Manakou A, Kavvadia K, Silvestros S, Angelopoulou E. Subgingival foreign body embedment in a preschool child: management with three and a half years follow-up. Eur J Paediatr Dent. 2004; 5:46-49
Becker T, Neronov A. Orthodontic elastic separator-induced periodontal abscess: a case report. Case Rep Dent. 2012; 2012
Ellison R, Rahman S, Barker D, Larmour C. Onychophagia and subgingival foreign body embedment: a case report. Br Dent J. 2014; 216
Ondik MP, Daw JL. Unusual foreign body of the hard palate in an infant. J Pediatr. 2004; 144
Sandler RH, Kumar A, Richardson KA, Constant E. Foreign body in the hard palate. Pediatrics. 1987; 79:484-485
Srivastava N, Vineeta N. Foreign body in the periradicular area. J Endod. 2001; 27:593-594
Colaneri L, Granger TR. Gold chain found between maxillary incisors. Oral Surg Oral Med Oral Pathol. 1982; 54
Serrant P, Mani WR, Clarke S. Gun pellet radiopacity. Br Dent J. 2012; 213
McAuliffe N, Drage NA, Hunter B. Staple diet: a foreign body in a tooth. Int J Paediat Dent. 2005; 15:468-471
Tseng E, Woolley AL. Foreign body simulating a hard palate lesion in a child. Int J Pediatr Otorhinolaryngol. 1996; 38:169-174
Tavargeri AK, Rao CB, Thakur S. Foreign body in the mouth and the dilemma in diagnosis: a case report. J Calif Dent Assoc. 2010; 38:512-513
Soubhia AM, Ribeiro AC, Martins LD Unusual wooden foreign body in the palate. Br Dent J. 2007; 203:573-574
Passi S, Sharma N. Unusual foreign bodies in the orofacial region. Case Rep Dent. 2012; 2012
This paper describes a case of an intra-osseous foreign body impaction in the hard palate, a chicken bone fragment, in an adult male. The presentation mimicked that of an odontogenic lesion. Though palatal soft tissue foreign bodies in toddlers are well reported, the literature is sparse on cases involving adults. The location of the foreign body, and radiographic presentation, resulted in a diagnostic challenge to the attending clinician. This appears to be the first reported case of an animal bone presenting in this way in an adult.
CPD/Clinical Relevance: The case highlights the importance of credible history reporting, 3D imaging and developing accurate differentials in the diagnostic pathway when faced with an atypical clinical presentation.
Article
Case history
A 47-year-old male presented to his general dentist with a painful palatal swelling of 2 day's duration between the UR2 and UR1. He reported a history of a chicken bone lodged behind his front tooth 12 months previously that he had been unable to remove. He remembered a small swelling immediately following the incident, which resolved shortly after. No further care was sought, but at the time of presentation, the patient was convinced it was the source of his pain. His medical history was unremarkable, and no other history of trauma was reported.
The tender ovoid, firm palatal swelling measuring 1 x 1 cm in size, with no suppuration, extended from the mesial surface of UR1 to the distal surface of UR2. The surface did not blanch and was the colour of normal mucosa. The buccal attached gingiva in the region of UR2 and UR1 was erythematous and mildly tender. The UR2 was tender to percussion and palpation and demonstrated grade 1 mobility. Hygienic Endo-Ice Pulp Vitality Refrigerant testing with a cotton pledget indicated a vital pulp in UL1, UR1, UR2. All other anterior teeth showed no abnormal findings.
Radiographic assessment confirmed an ill-defined radiolucency in the middle third radicular region, between the roots of UR1 and UR2 (Figure 1). An impacted supernumerary was also noted, but this was not associated with the radiolucency.
Figure 1. Peri-apical radiograph demonstrating a supernumary tooth and radiolucency in the mid third radicular region between the UR1 and UR2.
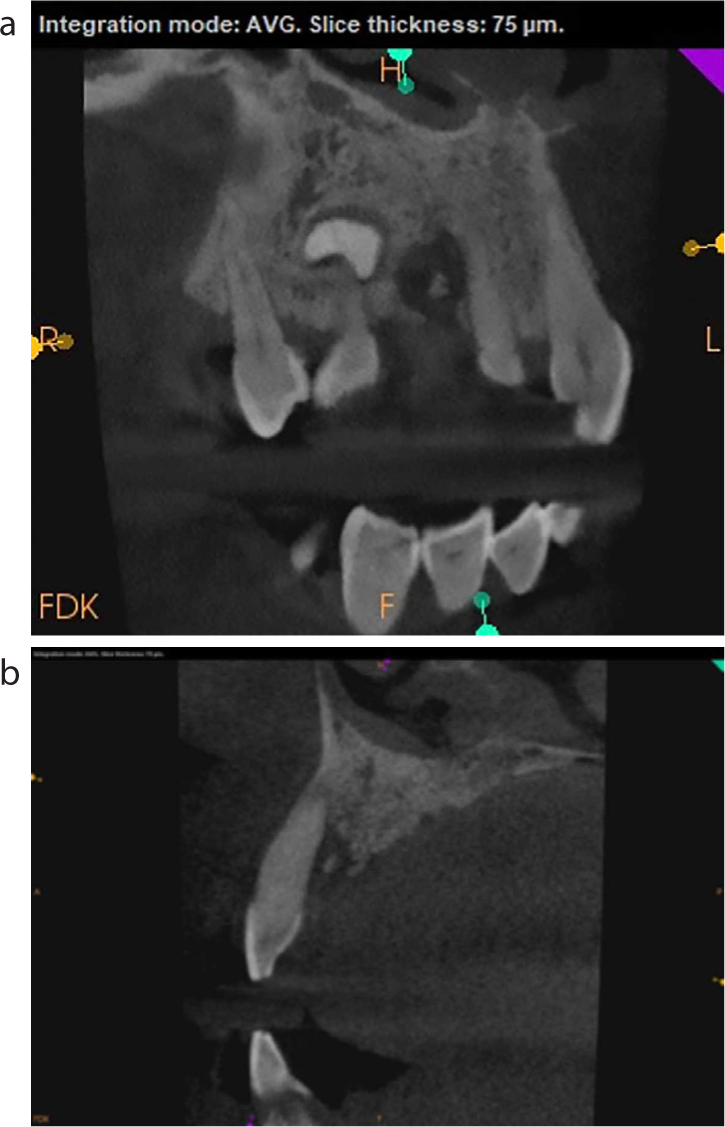
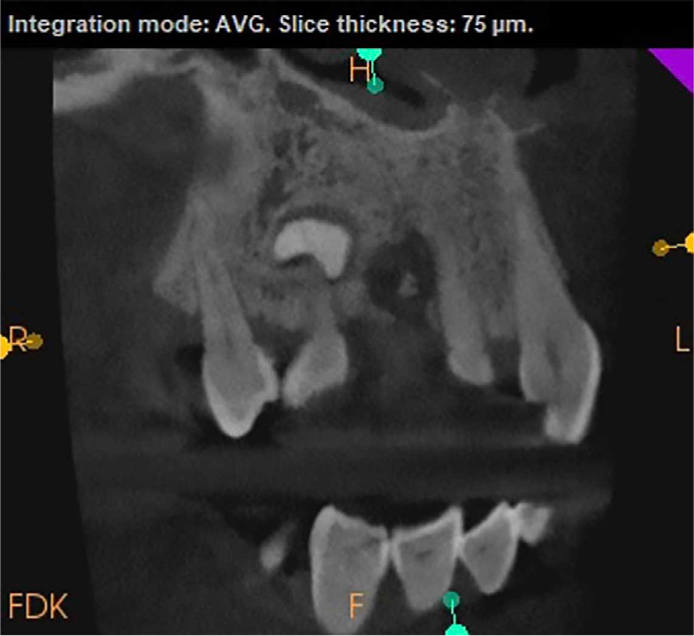
A subsequent CBCT revealed a radio-opaque mass palatal to the incisors with a surrounding radiolucency that was ill defined and not well corticated. In the sagittal section the radiolucent region around the opacity extended apically involving almost 90% of the root surface. The ectopic tooth was not involved (Figure 2). On the axial section, the radiolucency extended across the palatal aspect of the UR2, and the mesiodistal root surface of the UR1 (Figure 3). Both labial and palatal cortical plates remained intact.
Figure 2. (a, b) Sagittal slices of the CBCT showing the extensive radiolucent lesion involving almost 90% of the root surface.Figure 3. Axial slice of the CBCT where the lesion clearly involves both the UR1 and UR2, with sparing of the labial and palatal cortical plates.
In view of the concerning CT findings of a mixed lesion with ill-defined borders, the patient was referred to an oral surgeon for further evaluation. The differential diagnosis included bony sequestrum secondary to chronic osteomyelitis, foreign body impaction deduced from history or a calcifying odontogenic tumour. An adenomatoid odontogenic tumour was not considered owing to the location and uninvolvement of the unerupted tooth. A cementoma was also excluded owing to the location and non-involvement of the root apex.
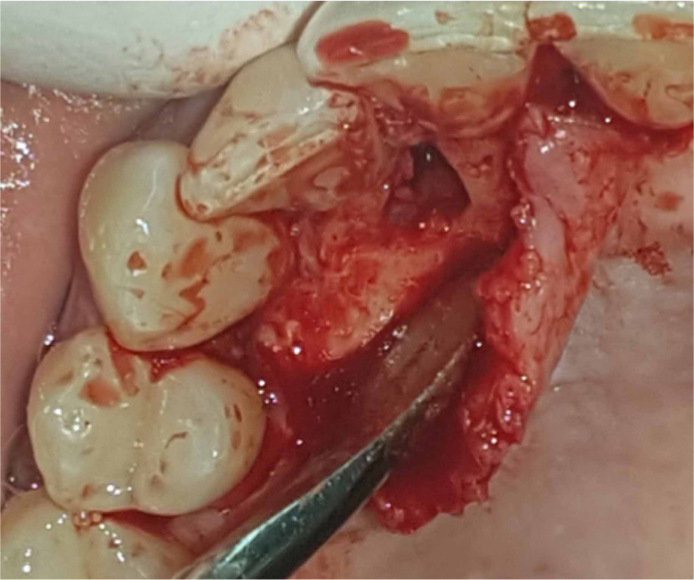
A palatal envelope flap was raised to expose the lesion (Figure 4). A small amount of granulation tissue was curetted, which exposed a loose splinter-like bony mass (Figure 5). This fitted the patient's description of the fragment of chicken bone that was lodged 1 year previously. The bony defect was explored and cleaned, the wound was closed and the patient placed on post-operative antibiotics and analgesics. He healed uneventfully. Bone regeneration was to be assessed and a secondary decision made on periodontal regeneration with graft and membrane if a large bony defect persisted in 6 months following the procedure.
Figure 4. Intra-oral photograph demonstrating the reflected palatal flap and bony defect after removal of the foreign body.Figure 5. Photograph showing the removed fragment of the reported chicken bone (8 mm).
Discussion
Foreign bodies in the maxillofacial region can be attributed to a plethora of incidents, including trauma, physical aggression and those that are iatrogenic in nature.
The majority of the literature relating to palatal foreign bodies is associated with infants, and involves soft tissue impactions in the hard palate itself. The literature revealed some examples of foreign bodies in the oral cavity that include:
Unfortunately, many cases can be misdiagnosed as suspected odontogenic tumours or neoplasms leading to unnecessary intervention and emotional distress.10,11 The literature also reveals one report of an intra-osseous calcified mass confirmed to be a wooden foreign body.12
As an accidental impaction of a foreign body, which not only remained asymptomatic for some time, but silently inflicted severe rapid medullary bone destruction in an otherwise healthy surrounding periodontium, this case may be unique. The chicken bone had been lodged for over 12 months, with the patient reporting only one instance of a mild swelling subsequent to the initial impaction, but no other symptoms. Interestingly, there was no abnormal pocketing or sinus draining at the emergency visit, which generally would be associated with a chronic foreign body reaction. The peri-apical radiograph, although demonstrating the presence of a small radiolucency, was of little diagnostic value, and could mislead the clinician as the incisors were superimposed over the inflammatory lesion.
The sequelae of a penetrating foreign body in the oral cavity is determined by the nature of the material. Inert materials may not cause significant inflammation whereas organic material will cause secondary infection and must be removed to prevent destruction to the surrounding tissues.13 In this instance, the organic material was walled off as a foreign body reaction and remained without producing any significant symptoms. The CBCT was critical in confirming the radio-opacity of the lesion, which coincided with the reported history, and the level at which it was located. The surgeon was thus given the benefit of proper pre-operative planning versus blind exploration.
When managing lesions that appear to be odontogenic, one should not discount a patient's reported history, or exclude foreign bodies from the differential diagnosis even though it may not be obvious on plain films. The importance of 3D imaging highlights their role in the diagnostic pathway.
Conclusion
The patient healed uneventfully with no recurrence of the swelling. A repeat CT was planned for 6 months post-operatively to assess bony regeneration and the need for secondary grafting and membrane placement.
This report underscores the importance that should be placed on the patient history, combined with a meticulous clinical examination. Foreign body impactions are rare in adults, and intra-osseous impactions are even less reported; a wise clinician should consider it, particularly when presented with an unusual clinical picture.