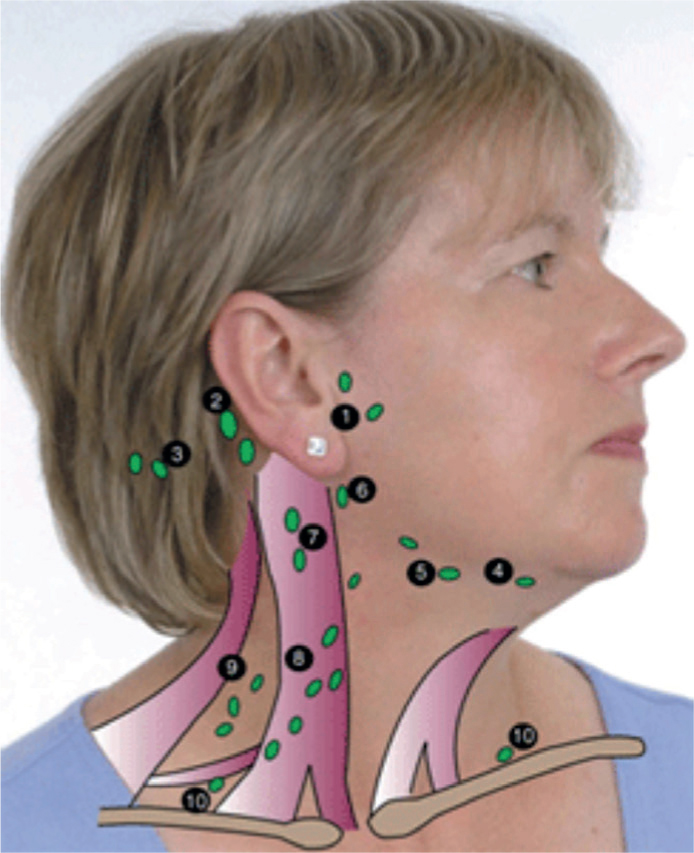
Palpation should be carried out with the fingertips and relatively firm, circular motions. A systematic approach is crucial to ensure everything is assessed for every patient. An example is outlined in Figure 3, with palpation starting in the pre-auricular area, working to the anterior triangle and then the posterior triangle.12 There are important factors that help to identify and differentiate between potentially malignant pathology and benign pathology, which include:11
Size: it is generally considered that a lymph node ³10 mm in size is suspicious and should be investigated further.13
Tenderness: the presence of pain generally indicates an infectious or inflammatory cause.
Mobility: if the lump is fixed to surrounding structures, this may be suggestive of a malignancy, including extra-nodal extension from a lymph node.
Texture: hard and irregular lumps are more suspicious for malignancy, while compressible and soft lumps are likely to be benign, such as cysts.
Figure 3. An example of a systematic approach to neck examination.
Other factors worth assessing and considering include any movement of the lump when swallowing or protruding the tongue, as well as the nature of the overlying skin.11 Identification of pathology in the neck should prompt a GDP to consider appropriate referral to their local oral and maxillofacial surgery unit as either a routine, an urgent or a suspected cancer referral.
It is generally understood that confidence among GDPs to carry out oral cancer screening and examination is limited, with around 37% stating they were confident to screen for oral cancer.14 Additionally, only 58% of GDPs stated that they carry out routine oral cancer screening, something that we should be carrying out for every patient.14 There is a lack of research into the confidence of GDPs to carry out a comprehensive neck examination; however, based on confidence with intra-oral examinations, it can be assumed that the confidence and frequency of neck examinations is low.
Conclusion
This case demonstrates a rare phenomenon of metastasis of SCC from the tongue to the thyroid gland. Any symptoms that may be suggestive of thyroid involvement should prompt immediate investigation, including biopsy and imaging, specifically to help differentiate between a primary thyroid SCC and a metastatic SCC. Any involvement of the thyroid is an incredibly difficult clinical scenario to manage and, unfortunately, there are limited treatment options for patients, particularly with advanced disease. As GDPs, we carry a responsibility to be part of the screening process for patients to identify primary or metastatic disease within the neck, along with other pathology. This is achieved through thorough and systematic examination of the neck.