Kalantzis A, Scully C. Oxford Specialist Handbook of Applied Medicine and Surgery in Dentistry.Oxford: Oxford University Press; 2009
Galán Gil S, Peñarrocha Diago M, Peñarrocha Diago M. Malignant mental nerve neuropathy: systematic review. Med Oral Patol Oral Cir Bucal. 2008; 13:616-621
Brady B, Coughlan AM, O'Brien T. Numb chin syndrome: a case report. J Pain Symptom Manage. 2016; 51:e3-4
Odell EW. Cawson's Essentials of Oral Pathology and Oral Medicine.: Elsevier Health Sciences; 2017
Loncarevic S, Brajkovic D, Vukomanovic-Djurdjevic B Bilateral numb chin syndrome as a symptom of breast cancer metastasis in the mandible: a case report and discussion on the usefulness of cone-beam computed tomography to assess bone involvement in oral cancer. Oral Radiol. 2016; 32:136-142
Hassanali H, Mannion C, Kanatas A. The full extent. Br Dent J. 2011; 210
Gandhi L, Rodríguez-Abreu D, Gadgeel S Pembrolizumab plus chemotherapy in metastatic non-small-cell lung cancer. N Engl J Med. 2018; 378:2078-2092
Brambilla E, Travis WD, Colby TV The new World Health Organization classification of lung tumours. Eur Respir J. 2001; 18:1059-1068
Ost DE, Yeung SC, Tanoue LT, Gould MK. Clinical and organizational factors in the initial evaluation of patients with lung cancer: diagnosis and management of lung cancer: American College of Chest Physicians evidence-based clinical practice guidelines. Chest. 2013; 143:e121S-141S
The Numb Lip: Non-Small Cell Lung Cancer First Presenting in the Head and Neck Michael Daldry Timothy Edwin Lloyd Grant Stewart Dental Update 2025 49:1, 48-50.
Diagnosing the cause of paraesthesia can be challenging. A patient with an unremarkable medical history, non-smoker and no known allergies, presented with paraesthesia in the distribution of the mental nerve with no obvious dento-alveolar pathology. After further investigations the patient was found to have multiple brain metastases and a solitary mandibular deposit, with the primary site being an adenocarcinoma of the lung.
CPD/Clinical Relevance: As dental professionals, knowledge of head and neck manifestations of systemic conditions is required if prompt diagnosis and treatment is to occur, which will subsequently improve patient health outcomes.
Article
Paraesthesia or anaesthesia of the lower lip is commonly associated with damage or compression of the inferior alveolar nerve and there are multiple causes. These include peripheral causes, such as past dental treatment involving inferior dental nerve blocks, post-surgical damage, trauma, infection (osteomyelitis), extensive ridge resorption with associated compression from a denture, and neoplastic or non-neoplastic jaw lesions in anatomical proximity to neural structures.
Paraesthesia in the lower lip can also be a sign of intracranial disease, such as multiple sclerosis, tumour, trigeminal neuralgia or cerebrovascular disease (stroke). There are also psychogenic (eg hyperventilation syndrome and hysteria), drug-induced (acetazolamide, labetalol, sulthiame), and systemic (electrolyte abnormalities such as hypocalcaemia causing tetany) causes, along with haematinic deficiency, and some connective tissue diseases.1
Red flags (but not exhaustive) indicating urgent referral to secondary care include: spontaneous focal neuropathy with no known associative cause; presence of a palpable mass in patients aged under 50 years; and associated neurological symptoms, such as seizures, headaches, limb weakness and a confirmed past medical history of cancer.2 Cancers most likely to metastasize to the jaw are breast, prostate, lung and leukaemia.3
Metastatic disease of the jaw is rare, but when it does occur, it is commonly associated with the blood-borne distribution of adenocarcinoma.4 The mandible, along with the spine, pelvis and femur, has a high medullary bone content, providing the ideal environment for cancer cells to survive. When tumours are found in the jaw, it is usually an indication of late stage cancer,5 indicating that the primary site and other metastases should be sought. Primary presentations in the jaw are rare, but should not be forgotten in the dentist's list of differential diagnosis.6
Case report
The patient presented with numbness and altered sensation to the left hand side of chin and lip. The patient had an unremarkable medical history, with no known allergies and was a non-smoker. After a 10-day monitoring period, there was no resolution of the numb area and the patient's GP sent an urgent referral to the oral and maxillofacial surgery department for further investigations. The patient had no other peripheral or central neurological symptoms at this point.
Investigations
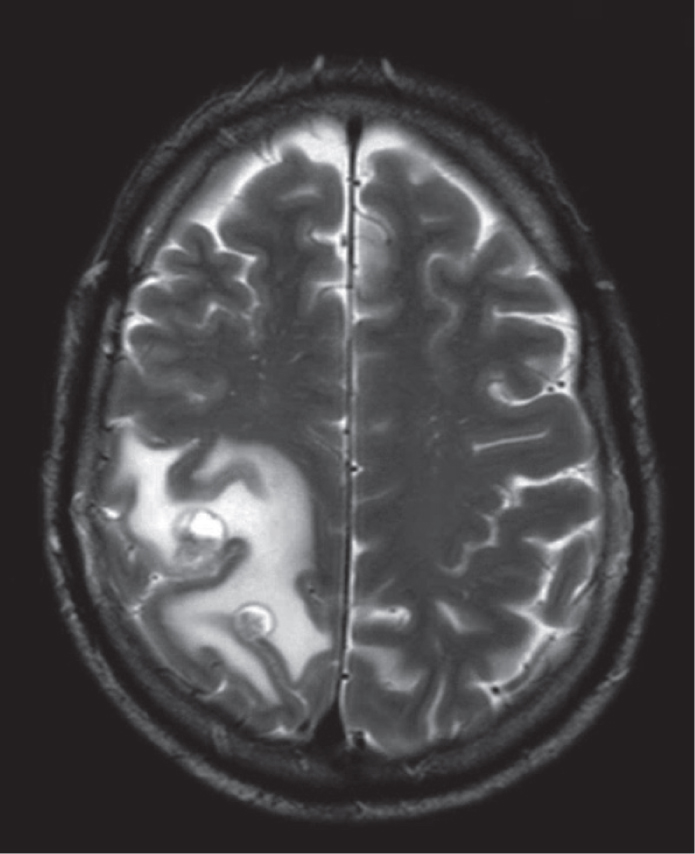
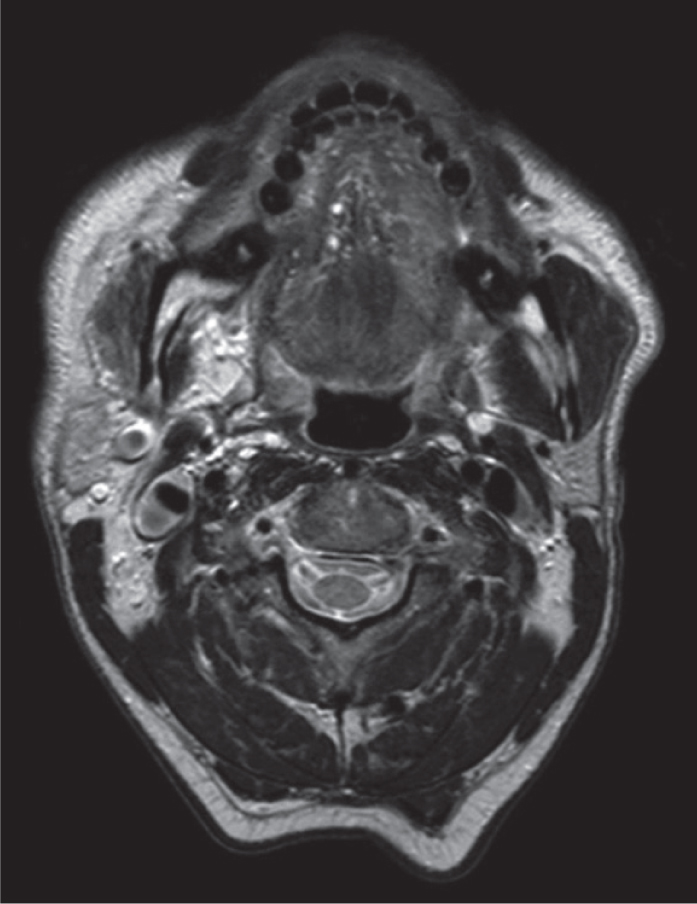
On examination, the patient had obvious anaesthesia in the distribution of the left mental nerve, and, with further mechanical testing, allodynia was also reported. An OPT (Figure 1) was requested and revealed no obvious dento-alveolar cause on the left-hand side; however, on the right side, the OPT showed a well-defined radiolucency in the right ramus. Further investigation with a craniofacial MRI identified multiple intra-cranial metastases (Figure 2), in addition to a small deposit within the left mandibular ramus (Figure 3), accounting for the mental nerve neuropathy. The right-hand side radiolucency on the OPT was concluded to be artefactual, because further 3D imaging showed only a slightly enlarged mandibular foramen, with no other abnormalities.
Figure 1. Orthopantomogram investigating dento-alveolar causes of anaesthesia in the left mandibular ramus. No obvious lesion identified on ipsilateral side. RHS contralateral to the patient's symptoms shows a well defined radiolucent area in the ramus; this was concluded to be artefactual after further 3D imaging.Figure 2. Two small enhancing mass lesions in the right dorsal frontal/parietal region with surrounding oedema seen on MRI.Figure 3. Abnormal signal in the left mandibular ramus with associated oedema shown on MRI.
Differential diagnosis:
Widespread intra-cranial metastases are usually indicative of either adenocarcinoma or malignant melanoma. The patient subsequently underwent a full skin check and a CT head thorax, abdomen and pelvis was organized, to stage the disease.
Diagnosis
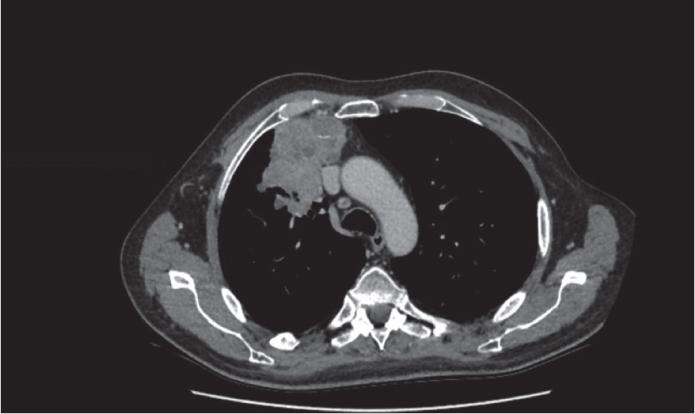
The patient was discussed at the lung multidisciplinary team meeting, which included respiratory physicians, oncologists, radiologists and clinical nurse specialists. The staging CT revealed a large anterior mass in the upper lobe of the right lung, which measured 7.7 × 7.1 × 4.7 cm with local invasion of the right mediastinum (Figure 4). Multiple ipsilateral and contralateral lung metastases were also present along with bilateral adrenal metastases. This was reported to be consistent with lung adenocarcinoma. A subsequent CT-guided biopsy confirmed adenocarcinoma, for which the most effective treatment included combined chemotherapy and immunotherapy.7 The patient commenced treatment, which was well tolerated and he experienced minimal side effects.
Figure 4. Large mass anteriorly in the right upper lobe on CT
Disease progression/complications
As the patient's disease progressed, he presented with focal seizures following the development of cerebral oedema. Dexamethasone was prescribed to manage these symptoms and the patient responded well. With seizure presentation, it was necessary to inform the DVLA as the patient had now become unfit to drive.
Despite treatment, re-imaging after three cycles showed frank disease progression at all sites. The patient became more debilitated by his neurological disease, and there was little response to increased doses of steroids. He died at home, 6 months after initial presentation.
Discussion
Adenocarcinoma presenting with only paraesthesia and altered lip sensation is extremely rare, with few documented cases. Therefore, it is important to have an awareness of the uncommon presentation of a common cancer of the lungs.
Non-small cell lung cancers make up 80% of lung cancers, of which 45% are adenocarcinomas.8 They are more common in the elderly population and associated with smoking.9 Lung cancers can remain asymptomatic for a long period of time. The lungs have a large functional reserve and few pain fibres and tumours can remain small while invading local structures and metastasizing to both bone and brain.10 Therefore, when presentation occurs, the cancer can be in its late stages.
Presentation of this cancer in the jaw as the first and only symptom in a non-smoker is uncommon. With no obvious dental cause, even after an OPT, there was a high suspicion of systemic factors, warranting further diagnostic imagining, which was effective in achieving an accurate and timely diagnosis.
Most of the marrow in the mandible lies below the inferior dental nerve canal and is, therefore, most likely to be seeded by metastases. Using the ID canal as an anatomical landmark can help distinguish radiographic findings from non-dental and dental origins. Radiographically, metastatic lesions can mimic infection and there should be high degree of suspicion should be raised if this does not correlate clinically, or with the patient's history.4 Prompt referral in accordance with the cancer pathway guidance,11 biopsy and subsequent histopathology is essential for diagnostic confirmation and targeted treatment.
The patient in this case started combined chemo/immunotherapy. This treatment has been shown to significantly increase patient prognosis and survival. However, in cases where cancer presentation is late, 1-year survival is 69.2% and median cancer-free survival is 8.8 months.7
Conclusion:
Early diagnosis is crucial to improve patient health outcomes and quality of life. As dental professionals, knowledge of head and neck anatomy, the possibility of systemic disease manifestations, including metastatic disease, in these area should be considered part of a differential diagnosis. If there is suspicion, urgent referral on the two-week wait pathway to the relevant specialty, should be undertaken.