Aidos H, Diogo P, Santos JM Root resorption classifications: a narrative review and a clinical aid proposal for routine assessment. Eur Endod J. 2018; 3:134-145 https://doi.org/10.14744/eej.2018.33043
Fuss Z, Tsesis I, Lin S Root resorption – diagnosis, classification and treatment choices based on stimulation factors. Dent Traumatol. 2003; 19:175-182 https://doi.org/10.1034/j.1600-9657.2003.00192.x
Abbott PV Prevention and management of external inflammatory resorption following trauma to teeth. Aust Dent J. 2016; 61:(Suppl 1)82-94 https://doi.org/10.1111/adj.12400
Di Giorgio G, Salucci A, Sfasciotti GL External root resorption management of an avulsed and reimplanted central incisor: a case report. Dent J (Basel). 2021; 9 https://doi.org/10.3390/dj9060072
Consolaro A, Bittencourt G Why not to treat the tooth canal to solve external root resorptions?. Here are the principles! Dental Press J Orthod. 2016; 21:20-25 https://doi.org/10.1590/2177-6709.21.6.020-025.oin
Abbott PV, Lin S Tooth resorption – part 2: a clinical classification. Dent Traumatol. 2022; 38:267-285 https://doi.org/10.1111/edt.12762
Lin S, Moreinos D, Kaufman AY, Abbott PV Tooth resorption – part 1: the evolvement, rationales and controversies of tooth resorption. Dent Traumatol. 2022; 38:253-266 https://doi.org/10.1111/edt.12757
Andreasen JO Periodontal healing after replantation of traumatically avulsed human teeth: assessment by mobility testing and radiography. Acta Odontol Scand. 1975; 33:325-335 https://doi.org/10.3109/00016357509004637
Talpos-Niculescu RM, Nica LM, Popa M External cervical resorption: radiological diagnosis and literature (review). Exp Ther Med. 2021; 22 https://doi.org/10.3892/etm.2021.10499
Patel S, Foschi F, Condon R External cervical resorption: part 2 – management. Int Endod J. 2018; 51:1224-1238 https://doi.org/10.1111/iej.12946
Umashetty G, Hoshing U, Patil S, Ajgaonkar N Management of inflammatory internal root resorption with biodentine and thermoplasticised gutta-percha. Case Rep Dent. 2015; https://doi.org/10.1155/2015/452609
Nilsson E, Bonte E, Bayet F, Lasfargues JJ Management of internal root resorption on permanent teeth. Int J Dent. 2013; https://doi.org/10.1155/2013/929486
Abbott PV Pulp, root canal and peri-radicular conditions. In: Ahmed HMA, Dummer PMH : Wiley; 2022
Dental Resorption. From Diagnosis to Management: An Update for the GDP Lucy Walker Jay-Krishan Pandya Steven Fletcher Dental Update 2025 51:9, 653-656.
Authors
LucyWalker
Dental Core Trainee, Department of Oral and Maxillofacial Surgery, Pinderfields Hospital.
Dental resorption is a physiological or pathological process that may be initiated and propagated by various mechanisms, including mechanical, surgical, thermal or chemical injury. It refers to non-bacterial destruction of dental tissue resulting from clastic cell activity. It is predominantly asymptomatic in the permanent dentition and may be misdiagnosed and/or poorly understood. This article describes the different types of dental resorption, the features of each and a guide on how to manage them. Some interesting cases are also highlighted.
CPD/Clinical Relevance: It is important to understand, identify and diagnose different types of resorption.
Article
Dental resorption refers to non-bacterial destruction of dental tissue resulting from osteoclastic cell activity.1 It is predominantly asymptomatic in the permanent dentition and may be misdiagnosed and/or poorly understood. Dental resorption can occur both internally and externally and is known to be initiated and propagated by many factors. Pulpal necrosis, trauma, periodontal treatment, orthodontic treatment and tooth whitening agents are the most commonly described causative agents.2 Root resorption in the permanent dentition is caused by osteoclast-like cells called odontoclasts. Cementum and predentine usually protect the root surface and typically do not undergo resorption as they contain potent inhibitors of resorption.3 However after an initial stimulus, the dentine can be exposed and odontoclasts can bind and initiate the resorptive process.3 Resorption will continue while the stimulus is present.
Resorption is generally classified as internal or external resorption and is further classified based on the site, nature and pattern of the resorptive process.4 External resorption includes inflammatory, replacement, cervical and surface. Internal resorption includes inflammatory and replacement.5
External resorption
External inflammatory resorption
External inflammatory resorption (EIR) occurs when there has been a loss of cementum of the root surface following trauma, alongside the root canal system becoming infected with bacteria.
The intracanal bacteria and their endotoxins are able to reach the periodontal ligament (PDL) more easily as a result of the loss of cementum, which can lead to EIR.6 Factors that may initiate EIR include replantation of avulsed teeth, intentional auto replantation and autogenous tooth transplantation.7 Radiographically, EIR is characterized by loss of tooth substance together with a radiolucency involving the adjacent PDL and bone. Clinically the tooth will not respond to pulp sensibility tests but there are usually no symptoms.6 EIR is a deteriorating lesion that, if not diagnosed and treated quickly and properly, could result in the gradual destruction of tooth structure and ultimately tooth loss.8 In cases where the resorptive process is established, the use of a corticosteroid–antibiotic intracanal medicament (e.g. Ledermix Dental Paste, Henry Schein, Kent) has been shown to be useful in the management of these lesions, followed by root canal therapy once it has been confirmed the resorptive process has ceased.6
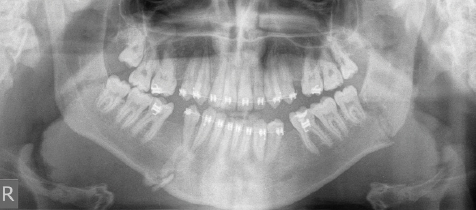
An interesting cause of external inflammatory resorption was seen in a 20-year-old male patient who was part-way through fixed orthodontic treatment. During this treatment, he sustained trauma resulting in fractures to the left angle and right body of the mandible (Figure 1).
Figure 1. DPT taken following mandibular fractures showing fracture to the left angle and right body of the mandible.
These fractures were fixed with metal plates (Figure 2) and the orthodontists were made aware of the injuries at his next appointment. He did not attend orthodontic appointments for over a year following this owing to leaving the country; however, when he returned, his GDP noted external resorption on the distal aspect of the LR4 as an incidental finding. The tooth was asymptomatic, percussion tests were normal and there was a negative response to vitality testing, all suggestive of external inflammatory resorption.
Figure 2. Post-operative DPT following fixation of mandibular fractures.
Radiographically, the lamina dura is not present on the distal aspect of the root of the LR4, and an unclear root outline is present, which is again suggestive of this type of resorption (Figures 3 and 4).17 Initially it was thought that the fracture fixation and screw positioning may have caused iatrogenic damage to the PDL; however, radiographic assessment showed the position of the screws were placed distant from the LR4 to avoid this. The most likely causative agent, therefore, is the fracture of the right body of the mandible, which disturbed the PDL.
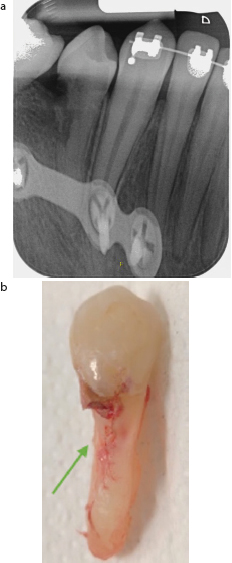
Figure 3. DPT taken 2.5 years after the fracture showing external resorption LR4.Figure 4.
(a) Peri-apical taken 2.5 years after fracture showing external resorption LR4. This clearly shows the screw placement away from LR4. (b) Photograph taken following simple extraction of LR4 showing resorption defect (shown by the green arrow).
External replacement resorption
External replacement resorption, a distinctive dental resorption form, involves the union of the tooth root with surrounding alveolar bone. It is often associated with factors such as trauma (particularly avulsion injuries) or infection during dental development. Ankylosis is the initial process and is defined as loss of the PDL, whereby there is effectively fusion of the alveolar bone and cementum. It is understood that ankylosis occurs when greater than 20% of the root surface is damaged.10 Fusion of the tooth to the alveolar bone prevents physiological tooth movement, resulting in functional and aesthetic concerns. Ankylosis is recognized radiographically by a lack of lamina dura and PDL. Clinically, these teeth will have a metallic or higher pitched sound on percussion.11 Unlike other types of resorption, replacement resorption usually cannot be treated effectively, and often results in extraction of the tooth or burial of the root to support an overdenture.12
External cervical resorption
External cervical resorption is usually caused by trauma; however, factors such as orthodontic treatment and internal bleaching have also been discussed.13 It is one of the least understood types of external resorption and occurs most frequently in upper anterior teeth. It begins on the root surface immediately below the epithelial attachment and the coronal aspect of the alveolar process.14 Clinically, the lesion often begins asymptomatically and is usually discovered at clinical or radiographic check up. A pink spot may be observed in the cervical third of the tooth, which is pathognomonic of cervical resorption, owing to the high vascularity of the tissue seen through the enamel.15 In more advanced cases, patients may report symptoms similar to those of reversible or irreversible pulpitis, as the defects may be in close proximity to, or invade the pulp chamber. In the initial stages of the lesion where there is no involvement of the pulp, vitality tests are normal.16 Owing to this, the diagnosis can be difficult as caries can present similarly. In cases where the defect is supra-crestal and superficial, surgical repair without initiating root canal treatment is indicated. With regards to more extensive lesions involving the pulp, vital pulp therapy or root canal treatment may be indicated.14
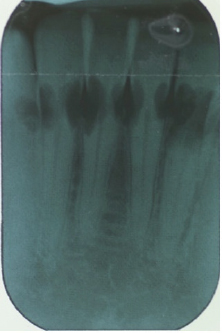
A case of external cervical resorption with idiopathic origin was seen in a 30-year-old female attending an orthodontic consultation. The peri-apical taken (Figure 5) shows radiolucencies affecting the cervical root third of all lower anterior teeth. These teeth were asymptomatic, and this was noticed as an incidental finding. The patient reported no previous orthodontic treatment, no injuries to the teeth or mandible, and no use of tooth whitening agents.
Figure 5. Peri-apical taken at initial presentation showing large radiolucencies affecting mesial and distal aspects of the lower anterior teeth
Unfortunately, this shows a case of substantial external cervical resorption that had progressed to a point at which the teeth were unrestorable and so were due to be extracted and replaced with implants. A differential diagnosis for these lesions could be caries; however, the teeth appeared clinically sound. Given the pink hue at the cervical margin (Figure 6), these teeth can be confidently diagnosed as having external cervical resorption of idiopathic origin.
Figure 6. Photograph taken at initial presentation showing the lingual aspect of the lower anterior teeth to be clinically sound. However, a pink hue can be seen affecting the lingual surface of the LR2 at the gingival margin (shown by the green arrow).
External surface resorption
External surface resorption involves only the outer surface of teeth and occurs as small areas of resorption on cementum that may occasionally progress into dentine.17 Surface resorption is selflimiting because there is no contamination by bacteria and thus, does not have a progressive stimulant. It is usually caused by an injury to the cementum or PDL. Clinically there are no symptoms or signs of surface resorption and radiographically, it is not usually seen, hence why is it unlikely to be diagnosed. There is no management for surface resorption owing to it being self limiting; however, if the root canal becomes infected during the injury, the resorption will progress to external inflammatory resorption and should then be treated as such.9
Internal resorption
Internal inflammatory resorption
Internal inflammatory resorption is usually associated with chronic pulpal inflammation. It is initiated within the pulp space and involves loss of dentine. It is an asymptomatic process that is usually detected on routine radiographs as an oval-shaped increase in the size of the pulp chamber. It is important to note the presence or absence of the tramlines of the pulp chamber as this helps to differentiate internal resorption from external.18 If the lesion becomes more advanced, it may cause symptoms when it progresses to apical periodontitis. Vital pulp tissue is required for this process to occur, and so when the pulp is completely necrosed, the resorption defect will not worsen; however, apical periodontitis will develop.19 Root canal treatment must be initiated as soon as possible once these lesions are diagnosed to prevent further progression of the defect.18 If diagnosed and treated correctly, the management is fairly simple and has a reasonable prognosis.
Internal replacement resorption
Internal replacement resorption is rare and occurs when the pulp and dentine are replaced by bone. It is thought to occur following trauma or insult to the pulp, and many dentists may be unaware of this type of resorption. Clinically, these teeth may be discoloured or have a pink hue. The tooth is usually asymptomatic, and this type of resorption is often detected during routine radiographic examination.20 It can occur anywhere within the root canal system and usually presents as an irregular radiolucency with a mottled or clouded appearance.21 Eventual extraction of these teeth is the most likely management, as usually diagnosis is not caught early enough for root canal treatment due to the lack of signs and symptoms.9
Conclusion
This article has discussed the different types of resorption, the causes behind them and management options (Table 1). Timely and accurate diagnosis followed by the appropriate treatment is crucial to provide the affected tooth with the best prognosis. Where appropriate, clinicians may refer these cases to a specialist or secondary/tertiary care setting; however, it is important to be aware of the types of resorption to be able to discuss this with patients, and manage causative agents in an acute situation. As highlighted by the cases, it is also important to be aware of unusual causes of resorption and to closely monitor teeth involved in dento-alveolar trauma.
Type of resorption
External inflammatory
External replacement
External cervical
External surface
Internal inflammatory
Internal replacement
Clinical features
The tooth is likely to have a normal colour; however, it may change if the pulp is involved. Mobility may be increased, and percussion tests are normal. Vitality tests usually show no response unless the resorption is caused by a non-bacterial factor (e.g. pressure)
The tooth is likely to have normal colour. There will be loss of physiological mobility and a high pitched/metallic sound on percussion. Vitality tests usually show no response
The tooth will have pink discolouration around the cervical region. Mobility may be increased, and percussion tests will be normal. Normal response to vitality testing, unless lesion is close to pulp, in which case the tooth will be hyperresponsive, or there is no response if the tooth is non-vital
The tooth will appear normal clinically. There will be normal mobility, normal percussion testing and normal vitality
The tooth may have pink discolouration if the lesion is coronally situated. Mobility will be normal and percussion tests normal. Vitality tests will show a normal response in active lesions; however, may be non-responsive in extensive lesions
The tooth may have pink discolouration if the lesion is coronally situated. Mobility will be normal and percussion tests normal. Vitality tests will show a normal response in active lesions; however, may be non-responsive in extensive lesions
Radiographic features
Loss of lamina dura with irregular saucershaped lesions and adjacent peri-radicular radiolucency
Irregular lesions around root surface, loss of lamina dura, absence of radiolucency of the periodontal ligament
Radiolucency of the cervical third of the root
Nil
Expansion of canal, usually symmetrical with well-defined margins
Irregular expansion of canal. Pulp space may be obliterated with radiopacities within the canal
Management
Corticosteroidantibiotic intracanal medicament followed by root canal therapy once lesion has stopped progressing
Monitoring, burial of the root or extraction of tooth
Surgical repair in cases where the defect is superficial and supra-crestal, vital pulp therapy or root canal treatment in cases where the pulp is involved
Nil
Root canal therapy
Root canal therapy; however, usually this type of resorption is not detected early enough and extraction is often indicated