Andreasen JO, Paulsen HU, Yu Z A long-term study of 370 autotransplanted premolars. Part II. Tooth survival and pulp healing subsequent to transplantation. Eur J Orthod. 1990; 12:14-24 https://doi.org/10.1093/ejo/12.1.14
Kim E, Jung JY, Cha IH Evaluation of the prognosis and causes of failure in 182 cases of autogenous tooth transplantation. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 2005; 100:112-119 https://doi.org/10.1016/j.tripleo.2004.09.007
Park S, Lee H, Lee E Guided autotransplantation of impacted canines using a cad/cam surgical template. Children (Basel). 2023; 10 https://doi.org/10.3390/children10040708
Czochrowska EM, Stenvik A, Album B, Zachrisson BU Autotransplantation of premolars to replace maxillary incisors: a comparison with natural incisors. Am J Orthod Dentofacial Orthop. 2000; 118:592-600 https://doi.org/10.1067/mod.2000.110521
Plakwicz P, Wojtowicz A, Czochrowska EM Survival and success rates of autotransplanted premolars: a prospective study of the protocol for developing teeth. Am J Orthod Dentofacial Orthop. 2013; 144:229-237 https://doi.org/10.1016/j.ajodo.2013.03.019
Clokie CM, Yau DM, Chano L Autogenous tooth transplantation: an alternative to dental implant placement?. J Can Dent Assoc. 2001; 67:92-96
Andersson L, Bodin I, Sörensen S Progression of root resorption following replantation of human teeth after extended extraoral storage. Endod Dent Traumatol. 1989; 5:38-47 https://doi.org/10.1111/j.1600-9657.1989.tb00335.x
In this article, we present a case report on the autotransplantation of an upper left canine (UL3) into the site of a retained upper left deciduous canine (ULC) in a 36-year-old male using a digital guided approach. The procedure involved meticulous pre-operative planning, careful extraction of the ULC and UL3, and the use of a stereolithic tooth and a surgical guide created using cone beam computed tomography (CBCT) data. Follow-up included endodontic treatment post-transplantation. The successful outcome of this case underscores the importance of how imaging techniques can help to provide successful and predictable autotransplantation results. This case report highlights the successful integration of a transplanted tooth and the unique approach to the techniques used.
CPD/Clinical Relevance: Autotransplantation of an impacted tooth can be considerd as a treatment option for the adult patient with a single tooth edentulous space or retained deciduous tooth.
Article
Autotransplantation involves the relocation of a tooth from one part of the mouth to another. This has evolved significantly over the years to become a crucial technique in oral rehabilitation. While the concept is not new to dentistry, it has seen its application and success rate increase dramatically, particularly due to advancements in surgical techniques and imaging technologies. The foundational work by Andreasen et al has been instrumental in demonstrating the viability and success of these procedures.1
Autotransplantation presents itself as a viable alternative to more conventional methods such as bridges, dentures, implants, or orthodontic treatments. The evaluation of the prognosis and causes of failure in autogenous tooth transplantation by Kim et al has provided a deeper understanding of critical factors that contribute to the success of such procedures. Two of these pertinent areas of consideration are the initial stability of the transplanted tooth, and the extra-oral time experienced by donor teeth. Transplanted teeth require a recipient site that has been as precisely prepared as possible, and while the computer-aided rapid protoype (CARP) tooth model allows operators the means to do so, success ultimately rests on the skill of the surgical operator and their preparation of the recipient site. This evaluation by Kim et al revealed improved results in early healing, but no significant difference in the later healing stages. With regards to extra-oral time, it has been noted that the less time this is, the better. This is due to increased potential for root surface injury, which can lead to root resorption or ankylosis.2
Historically, the autotransplantation of canine teeth was less common, primarily because of challenges in matching donor and recipient sites. However, with the advent of precise imaging techniques, such as cone beam computed tomography (CBCT), and the use of computer-aided design/computer-aided manufacturing (CAD/CAM) in dental applications, the feasibility and predictability of such procedures have improved considerably. The advancements in diagnostic and surgical techniques, as discussed by Park et al have been game-changing in the field of dental surgery.3 These technological leaps have dramatically improved the predictability and success rates of complex dental procedures, such as autotransplantation.
The patient upon whom we are focusing presented with a unique challenge: a retained ULC and a palatally displaced UL3. The decision to auto transplant the UL3 into the ULC site was influenced by several factors, including the patient's age, oral health status, and the specific anatomical considerations of the teeth involved.
The literature on canine tooth autotransplantation provides a spectrum of outcomes and methodologies. Earlier studies focused on tooth survival and pulp healing after transplantation, highlighting the importance of factors including root development stage, surgical technique, and post-operative care. More recent research by Lee et al has delved into the role of advanced imaging and surgical guides in enhancing success rates on the clinical application of CARP for tooth transplantation.4
This case report highlights the use of a laboratory-made canine model tooth with a fully guided osteotomy from a tooth-supported guide, using the CBCT digital imaging and communications in medicine (Dicom) data and standard tessellation language (STL) file of a digital pre-operative scan. This approach can aid in the precise surgical planning and fitting of the tooth before its removal. It also helps anticipate and manage potential difficulties of the procedure, such as the curved apex of an autotransplanted tooth. Such technological integration represents a significant leap from the rudimentary methods of autotransplantation where success was largely dependent on the surgeon's experience and visual judgement.
Patient selection
Patient selection is critical in autotransplantation. Ideal candidates are typically those in good general and oral health, with sufficient bone structure to support the transplanted tooth. Age plays a significant role; younger patients with developing dentition often have a better prognosis owing to the potential for continued root development and bone adaptation. However, as demonstrated the presented case (Figures 1 and 2), successful autotransplantation is not limited exclusively to younger individuals, a perspective also supported by the work of Paulsen, who discusses autotransplantation in orthodontic treatment.5
Figure 1. Pre-operative situation.Figure 2. Axial view of the pre-operative situation.
There are multiple advantages to autotransplanting a canine tooth. It allows for the preservation and relocation of a natural tooth, maintaining proprioception as well as aesthetics, both of which are often compromised with artificial prostheses. Moreover, it helps in preserving the alveolar bone structure and the integrity of the surrounding soft tissues, which is essential for long-term oral health. In this patient's case, these benefits were crucial considerations, given the functional and aesthetic importance of the canine tooth. This is echoed in the study by Czochrowska et al that compared autotransplanted premolars with natural incisors.6
One major contraindication is inadequate bone support in the recipient site. The success of autotransplantation largely depends on the recipient site's ability to support the transplanted tooth. If there is insufficient bone volume or quality, the procedure is likely to fail.1 Additionally, the periodontal health of the patient plays a crucial role. Patients with active periodontal disease or poor periodontal health are not considered good candidates for this procedure, because these conditions can significantly compromise the transplant's success.7
The condition of the donor tooth is another critical factor. The donor tooth must be vital and structurally sound. Non-vital or significantly damaged teeth are unsuitable for transplantation, because they do not provide a viable option for successful autotransplantation.8
Furthermore, autotransplantation offers a cost-effective and biologically harmonious solution. When compared to other dental restoration option. such as implants or bridges, it presents a less invasive and more conservative approach. This aspect was particularly relevant in our patient's treatment plan, considering the long-term health and stability of the oral cavity, a notion supported by Tsukiboshi, explaining the requirements for predictable success in autotransplantation of teeth.7
Case report
Pre-operative assessment and planning
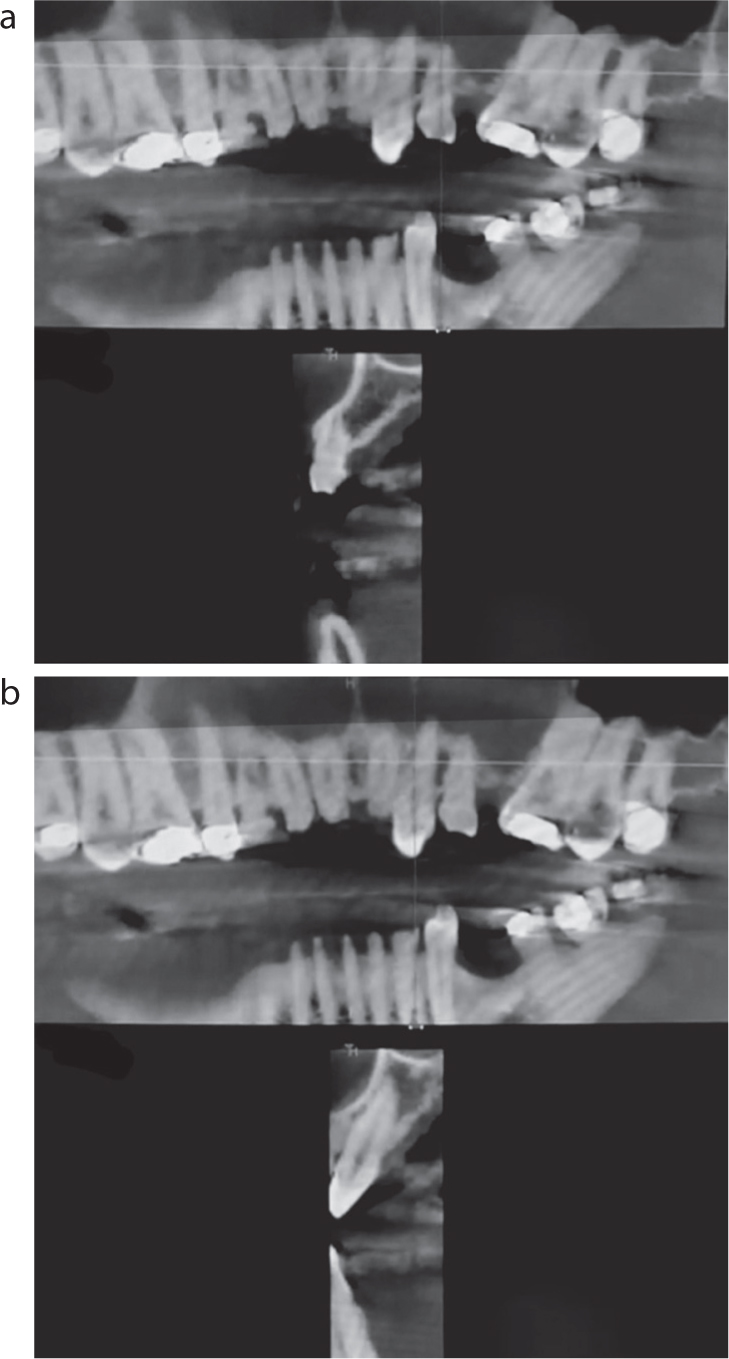
The foundation of successful autotransplantation is dependent on thorough pre-operative planning. In this case, a detailed assessment was conducted using pre-operative cone beam computed tomography (CBCT) (Figure 3). This advanced imaging technique, as discussed by Park et al, provided a three-dimensional view of the patient's dental anatomy, facilitating accurate planning.3 The ULC was digitally extracted from the pre-operative intra-oral scan and the UL3 virtually placed. Once placed, this STL file was used alongside the CBCT data to produce a tooth-supported osteotomy guide. This was crucial in ensuring precision in both the extraction and transplantation steps, a technique that has been highlighted in the work of Lee et al for its role in enhancing the success rates of complex dental procedures.4 In this way, we were able to ensure the osteotomy provided the ideal tooth position of the autotransplanted tooth.
Figure 3. Pre-operative CBCT slices of (a) ULC and (b) UL3.
Surgical technique
Extraction of ULC
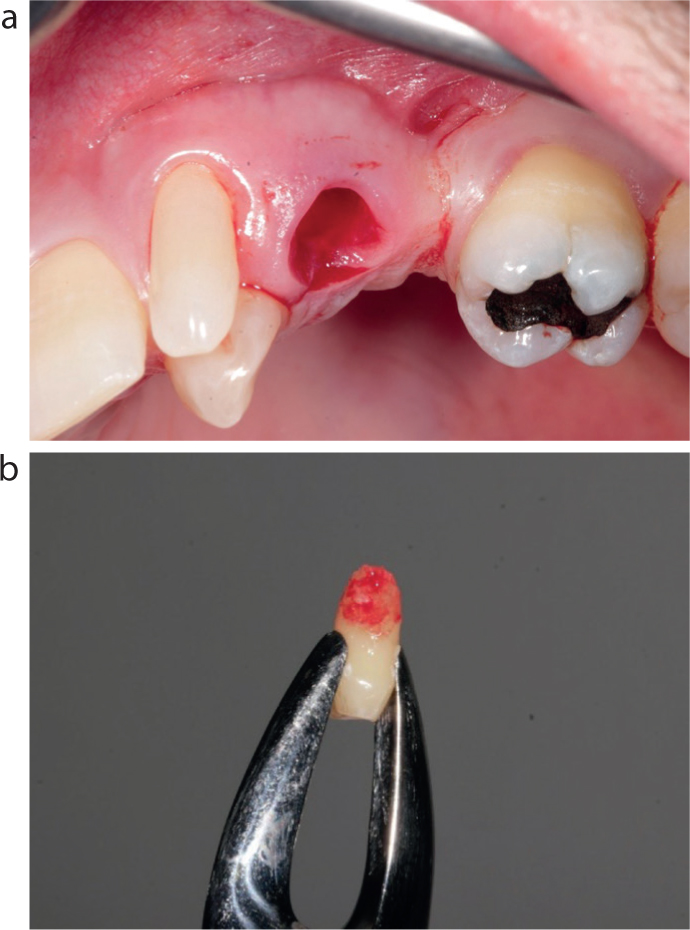
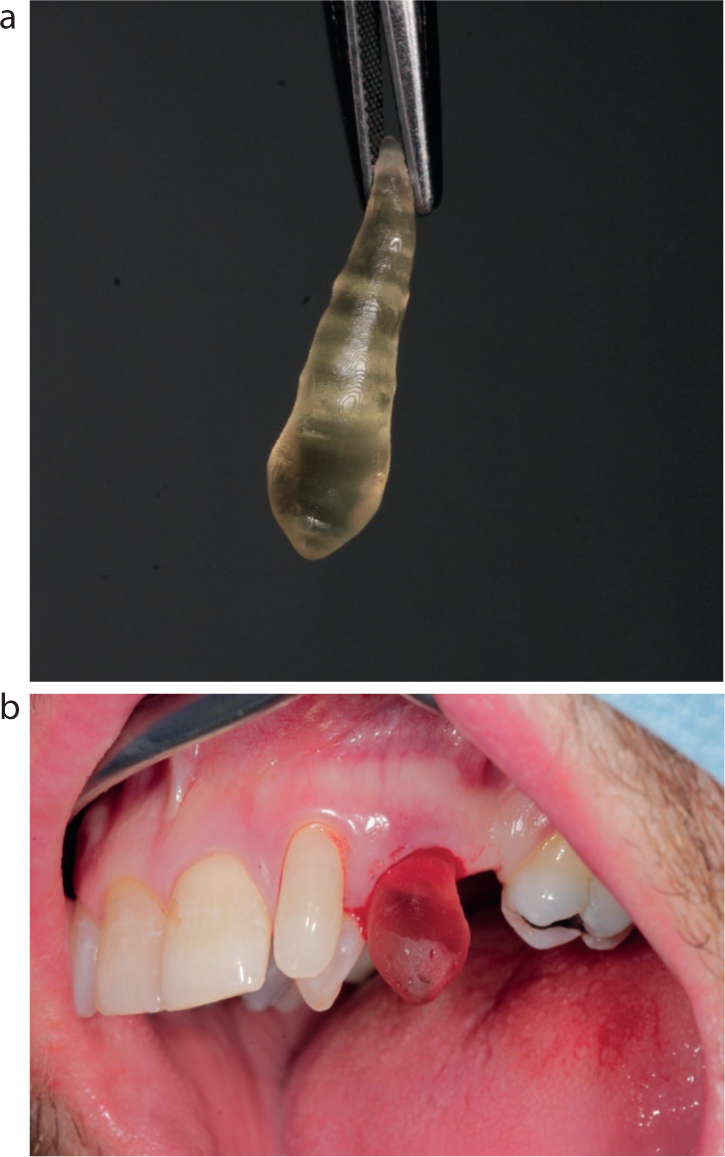
The first step involved the extraction of the ULC (Figure 4). Care was taken to preserve the integrity of the surrounding bone and soft tissues, a vital factor for the success of the transplanted tooth, as highlighted by Tsukiboshi.7
Figure 4. (a) ULC extraction socket and (b) the extracted tooth.
Preparation of the ULC site
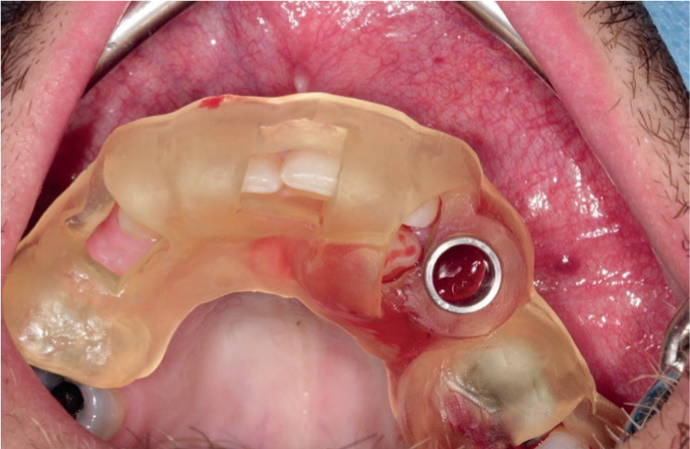
Following the extraction, the ULC socket was thoroughly degranulated with round surgical burs and irrigated with saline. The osteotomy was completed with implant drills and the tooth-supported osteotomy guide (Figure 5).
Figure 5. Tooth-supported osteotomy guide in place.
Trial fitting
A stereolithic lab-made model copy of the canine created from the CBCT data was used to ensure the transplanted tooth would fit perfectly in the socket (Figure 6).
Figure 6. (a) Stereolithic tooth. (b) Stereolithic tooth in the newly made socket.
Extraction of UL3
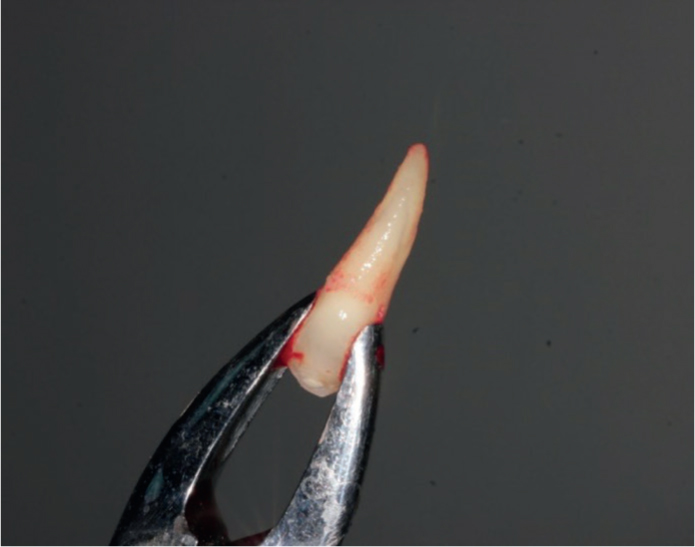
The UL3 was extracted as carefully as possible, avoiding any contact with the periodontal ligament. Only forceps were used to contact the tooth crown above the cemento-enamel junction before extraction, avoiding the use of any luxators or periotomes. Immediate local irrigation of the extraction socket with metronidazole (500 mg/100ml intravenous infusion) was performed to reduce post-operative infections (Figure 7).
Figure 7. The extracted UL3.
Transplantation of UL3
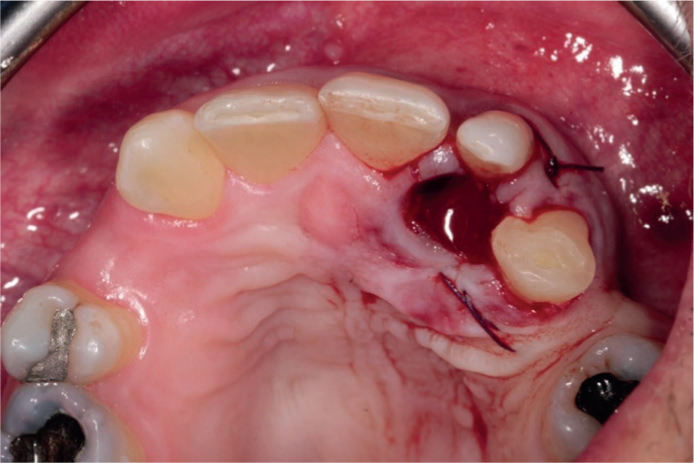
The UL3 was then carefully positioned into the prepared ULC site (Figure 8). The fit was verified to be snug, an essential factor for the stability and integration of the transplanted tooth, as noted by Clokie et al in their examination of autogenous tooth transplantation as an alternative to dental implants.9
Figure 8. UL3 tooth fitted into socket.
Stabilization
A sling suture, using 4-0 Vicryl Rapide, was placed to stabilize the transplanted tooth, ensuring minimal movement during the initial healing phase (Figure 9), a technique underlined by Andreasen et al for its importance in the success of tooth transplantations.1
Figure 9. Sling suture used to help stabilize autotransplanted tooth.
Post-operative care and management
An immediate post-operative intra-oral scan allowed the fabrication of an Essix retainer, which was fitted the following day. This enabled passive splinting of the newly autotransplanted tooth.
The patient was provided with detailed post-operative instructions. These included managing potential bruising and swelling, dietary recommendations, and prescriptions for antibiotics and analgesics. The patient was also advised on sleeping positions to minimize discomfort and bleeding. Such meticulous post-operative care is crucial for ensuring the success of the transplantation and the patient's comfort.
Endodontic treatment
The patient underwent endodontic treatment of the UL3 2 weeks after the autotransplantation (Figure 10), as per recommendations by Andersson et al.10
Figure 10. (a) Peri-apical radiograph showing master cone gutta percha in situ during root canal therapy. (b) Peri-apical radiograph showing completed root canal therapy. (c) Peri-apical radiograph at 12 months post operatively.
A 12-month peri-apical radiograph was taken to check for bone levels and apical health (Figure 10c).
Discussion
This article not only describes a digitally planned surgery with help from both a CBCT Dicom file and an STL file to design an osteotomy guide and replica resin tooth, but also an immediate post-operative digitally fabricated Essix retainer enabling passive splinting of the new autotransplanted tooth.
Autotransplantation of teeth, especially canines, presents a unique alternative to dental implants or orthodontic interventions. In this patient's case, the decision to autotransplant the UL3 instead of opting for an implant or orthodontic re-alignment was based on several factors, including the desire to preserve natural dentition and the patient's specific anatomical considerations. While dental implants are a popular choice for tooth replacement, they cannot provide the same proprioceptive feedback as natural teeth or establish the same biological periodontium, a consideration highlighted in the research by Clokie et al.9 Similarly, orthodontic treatments to re-align existing teeth can be time-consuming and may not always be feasible, particularly in adult patients with less malleable bone structures.
The surgical challenges in this case were manifold, ranging from ensuring the viability of the periodontal ligament cells during extraction and transplantation, to achieving a perfect fit in the recipient site. These steps highlight the importance of evolving surgical techniques and materials in improving the outcomes of such procedures, as noted in the extensive research by Andreasen et al.1
Post-operative care is vital in the success of autotransplantation. In this case, detailed instructions on managing swelling, bruising, dietary restrictions, and oral hygiene were pivotal in the patient's recovery, as was the use of analgesics.
Looking forward, the future of dental autotransplantation appears to be promising, particularly with the ongoing advancements in imaging and surgical techniques. Ongoing research is needed to further refine these methods, reduce the incidence of complications, and improve long-term success rates. Studies focusing on patient outcomes, especially in adult populations, can provide deeper insights into the efficacy and viability of autotransplantation as a standard dental procedure. Additionally, exploring the genetic and biological factors that influence the healing and integration of transplanted teeth could open new avenues for personalized dental care.
Conclusion
This case study of canine tooth autotransplantation sheds light on the current capabilities and challenges in the field. It underscores the importance of a multidisciplinary approach, incorporating advanced technology, meticulous surgical technique, and comprehensive post-operative care, to achieve successful outcomes. As dental technology and techniques continue to evolve, autotransplantation stands as a viable and effective option for tooth replacement, meriting further exploration and refinement.
In summary, this case study contributes to the literature on dental autotransplantation, offering practical insights and underlining the importance of continual research and innovation in this specialized field. The collaboration between advanced technology, surgical expertise, and comprehensive patient care forms the cornerstone of successful autotransplantation procedures, setting a standard for future cases and research in dental medicine.