Article



Specialist referral may be indicated if the Practitioner feels:
Radiolucencies (Tables 1–3)
| Procedure | Advantages | Disadvantages | Remarks |
|---|---|---|---|
| Aspiration | Simple using 18 gauge needle | May introduce infection | May confirm haemangioma. Cyst fluid protein content may be diagnostic (Protein levels <4g% in keratocysts) |
| Bone biopsy | Definitive | Invasive | Most commonly used |
| Bone scan | Surveys all skeleton | Those of any isotope procedure | Reveals areas of increased bony turnover, eg metastases; lacks specificity |
| Endoscopy (fibre-optic) | Simple; good visualization | Skill needed | Examines nasal passages, sinuses, pharynx and larynx but not widely available |
| Imaging | Reveals data not obvious on clinical examination | Specialized techniques may be difficult or expensive. Cone beam CT (CBCT) is becoming more widely used and available | See Table 2 |
| Region required | Standard views | Additional views |
|---|---|---|
| Facial bones | OM | Zygoma |
| OM 30 | Reduced exposure SMV | |
| Lateral | ||
| Mandible | DPT | Lateral obliques |
| PA mandible | ||
| Mandibular occlusal | ||
| Maxilla | OM for maxillary antra |
Upper occlusal or lateral SMV |
| DPT, tomography | ||
| Endoscopy | ||
| Nasal bones | OM 30 | |
| Lateral | ||
| Soft tissue lateral | ||
| Skull | PA 20 | SMV |
| Lateral | Tangential | |
| Townes (1/2 axial view) | ||
| Temporomandibular joints | DPT (mouth open and closed) |
Transpharyngeal – rarely used |
| Arthrography – almost obsolete | ||
| Reverse Townes | ||
| Consider MRI if the position of the disc is required/CT scan/cone beam CT to show abnormalities of the condylar heads or fractures |
| Lesion | Average age presentation | Gender predilection | Site and other comments |
|---|---|---|---|
| Nasopalatine duct cyst | 40–60years | M>F 4:1 | 1% of population. |
| Radicular cyst | 20–60 years | M>F 3:2 | 3x maxilla: mandible |
| Dentigerous cyst | <20 years | M>F 2:1 | L8; U3; L5 |
| Paradental cyst | 4–62 years | M = F | 93% mandible |
| Keratocystic odontogenic tumour | 20–40 years | M>F 1.7:1 | 80% mandible |
| Lateral periodontal cyst | 40–70 years | M>F 2:1 | 76% L3; L4&5; U2 teeth vital |
| Central giant cell granuloma | 60% <20 years | F>M 2:1 | Mandible anterior to 1st molar 2x maxilla |
| Aneursymal bone cyst | 90% <30 years | F>M slight | Mandible>Maxilla 3:2 molar region |
| Central haemangioma | <20 years | F>M 2:1 | Mandible>Maxilla |
| Arterio-venous malformation | 10–25 years | F>M | Mandible>maxilla |
| Solitary bone cyst | <20 years | M>F? M = F | 95% mandible |
| Stafne cavity | >40 years | M>F | Seen on up to 1% of DPTs. Lower 7 to angle of mandible below ID canal |
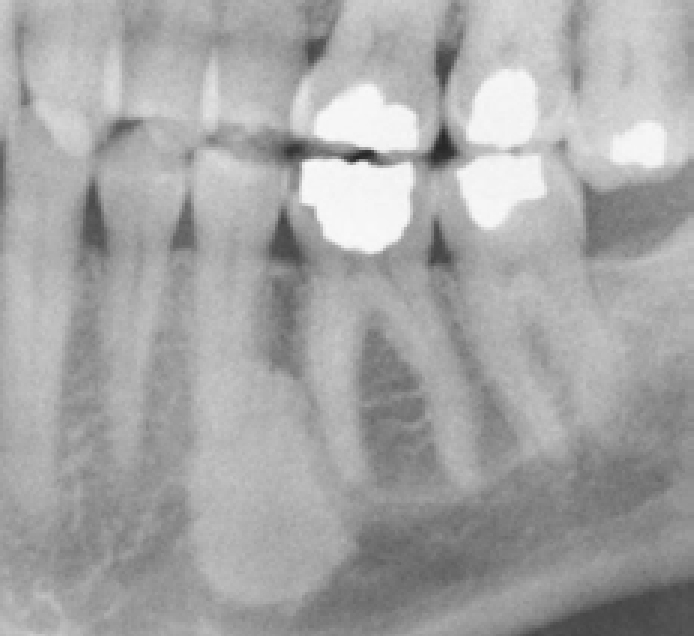
Radiographic features to be assessed include the lesional size, site, shape, margins, radio-density and effects on adjacent structures (displacement of the inferior alveolar nerve or tooth displacement or resorption).
Well-defined corticated radiolucencies are often odontogenic cysts and benign tumours as they are generally slow growing and allow the bone surrounding them to remodel. If they become infected cortication may be lost and they may appear to be less well defined.
Well-defined non-corticated lesions (punched out lesions) may be odontogenic cysts, granulomas that have become infected, or more sinister rapidly-growing lesions such as multiple myeloma, malignancy or histiocytosis.
Poorly defined radiolucencies are often infections or malignant tumours.
Jaw radiolucencies may include:
Giant cell lesions such as the Central Giant Cell granuloma – initially a small, unilocular radiolucency – eventually become multilocular, and may then mimic brown tumours of hyperparathyroidism (histologically similar). Biochemistry distinguishes these entities. Other giant cell lesions include brown tumour of hyperparathyroidism, cherubism and aneurysmal bone cysts.
Vascular or neurogenic lesions include:
Metabolic disorders include:
All cause a loss in bone density making radiographs appear over-exposed and there is also loss of corticomedullary differentiation (loss of lamina dura, outline of maxillary antrum, ID canal tramlines).
Neoplastic lesions include:
Radio-opacities
Radio-opaque lesions may be either of soft tissue origin or bony origin and therefore require localization with radiographs taken from two different aspects, and include:

Primary non-odontogenic tumours, eg prostatic carcinoma and breast metastases are occasionally radio-opaque. Sarcomas can cause osteolytic or osteoblastic lesions.
Mixed radiolucent and radio-opaque lesions
Mixed radiolucent and radio-opaque lesions are mainly fibro-osseous lesions, inflammatory processes (eg osteomyelitis, actinomycosis, osteonecrosis) and, less commonly, odontogenic tumours (mainly adenomatoid odontogenic tumour and calcifying epithelial odontogenic tumour). Florid osseous dysplasia is one of the commonest causes of multiple radio-opacities of the tooth-bearing area of the jaws.