Carrol MJ. Spontaneous fracture of the genial tubercles. Br Dent J. 1983; 154:(2)47-48
Youngs R, Albert D. Fractured genial tubercles. J Laryngol Otol. 1984; 98:1047-1048
Santos-Oller JM, Junquera Gutierrez LM, De Vicente Rodriguez JC, Pendas SL. Spontaneous fracture of hypertrophied genial tubercles. Oral Surg Oral Med Oral Pathol. 1992; 74:28-29
Burnett CA, Clifford TJ. A case of fractured genial tubercles. Dent Update. 1993; 20:(5)
Shohat I, Shoshani Y, Taicher S. Fracture of the genial tubercles associated with a mandibular denture: a clinical report. J Prosthet Dent. 2003; 89:232-233
Yaedu RYF, Rubira-Bullen IRF, Sant'Ana E. Spontaneous fracture of genial tubercles: case report. Quintessence Int. 2006; 37:737-739
Gallego L, Junquera L, Villarreal P, de Vicente JC. Spontaneous fracture of the mandibular genial tubercles. A case report. Med Oral Patol Oral Cir Bucal. 2007; 12:(8)599-601
Bays RA. The pathophysiology and anatomy of edentulous bone loss. In: Fonseca RJ, Davis WH (eds). Philadelphia: WB Saunders;
Regional Maxillofacial Unit, University Hospital Aintree, Liverpool, UK and Edge Hill University, Liverpool and Evidence-Based Practice Research Centre (EPRC), Faculty of Health, Edge Hill University, St Helens Road, Ormskirk
Spontaneous fracture of the genial tubercles is rare and, of the 13 reported cases in the literature, all involve the older edentulous patient. A case of genial tubercle fracture in a 62-year-old edentulous female is presented. The symptoms are pain and swelling of the floor of the mouth and restricted tongue movement. Surgical intervention was not required and a complete recovery without loss of function was made.
Clinical Relevance: This case aims to make practitioners aware of genial tubercle fracture as a possible diagnosis when the older edentulous patient presents with pain and swelling in the floor of the mouth.
Article
Peter J Burnett, Paul P Nixon and Professor Simon N Rogers
The genial tubercles are a pair of bony projections, which are situated on the lingual surface of the anterior mandible, midway between the superior and inferior borders. These projections are part of the origin of the genioglossus and geniohyoid muscles.
Although usually quite small, the genial tubercles can increase in size and extend inwards from the lingual surface of the mandible, which can interfere with the seating of the lower denture.
Case report
A 62-year-old edentulous woman presented with pain and swelling of the floor of her mouth which affected her ability to swallow and also wear her lower denture. There was no relevant medical history and she had worn complete dentures for the past 30 years.
While eating, 4 days previously, she heard a cracking noise which was followed by severe pain. This lasted through the night but was eased by analgesics.
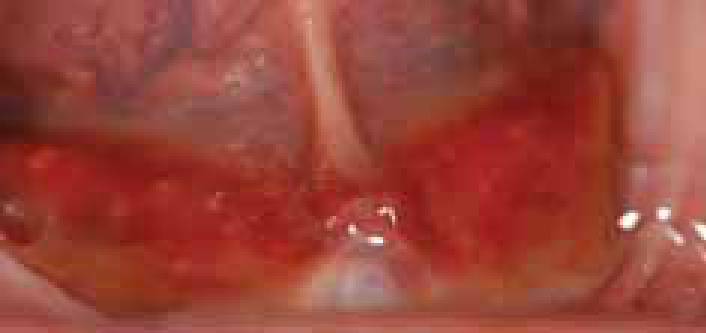
On examination, there was bilateral swelling and haematoma of the floor of the mouth (Figure 1). The submandibular salivary ducts were patent, salivary secretion was normal and there was a full range of tongue movement.
Figure 1. View of floor of patient's mouth showing bilateral swelling and haematoma.
A panoramic radiograph was taken which showed gross atrophy of the anterior mandible (Figure 2), and an occlusal radiograph revealed a radio-opaque body in the midline 3 cm distal to the lingual border of the anterior mandible (Figure 3). The possibility of a sialolith was considered but was ruled out owing to the midline position of the radio-opacity and the absence of any salivary gland swelling. A diagnosis of fracture of the genial tubercles was made.
Figure 2. Panoramic radiograph showing gross atrophy of the anterior mandible.Figure 3. Occlusal radiograph showing the fractured genial tubercle.
The patient was reassured and advised to continue taking analgesics. At her review appointment 3 days later, the swelling and inflammation had resolved and the fractured tubercle could now be palpated. The area was tender and she found it painful to protrude her tongue. On review 6 weeks later, protrusion of her tongue was not painful but the floor of her mouth was still tender. A CT scan was requested to identify any pathology associated with the bone fragment, but no obvious abnormality was seen. In view of this, the patient was managed conservatively without any surgical intervention. After four months, she was asymptomatic and was referred to a specialist prosthodontist for new dentures and possible dental implant placement to improve the stability of her lower denture on her severely atrophic ridge.
Discussion
Genial turbercle fracture is very rare and there are only a small number of cases in the literature.1–13 All of these involved elderly edentulous patients aged between 63 and 86 with a 5–2 ratio of females to males. Prominence of the tubercles usually occurs as a result of severe alveolar atrophy, but different theories have been proposed to explain why the tubercles are enlarged. In some individuals, altered masticatory function develops to control the lower denture which causes enlargement caused by degenerative calcification of the ligaments.9,14 Another possible explanation, described by Stafne,15 is ossification of the normal embryonic cartilage similar to that observed with the styloid process.
Santos-Oller9 advised surgical intervention to remove the fractured tubercle and reattachment of the muscles in order to prevent chronic fibrous hyperplasia. However, most cases in the literature were managed in a similar way to the case presented and were observed with no active treatment. These patients all made a complete recovery with no loss of function.
The radiographic appearance of fractured genial tubercles has some similarities to that of a submandibular calculus, but these can usually be differentiated as they are positioned to one side of the midline and are often associated with a history of mealtime swelling. Although salivary calculi sometimes develop without significant symptoms, the history of genial tubercle fracture is usually a significant episode which the patient can easily recall and, on examination, the typical signs of bruising and swelling associated with a bony fracture should be evident.
Conclusion
Although it is rare, a fractured genial tubercle should be considered in the differential diagnosis of pain and swelling of the floor of the mouth in elderly edentulous patients.