References
Necrotizing sialometaplasia – a diagnostic conundrum
From Volume 45, Issue 5, May 2018 | Pages 457-461
Article

Salivary gland diseases are one of the most diverse lesions encountered within the oral cavity by head and neck practitioners. With numerous differential diagnoses on board,1 this report aims to highlight the importance of obtaining a thorough medical history and increasing awareness of the clinical presentation of necrotizing sialometaplasia to healthcare professionals. NS is a benign, inflammatory, self-healing condition often misdiagnosed as malignancy,2 therefore the importance of a correct diagnosis and subsequent treatment is imperative.
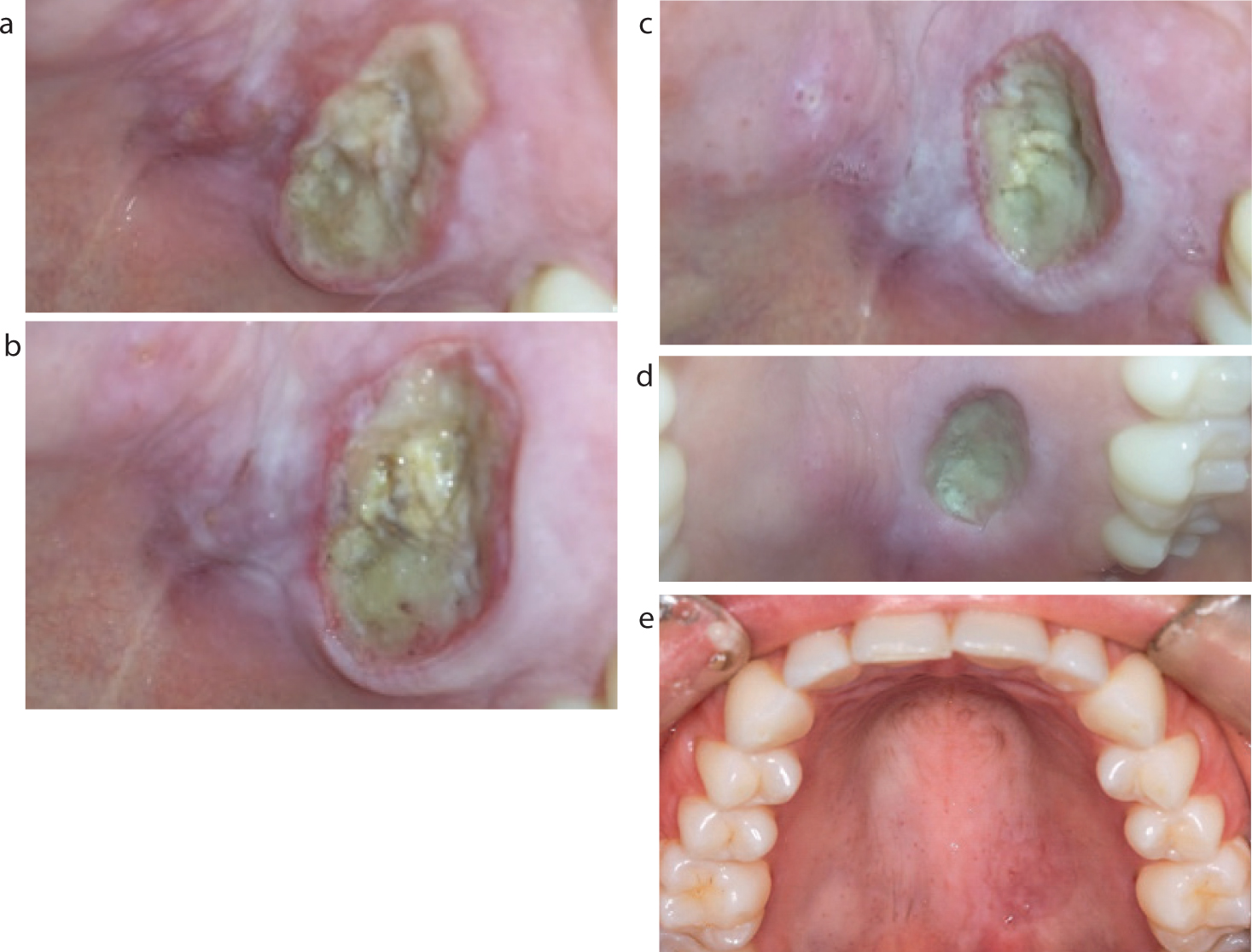
This case report documents the presentation and natural history of this benign tumour-like lesion of the hard palate in a 27-year-old female with digital pictures captured from the patient's own smartphone, which show the lesion from presentation through to the healing stage.
Case report
A 27-year-old female presented to the hospital with a 5-day history of a painful swelling on the left of the midline of the hard palate, which appeared spontaneously and was intensely painful on eating. Clinical examination showed a deep necrotic ulcer with a surrounding erythematous halo measuring 2.5 cm by 2cm in diameter (Figure 1a). The cervical lymph nodes were palpable on both sides. The only relevant history included a previous diagnosis of bulimia.
The patient underwent a series of different imaging, including an MRI and ultrasound scan (Figure 2) showing diffuse thickening of the hard palate and deep ulceration.

An incisional biopsy of the lesion showed ulcerated mucosa covered with hyper-parakeratotic and hyperplastic stratified squamous epithelium. The mucosalivary glands showed acinar atrophy carrying degrees of lobular necrosis within the granulation tissue and mixed acute and chronic inflammatory cell infiltrate (Figure 3). The histopathological appearances were consistent with NS.

The patient was followed up weekly and prescribed metronidazole and chlorhexidine mouthwash to help prevent further infection, cleanse and reduce the pain of the ulcer. Follow-up was managed conservatively and the lesion regressed completely after 6 weeks (Figure 1e).
Method
This case report principally focused on primary research of reports undertaking a response to specific key words related to NS.
Types of studies considered in this review
Search strategy for identification of studies
Databases PubMed and Ovid Medline (1946 to December week 1 2016) were reviewed and references from each retrieved article were also considered and handpicked according to the most frequently cited journals.
Figure 4 discusses the selection criteria, method and number of articles sought using our search criteria via PRISMA. In order to obtain up-to-date information, the search strategy used a combination of key words including: necrotizing sialometaplasia, bulimia, oral cavity and smartphone. Databases used during the search criteria were limited to English language articles only and peer reviewed published literature. Research from non-human studies and published case reports dating pre-2006 were not included in the literature review.

Discussion
Necrotizing sialometaplasia is a rare inflammatory condition, which can present differently from other more common inflammatory lesions of the oral cavity. The pathogenesis has been described as five distinct histologic stages:
Features which are helpful in differentiating NS of the hard palate have been reported by Abrams et al when the first case of NS was published.1 These include crater-like ulcerations, a surrounding red halo and ragged edges around the lesion. Prominent granulation tissue and inflammatory components, metaplasia of salivary ducts and mucous acini and lobular infarction are histological features that are most helpful in the differentiation of NS from neoplastic lesions. Kaplan et al cite potential differential diagnoses that should be considered, including zygomycosis, Wegener's granulomatosis and malignancies such as squamous cell carcinoma and mucoepidermoid carcinoma.2,3
The aetiology of NS remains a mystery, however, ischaemia has long been considered to be the most probable explanation linking the presentation of salivary gland necrosis and ulceration of the overlying mucosa.4 The risk factors associated with onset of ischaemia include localized trauma during tooth extractions, an iatrogenic trauma, eg intubation, poor-fitting prostheses leading to compression of the palate, smoking, alcohol ingestion and the use of recreational drugs such as cocaine that can decrease blood flow to the mucosa.4 There has also been one report of NS associated with the use of a topical non-steroidal anti-inflammatory drug.4
In this case report, none of the above risk factors was applicable, however, the patient admitted to suffering from bulimia approximately one year previously. There have been reports of NS in females between the ages of 29–32 years with a history of bulimia5 (Table 1). Bulimic patients will often induce vomiting by pushing their fingers onto the palate to induce the gag reflex and provoke vomiting. This leads to chemical irritation resulting from chronic vomiting and low pH gastric contents, along with the trauma sustained by the palate that can induce arteriosclerotic changes, leading to ischaemia.6 Due to the lack of reporting and documentation of NS, an established definitive cause cannot be concluded, however, the reader should bear these contributory factors in mind when taking a thorough history.
| Case | Age/Sex | Biopsy | Histopathological Diagnosis | Treatment |
|---|---|---|---|---|
| Kaplan et al2 | 33/F | Incisional | NS | Observation |
| Diane & Carlson5 | 32/F | Incisional | 1st – Mucoepidermoid carcinoma |
Surgical resection owing to histopathologic misdiagnosis |
| Bascones-Martinez et al7 | 21/F | Incisional | NS | Observation |
| Solomon et al8 | 32/F | Excisional | 1st – Mucoepidermoid carcinoma |
Additional resection owing to histopathological misdiagnosis |
| Tomoaki & Michizawa9 | 26/F | Incisional | NS | Observation |
| Present case | 27/F | Incisional | NS | Antibiotics & chlorhexidine |
Necrotizing sialometaplasia does not usually recur and the condition usually completely regresses following risk factor removal within 6–8 weeks. Lesions that fail to resolve should be reassessed for accurate diagnosis and treatment. In this case, the patient reassured the clinicians that the bulimia was under control after seeking psychological therapy.
Mobile technology has begun to play a popular role within the developed world and medicine has been no exception to this trend. Smartphones are one of the most ubiquitous and dynamic trends in communication within medicine, allowing both therapeutic and non-therapeutic purposes to be followed, including research, education and clinical photography. This allows patients to capture and photograph suspected lesions from their presentation through to the healing process (Figure 1e). The key word ‘Smartphone’ was incorporated into our search criteria, however, no results or documentation associated with NS was found. This is the first known case report to document the natural history of this condition through clinical imagery by utilizing images captured and recorded from the patient's own smartphone. Clear chronological photographs in this case report, demonstrating the lesion from presentation, to progression, up to regression, enables healthcare professionals to familiarize themselves with the clinical presentation of NS from early onset. However, the limitations associated with this unanimous trend, including distortion of photographs, poor quality imaging and lack of clinical information must be borne in mind; especially when assessing the severity of a condition, which may lead to incorrect clinical judgement, further potentiating a diagnostic conundrum.10
Summary
The presentation of a non-healing palatal ulcer with a short onset in a young adult patient with a history of bulimia should increase suspicion for NS. The images provided in this case report, documenting the natural history of the condition, can act as a reference to anyone who is suspecting this diagnosis. Ultimately, histopathological examination is necessary in cases of NS as the clinical features of this condition can mimic other diseases, particularly salivary gland tumours.