Yi S, Bhate C, Schwartz RA. Sweet's syndrome: an update and review. G Ital Dermatol Venereol. 2009; 144:(5)603-612
Ginarte M, Toribio J. Sweet's syndrome. Med Clin (Barc). 2009; 133:(1)31-35
Hospach T, von den Driesch P, Dannecker GE. Acute febrile neutrophilic dermatosis (Sweet's syndrome) in childhood and adolescence: two new patients and review of the literature on associated diseases. Eur J Pediatr. 2009; 168:(1)1-9
Femiano F, Gombos F, Scully C. Sweet's syndrome: recurrent oral ulceration, pyrexia, thrombophlebitis, and cutaneous lesions. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 2003; 95:(3)324-327
Notani K, Kobayashi S, Kondoh K, Shindoh M, Ferguson MM, Fukuda H. A case of Sweet's syndrome (acute febrile neutrophilic dermatosis) with palatal ulceration. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 2000; 89:(4)477-479
Oral ulceration in newly diagnosed leukaemic patient with undiagnosed sweet's syndrome Daniel Brierley David N Slater John Snowden Debbie Holt Anne Hegarty Dental Update 2025 42:6, 584-585.
Authors
DanielBrierley
BDS(Hons), MFDS
BDS (Hons), MFDS RCS (Ed), MFDS RCS (Eng), FRCPath, PhD, SFHEA, Senior Clinical Teacher and Honorary Consultant in Oral and Maxillofacial Pathology; School of Clinical Dentistry, University of Sheffield
Sweet's syndrome is a relatively rare but important skin condition which can affect the oral cavity. Awareness of this reactive condition is important for dentists who work in hospitals, where it is most likely to present. This report summarizes one such case and aims to introduce the reader to Sweet's syndrome.
CPD/Clinical Relevance: Oral ulceration is a common condition occurring in medical inpatients for which oral and maxillofacial surgery and medicine senior house officers and specialists are often asked to review on the ward. An awareness of Sweet's syndrome is important as it is most likely to occur in this setting and may present with oral ulceration.
Article
Case report
In early 2011, a 53-year-old female patient with a 3-week history of oral ulceration was referred to Oral Medicine from Haematology at the Charles Clifford Dental Hospital. There was no history of ulceration before this episode. A few weeks previously she had presented to another hospital with a sore throat and skin lesions on her face, neck, legs and forearms. The patient had also been aware of ulcers on her palate and throat during this period. At this time, a full blood count showed haemoglobin to be 7.6g/dL, a raised WCC count of 48.9 x 109/L and neutrophil count of 22.5 x 109/L with blast cells on blood film examination (0.56 X 109/L). She had pyrexia during the following weeks, constant leukocytosis and low platelets ranging from 7 to 134 x 109/L. After extensive work-up she was diagnosed as having acute leukaemia.
Her previous medical history revealed that she had controlled hypertension and asthma, with an allergy to penicillin. She was a non-smoker and drank a minimal amount of alcohol. She worked as a school teacher and was married with two children.
Clinically, the skin lesions appeared as erythematous palpules and nodules (Figure 1). They were tender and well-circumscribed with a variation in size from 1–1.5 cm in diameter. Owing to the associated crusting, a working diagnosis of herpes zoster infection was made and a course of acyclovir started. However, a specialist dermatological review revealed the clinical presentation of the plaques to be inconsistent with herpes zoster infection, which was later confirmed by negative swab results. Therefore, a skin biopsy was arranged.
Figure 1. Erythematous papules on forearm.
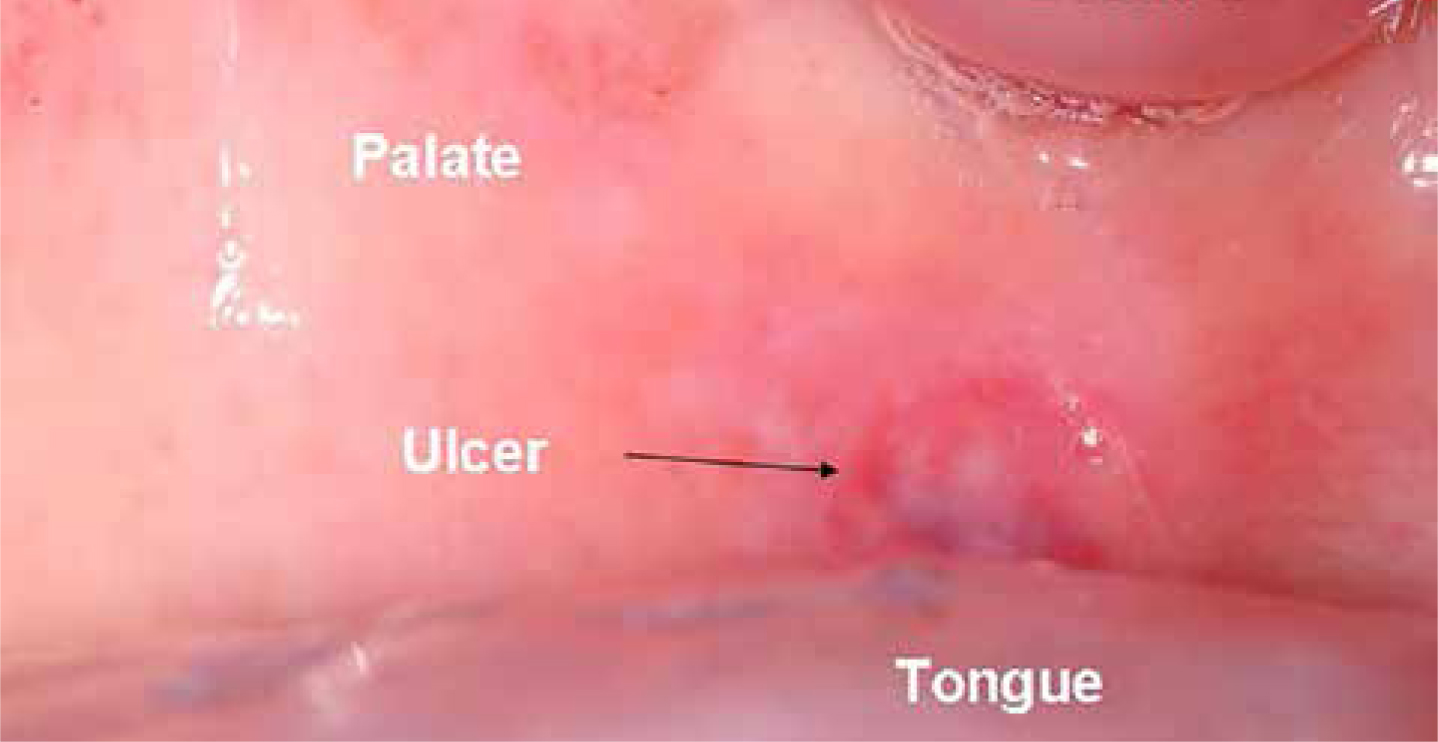
Intra-oral examination revealed a 1.5 cm ulcer on the soft palate (Figure 2). Treatment commenced with benzydamine hydrochloride 0.15% mouthwash which allowed the patient to drink and eat more easily. The possibility of whether the oral and skin lesions were consistent with Sweet's syndrome was raised at this point by the Oral Medicine consultant. This was confirmed by the skin biopsy results which revealed a dense infiltrate of neutrophils in the dermis, which conformed to a neutrophilic dermatosis such as Sweet's syndrome.
Figure 2. Ulcer on soft palate.
The patient was commenced on 40 mg prednisolone once daily, which was gradually reduced over the following weeks and led to a complete resolution of the skin and oral lesions. The patient subsequently received two cycles of intensive chemotherapy and bone marrow stem cell transplantation. She is currently stable with no recurrence of Sweet's syndrome following initial treatment.
Oral ulceration can also occur commonly in leukaemia but the concurrent skin lesions, which were proven to be part of Sweet's syndrome, would increase the likelihood of the oral ulceration also being a manifestation of this process. Oral biopsy was not performed because a skin biopsy had already proven the patient to have Sweet's syndrome and the ulcers responded well to benzydamine hydrochloride 0.15% mouthwash.
Comment
Sweet's syndrome or acute febrile neutrophilic dermatosis was first described by RD Sweet1 as an unusual and reactive dermatologic disorder that may serve as a marker of haematological malignancy, other malignancy or another serious systemic disorder,2 such as infection, inflammatory bowel disease and auto-immune disorders.3 In the case we have described, the underlying cause was known to be acute leukaemia.
Aetiology is felt to represent a manifestation of altered immunologic reactivity,4 but may be multifactorial with a preferential role for cytokines.5
Sweet's syndrome is characterized by the sudden eruption of tender discrete erythematous nodules or plaques, which are sometimes associated with fever, neutrophilic leukocytosis and a dense dermal infiltrate of mature neutrophils.2 The lesions are mainly observed on the arms, neck and face.2 The gold standard of treatment is systemic corticosteroids,2 but lesions may resolve spontaneously without therapeutic intervention.5
Oral ulceration in connection with Sweet's syndrome has previously been reported, including a case involving the skin and palate.5 The ulcers healed within 15–20 days and were associated with pyrexia and leukocytosis. Biopsy of the oral ulcers confirmed a dense, perivascular neutrophilic infiltrate, without vasculitis, consistent with Sweet's syndrome. The patient was treated with systemic prednisolone and oral cyclosporine for 1 month, and a dramatic improvement was noted. Another case,6 involving the palate, shared the same histological features and was treated with a reducing parenterally administered dose of prednisolone. Marked improvement was seen within a month and no recurrence was noted in the following 2 years, but recurrences have been seen to occur in 30% of patients.6
Conclusion
We report a case of Sweet's syndrome simultaneously presenting with skin and oral lesions and acute leukaemia in a previously well 53-year-old female. Dentists working in hospital, and especially those working in oral and maxillofacial surgery and medicine, may need to review medical inpatients with oral ulceration. An awareness of Sweet's syndrome is beneficial as it is most likely to occur in this setting and many dentists will not be familiar with it.