Kasamatsu A, Kanazawa H, Watanabe T, Matsuzaki O Oral sarcoidosis: report of a case and review of literature. J Oral Maxillofac Surg. 2007; 65:1256-1259
Marie I, Proux A, Levesque H, Bony-Rerolle S, Chenal P Tongue involvement revealing sarcoidosis. QJM. 2008; 101:909-911
Antunes KB, Miranda AM, Carvalho SR, Azevedo AL, Tatakis DN, Pires FR Sarcoidosis presenting as gingival erosion in a patient under long-term clinical control. J Periodontol. 2008; 79:556-561
Koike K, Ide K, Shiratsuchi H, Nakashima T, Umezaki T, Komune S Sarcoidosis of the tongue: a case report. Auris Nasus Larynx. 2007; 34:131-133
Semenzato G ACCESS: A Case Control Etiologic Study of Sarcoidosis. Sarcoidosis Vasc Diffuse Lung Dis (official journal of WASOG/World Association of Sarcoidosis and Other Granulomatous Disorders). 2005; 22:83-86
Gribbin J, Hubbard RB, Le Jeune I, Smith CJ, West J, Tata LJ Incidence and mortality of idiopathic pulmonary fibrosis and sarcoidosis in the UK. Thorax. 2006; 61:980-985
McGrath DS, Daniil Z, Foley P Epidemiology of familial sarcoidosis in the UK. Thorax. 2000; 55:751-754
Mahevas M, Le Page L, Salle V Thrombocytopenia in sarcoidosis. Sarcoidosis Vasc Diffuse Lung Dis. 2006; 23:229-235
Consultant in Oral Medicine, Oral Medicine Department, Guy's Hospital, King's College London Dental Institute at Guy's and St Thomas' Hospital, London, UK
Sarcoidosis is a multisystem, non-caseating, chronic, granulomatous disease affecting any organ. In the head and neck region, salivary glands and lymph nodes are most commonly involved. Oral manifestations are rare but these lesions, occasionally haemorrhagic, may be the first sign of systemic disease. It is important to recognize the oral manifestations of sarcoidosis and to be aware of potential secondary disease-driven processes, such as thrombocytopenia. The purpose of this paper is to present a previously undiagnosed case of sarcoidosis, initially presenting with oral manifestations, including mucosal bleeding, and to review the current literature on oral sarcoidosis.
CPD/Clinical Relevance: Oral lesions can be the first sign of undiagnosed systemic sarcoidosis.
Article
Sarcoidosis is a classic non-caseating, multisystem, chronic, granulomatous disease affecting any organ. In the head and neck region, salivary glands and lymph nodes are most commonly involved. Oral manifestations are rare but have been reported in the literature.1,2,3,4,5,6 A new case of oral sarcoidosis with disease-driven thrombocytopenia is presented.
Case report
A 39-year-old female was referred to the Acute Dental Care Department by her dentist, with a 4-day history of spontaneous gingival bleeding. At the time of her consultation she also complained of lethargy, malaise, poor appetite resulting in 12.5 kg of unintentional weight loss and a persistent cough, which were undiagnosed and consequently not treated.
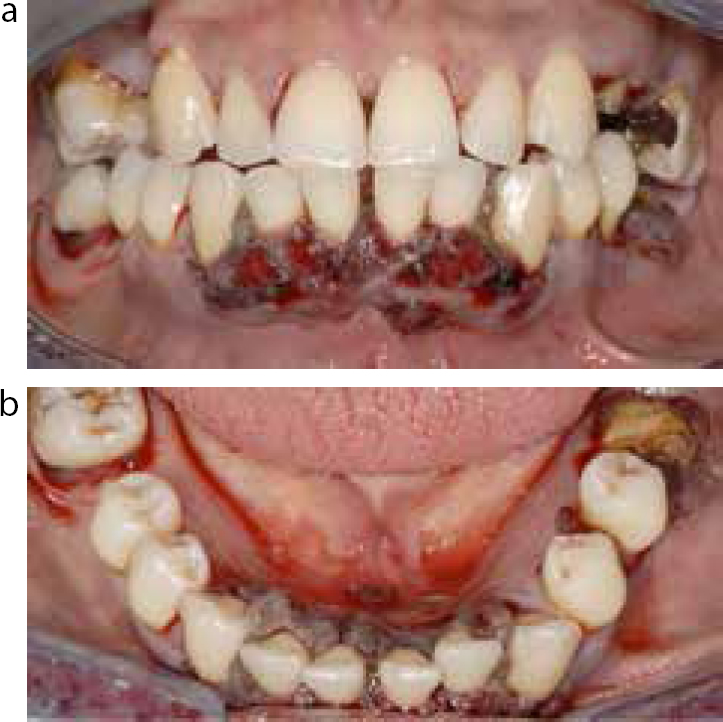
Examination revealed a swollen lower lip with petechial haemorrhages, spontaneous gingival bleeding and nodular areas with soft tissue hyperplasia in the lower labial gingivae (Figure 1). Several purpurae were present in the mouth, particularly on the left buccal mucosa, along with surrounding ecchymosis (Figure 2). No skin lesions were noted but the patient described pruritic petechial rashes on the legs which had resolved spontaneously.
Figure 1.
(a, b) Gingival hyperplasia and nodules, with bleeding on anterior labial gingivae.Figure 2. Purpurae and surrounding ecchymosis on buccal mucosa.
Initial differential diagnoses included platelet disorders, leukaemia and other bleeding disorders. Urgent blood investigations showed anaemia: 11.1 g/dl (normal range 12–15 g/dl) and marked thrombocytopenia: platelets 2x109/ml (normal range 150–400x109/ml). The patient was admitted urgently under the care of haematology. She was initially treated with systemic corticosteroids and tranexamic acid to reduce gingival bleeding, followed by platelet transfusion and intravenous immunoglobulins. The patient failed to improve and on further investigation a chest radiograph showed hilar lymphadenopathy and PET-CT scans showed splenomegaly and mediastinal, axillary, groin and upper abdominal adenopathy, suggesting lymphoma. At this stage, no biopsy was possible due to the continued low platelet levels. Eltrombopag (Revolade™, GlaxoSmithKline), a platelet regeneration therapy, was then administered and gave an incremental and sustained rise to normal platelet levels. Mediastinal lymph node biopsies were now possible, and showed multiple epithelioid granulomas, with dense fibrosis and numerous Langhans-type multinucleated giant cells. No acid-fast bacilli or fungal organisms were present and a tuberculin test was negative. The histopathological appearance was consistent with sarcoidosis having excluded other granulomatous lesions, such as tuberculosis, via negative Ziehl-Neelsen and periodic acid-Schiff stains.
A blood test showed raised SACE level of 106 IU/L (normal range 8–65 IU/L) also consistent with a diagnosis of sarcoidosis. The patient's lung function was normal and, following correction of her platelet level, no other treatment for her sarcoidosis was required. Before leaving hospital the patient was reviewed in the Oral Medicine Department and all oral lesions had resolved completely.
Discussion
Sarcoidosis is a multisystem, chronic, granulomatous disease with classic non-caseating granulomas in the affected organs, with the addition of T lymphocytes and mononuclear phagocytes.
Ninety percent of patients have pulmonary involvement, but other affected sites include mediastinal and peripheral lymph nodes, liver, spleen, eyes, bone, nasal mucosa, larynx, salivary gland, kidney, nervous system, heart, endocrine system, and gastrointestinal tract. Bone marrow involvement is rare, and isolated extrapulmonary sarcoidosis occurs in less than 5% of cases.7
Approximately 3000 new cases of sarcoidosis are diagnosed in the UK, with most being diagnosed over the age of 40. Males and females are equally affected.8 There is evidence of familial clustering which suggests that a shared determinant, either genetic or environmental, is operating in familial sarcoidosis cases.9
In the head and neck region, the most predominant sites are parotid glands where sarcoidosis can mimic, or occur in conjunction with, Sjögren's syndrome. Involvement of oral structures is uncommon, however, a review of the literature in 20073 found 23 well-documented cases of histologically-verified sarcoidosis manifesting in the oral mucosa without salivary gland or lymph node involvement. A further literature search found only five other reported cases since 2007,1,2,4,5,6 not including this case. The oral sites most commonly affected by sarcoidosis are: buccal mucosae (18%), gingivae (22%), tongue (25%), lips (18%), hard and soft palate (17%). The clinical presentation is of diffuse submucosal swelling or firm nodules with normal overlying mucosa.3 Oral swellings caused by sarcoidosis are not distinguishable clinically but should be considered in the differential diagnosis of soft tissue swellings and jaw lesions, because oral manifestations can be the first sign of systemic sarcoidosis when the patient is otherwise asymptomatic.3
There is no one specific confirmatory investigation so diagnosis is established by a combination of clinical features and investigations. These include histological evidence of non-caseating epithelioid granulomas, bilateral hilar lymphadenopathy on a chest radiograph,7 parenchymal lung disease, or both, an elevated SACE and an elevated 24-hour urine calcium level.
Severe thrombocytopenia is a rare presentation of sarcoidosis, and can be life-threatening. Different pathophysiological mechanisms are thought to be responsible for thrombocytopenia in sarcoidosis. Granulomas in bone marrow or hypersplenism may be involved but immune thrombocytopenic purpura must be suspected in all other cases. In all cases, there is rapid destruction of any platelets produced.10
Not all cases of sarcoidosis require treatment as the disease tends to be self-limiting. Oral sarcoidosis tends to resolve spontaneously.3 The mainstay of treatment of symptomatic sarcoidosis is corticosteroids, which leads to a good therapeutic response in most patients. A review of thrombocytopaenia secondary to sarcoidosis by Mahevas et al10 showed successful use of corticosteroids alone or in association with intravenous immunoglobulins, although some patients required a splenectomy. They also describe a case of successfully treated sarcoidosis with Rituximab, an anti-tumour necrosis factor (TNF) monoclonal antibody.
Conclusion
Patients with serious medical problems may present to the dental surgeon first with oral symptoms. Spontaneous gingival bleeding in particular should alert the dentist to the likelihood of a serious medical condition and prompt early referral to secondary care for investigation. Clinicians should also be aware that signs, such as salivary gland swelling, nodules in the palate, lips, buccal mucosae or gingivae, can indicate sarcoidosis and may be the first sign of disease. This patient was treated successfully for potentially fatal thrombocytopenia due to sarcoidosis because of the prompt action of her dentist.