Holland N. Recent developments in Bell's palsy. Br Med J. 2004; 329:(7465)553-557
Oosterveer D, Bénit C, de Schryver E. Differential diagnosis of recurrent or bilateral peripheral facial palsy. J Laryngol Otol. 2012; 126:833-836
Baxter A. Dehiscence of the Fallopian canal an anatomical study. J Laryngol Otol. 1971; 85:587-594
House J, Brackmann D. Facial nerve grading system. Otolaryngol Head Neck Surg. 1985; 93:146-147
Woodhouse N, Gok G, Howlett D, Ramesar K. Warthin's tumour and facial nerve palsy: an unusual association. Br J Oral Maxillofac Surg. 2011; 49:237-238
Bell C. XXVIII. On the nerves; giving an account of some experiments on their structure and functions, which lead to a new arrangement of the system. Phil Trans R Soc Lond. 1821; 111:398-424
Peitersen E. Bell's palsy: the spontaneous course of 2,500 peripheral facial nerve palsies of different etiologies. Acta Oto-Laryngol. 2002; 122:4-30
McCaul J, Cascarini L, Godden D, Coombes D, Brennan P, Kerawala C. Evidence based management of Bell's palsy. Br J Oral Maxillofac Surg. 2014; 52:387-391
Morales D, Donnan P, Daly F, Staa T, Sullivan F. Impact of clinical trial findings on Bell's palsy management in general practice in the UK 2001–2012: interrupted time series regression analysis. Br Med J Open. 2013; 3
Murakami S. Bell palsy and herpes simplex virus: identification of viral DNA in endoneurial fluid and muscle. Ann Intern Med. 1996; 124:63-65
Fujiwara T, Hato N, Gyo K, Yanagihara N. Prognostic factors of Bell's palsy: prospective patient collected observational study. Eur Arch Oto-Rhino-L. 2013; 271:1891-1895
Masterson L, Vallis M, Quinlivan R, Prinsley P. Assessment and management of facial nerve palsy. Br Med J. 2015; 1-5
Sullivan F, Swan I, Donnan P, Morrison J, Smith B, McKinstry B Early treatment with prednisolone or acyclovir in Bell's palsy. N Engl J Med. 2007; 357:1598-1607
Madhok V, Gagyor I, Daly F, Somasundara D, Sullivan M, Gammie F, Sullivan F. Corticosteroids for Bell's palsy (idiopathic facial paralysis). Cochrane Database Syst Rev. 2016; 7
Gagyor I, Madhok VB, Daly F, Somasundara D, Sullivan M, Gammie F, Sullivan F. Antiviral treatment for Bell's palsy (idiopathic facial paralysis). Cochrane Database Syst Rev. 2015; 11
Murakami S, Hato N, Horiuchi J, Honda N, Gyo K, Yanagihara N. Treatment of Ramsay Hunt syndrome with acyclovir-prednisone: significance of early diagnosis and treatment. Ann Neurol. 1997; 41:353-357
Lieberthal A, Carroll A, Chonmaitree T, Ganiats T, Hoberman A, Jackson M The diagnosis and management of acute otitis media. Pediatrics. 2013; 131:e964-e999
Facial nerve palsy is the most frequently occurring cranial neuropathy reported to affect 1 in 60 people during their lifetime. An important step in examining these patients, is establishing whether the palsy is caused by an upper or lower motor neurone. Of the many potential aetiologies, Bell's palsy is the most frequently occurring lower motor neurone lesion. The prognosis for this is good, with approximately 85% of patients making a full recovery within three weeks. The aims of this article are to review the appropriate anatomy, potential causes of facial nerve palsy and describe a recommended assessment and management strategy for these patients.
CPD/Clinical Relevance: To inform readers of the variety of causes of facial nerve palsy and present the evidence-based management.
Article
Facial nerve palsy is the most frequently reported cranial neuropathy and has a multitude of potential aetiologies. There is a reported incidence in the UK of 20 per 100,000, with 1 in 60 people being affected during their lifetime.1 Improved outcomes are associated with early diagnosis and treatment, however, it is worth noting that, in many cases, investigation fails to yield a diagnosis.2 Given the high incidence of facial palsy, dental practitioners should be aware of how to assess and appropriately manage a facial nerve palsy. Most importantly, dental practitioners may play a significant role in quickly identifying cerebrovascular accidents (stroke) or transient ischaemic attacks (TIA) and urgently referring via 999 for medical attention.
Anatomy
A good understanding of anatomy is essential for interpreting the presenting signs and symptoms. The facial nerve, cranial nerve number VII, develops from the second pharyngeal arch and, as such, supplies motor and sensory innervation to the muscles formed by the second pharyngeal arch (Table 1).
Function
Supplies
Motor
Muscles of facial expression (frontalis, orbicularis oculi, buccinators and orbicularis oris), also posterior belly of digastric, stylohyoid muscle and stapedius muscle of the middle ear
Sensory
Taste to anterior two-thirds of tongue and sensation around the external auditory meatus
Parasympathetic
Secretomotor parasympathetic fibres to lacrimal, submandibular and sublingual glands
The facial nerve originates at the junction of the pons and medulla in the brain stem, passing laterally through the cerebellopontine angle and then proceeding along a complex course intra- and extra-cranially.
Following emergence from the pons, the nerve then traverses through the internal auditory canal together with the acoustic nerve. It enters its own canal, the Fallopian canal, within the temporal bone, which is immediately beneath the lateral semi-circular canal. The Fallopian canal is the longest bony canal through which a nerve passes and 25–55% of post-mortem specimens show that the bone of the Fallopian canal has a dehiscence present, suggesting its vulnerability at this stage to middle ear infections.3 The facial nerve then exits the skull at the stylomastoid foramen.
In exiting the stylomastoid foramen, a sensory branch is given off which supplies part of the external acoustic meatus and tympanic membrane. It then passes between the posterior belly of the digastric and the stylohyoid muscle, providing innervation to both. It then enters the parotid, passing between the deep and superficial lobes. Here it divides into two main branches, the superior temporofacial and the inferior cervicofacial branches, commonly known as pes anserinus (duck foot). These then subsequently divide to form the final five branches (Figure 1 and Table 2).
Figure 1. Branches of the facial nerve.
Ten Zebras Bashed My Car
T:
temporal
Z:
zygomatic
B:
buccal
M:
mandibular
C:
cervical
Determining whether a motor neurone lesion is upper or lower
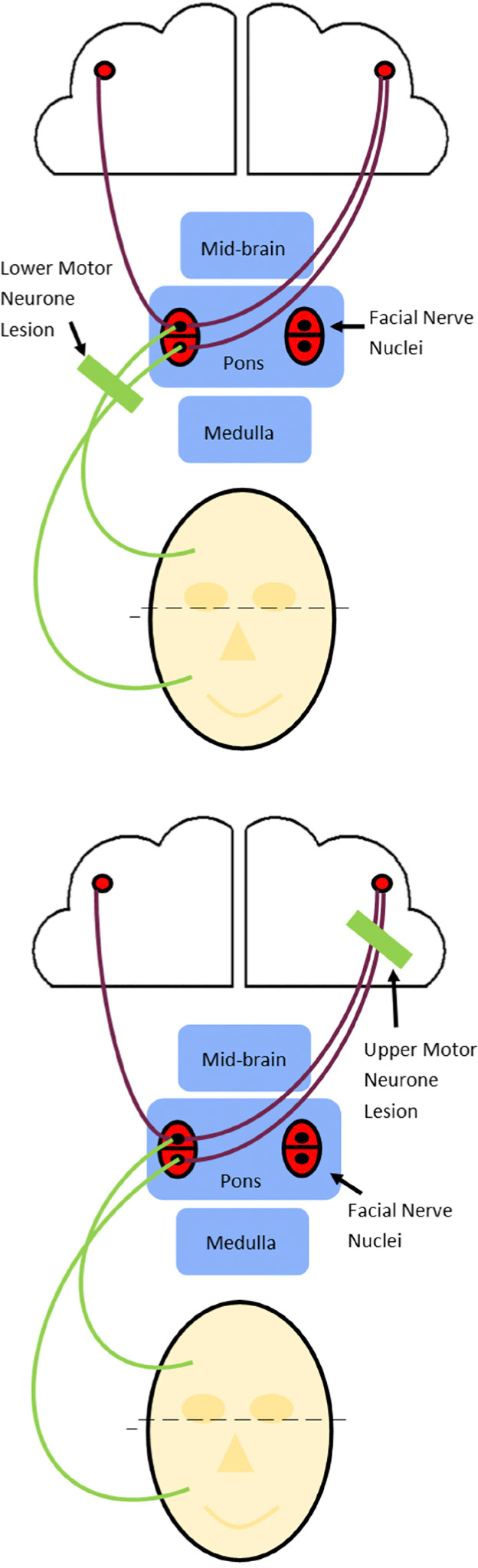
The first step is to determine whether paralysis is as a result of an upper (UMN) or lower motor neurone (LMN) lesion (Figure 2). An upper motor neurone lesion occurs above the facial nerve nucleus, situated in the pons, whereas a lower motor neurone lesion occurs below this.
Figure 2. Bicortical supply to frontalis.
UMN
An UMN lesion is most often associated with a cerebrovascular accident, however, there are other causes (Table 3). The forehead has bi-cortical innervation (supply from both ipsilateral (same side) and contralateral (opposite side) cortices). Therefore, if paralysis is caused by an UMN lesion, the forehead is spared due to the ipsilateral (same side) nerve supply to frontalis. This can be assessed by asking patients to raise their eyebrows; sparing of forehead movement confirms an upper motor neurone lesion. An urgent referral to A&E may be required at this stage to assess the need for thrombolysis in the management of a stroke. There are other red flags requiring urgent medical attention (Table 4).
Upper motor neuron lesion (limb weakness, ataxia, hyperreflexia)
Features suggestive of neoplasia (slowly progressing lesion, painful facial paralysis, pain within the distribution of the facial nerve, suspicious head and neck lesion, unilateral hearing loss, previous head and neck cancer
Paediatric patients
Bilateral facial paralysis
Systemic upset
No improvement after 3 weeks
Recurrent Bell's palsy
Association with a rash elsewhere/generally unwell
LMN
LMN lesions result in weakness of all muscles of facial expression on the same side as the lesion, therefore patients cannot raise their eyebrows, and eye closure and blinking is impaired. This is due to the lesion impairing both the ipsilateral and contralateral nerve supplies. If a LMN lesion is suspected, the muscle groups supplied by the facial nerve can be assessed by asking the patient to complete specific tasks (Table 5).
Raise their eyebrows
Frontalis supplied by temporal branches
Close their eyes
Temporal and zygomatic branches supplying orbicularis oculi
Grin showing their teeth and blow out their cheeks
Buccal and marginal mandibular branches
In addition to this, the following are required:
A full cranial nerve examination: This will aid in excluding a lesion originating at the pons and thereby compressing the facial nerve at its origin.
Ear examination: The facial nerve runs in close proximity to the external auditory meatus and therefore can compromise the facial nerve. The external ear should be assessed for vesicles which would suggest herpes zoster infection (Ramsay Hunt syndrome). An exudate may indicate suppurative otitis media. When assessing the ear, attention should be paid to the mastoid process, in case of trauma.
Parotid gland examination: Examination of the parotid for any masses which may be compressing on the facial nerve as it traverses the gland. Most tumours (80%) present in the salivary gland are benign but have been reported to cause paralysis.5
Aetiology
A thorough history and examination should have determined whether the cause of facial palsy was an UMN or LMN lesion. From here, the authors will concentrate on the most frequent LMN aetiologies (Table 5).
Assessment
The most frequently used classification for paralysis is the House-Brackmann scale, which was developed in 1985.4 This scoring system (Table 6) allows clinicians to determine the severity of a facial nerve palsy and facilitates a clinician in assessing whether a paralysis is improving or not with time.
Grade
Characteristics
INormal
Normal facial function in all nerve branches
IIMild dysfunction
Slight weakness on close inspectionEye: Complete closure with minimum effortMouth: Slight asymmetry
IIIModerate dysfunction
Obvious but not disfiguring facial asymmetryEye: Complete closure with effortMouth: Slight weakness with maximum effort
IVModerately severe
Asymmetry is disfiguring and/or obvious facial weaknessEye: Incomplete eye closureMouth: Asymmetrical with maximum effort
VSevere dysfunction
Only slight, barely noticeable, movementEye: Incomplete closureMouth: Slight movement
VITotal paralysis
No facial function
Differential diagnosis for facial palsy
Bell's palsy
Presentation
The most frequently occurring LMN lesion was first described by Scottish Surgeon Sir Charles Bell in 1830, eight years after he first described the anatomy of the facial nerve.6 Bell's palsy is a diagnosis of exclusion. The condition usually develops within 24–48 hours, with sudden unilateral lower motor neurone weakness. In 60% of cases, it is associated with post-auricular pain.7 There may also be hyperacusis (increased sensitivity to certain frequencies), ipsilateral taste disturbance, and reduced lacrimation.8 It was previously believed to occur most frequently in the 30–45-year-old group, however, a recent database study has shown that Bell's palsy is most likely to occur in those over 70 years of age.9
Examination
On examination, gross drooping of the eyebrow and corner of the mouth is present. The exact aetiology isn't completely understood but is believed to result from oedema of the facial nerve caused by reactivation of herpes simplex type 1 and herpes zoster virus.10 Viral DNA has been recovered from the facial nerve during acute palsy to support this theory.1
Prognosis
The prognosis for Bell's palsy is good, with approximately 85% of patients making a full recovery within three weeks.7 The remaining 15% tend to partially recover within three to six months. Incomplete or partial weakness at presentation is believed to affect outcome, with residual muscle function improving the long-term recovery rate.8 A study of prognosis demonstrated that facial grading scores recorded at one week is predictive of long-term recovery.11 Interestingly, gender, ethnicity, diabetes and hypertension apparently have no effect on long-term recovery.
Management
There are a few main aims of management. Firstly, if the cornea is exposed due to reduced blink reflex (House-Brackmann score IV–VI), then protection from corneal ulceration is required. During the day, artificial tears are recommended hourly and eye ointment with a secure dressing is required at night to protect the globe.12 Medical intervention is supported with the use of corticosteroids, with previous trials demonstrating that early treatment with corticosteroids is associated with an improved outcome at 3 and 9 months.13 This treatment is most effective within the first 72 hours, though it is an accepted management technique within the first week.12 The combination of corticosteroids with antivirals for varying degrees of palsy is supported by a Cochrane systematic review.14, 15
Two different prednisolone regimens are recommended by NICE and each is appropriate:16
25 mg twice daily for 10 days; or
60 mg daily for five days followed by a daily reduction in dose of 10 mg (for a total treatment time of 10 days).
Currently, prednisolone is not present in the dental practitioner's formulary, therefore patients with suspected Bell's palsy should be referred to their general medical practitioner for management. Alternate treatment modalities may include botulinum toxin injections, physical therapy, acupuncture, hyperbaric oxygen, and surgery.17, 18, 19, 20, 21 However, there is a lack of high quality evidence in the literature to support them.
Follow-up
Follow-up is required to monitor symptoms, with patients advised to return sooner if symptoms change or deteriorate. An urgent referral to ENT is required if symptoms have not resolved with 2–3 weeks of corticosteroids.
Ramsay Hunt syndrome
Ramsay Hunt syndrome is the second most common cause of atraumatic peripheral facial paralysis.22 It is described as peripheral facial nerve palsy accompanied by zoster oticus (erythematous vesicular rash on the ear or mouth) and otalgia (ear pain). The pathophysiology is thought to be caused by varicella-zoster virus reactivation involving the geniculate ganglion of CN VII within the temporal bone. Presentation and prognosis for these patients is worse than for Bell's palsy, with only 21% demonstrating full recovery at one year.7 The use of both prednisone and acyclovir within 3 day's onset is indicated.23
Bacterial infections
Bacterial infections are reported to be responsible for 1–4% of LMN lesions.12 The majority are caused by acute otitis media, which presents with acute onset and severe otalgia.24 Patients require specialist assessment and hospital admission.24, 25 Lyme disease is the most common tick-borne infection in both the US and Europe.26 It usually presents between May and October, in relation to increased outdoor activity at this time, in a tick-borne area. In 75% of cases, there is a characteristic erythema migrans rash. If suspected, patients should be referred urgently to a medical practitioner.
Neoplasia
A facial palsy with slow progression is redolent of cancer.12 Cancer may also limit its paralytic effect to certain branches of the facial nerve, causing pain at the same time. It is vital to undertake a head and neck examination to check for cervical lymphadenopathy, parotid masses or scalp lesions. Urgent referral to the appropriate medical specialty is required.
Trauma
Surgery in close proximity to the facial nerve has the potential to cause palsy. This is most frequently seen in cerebellopontine angle, middle ear and parotid gland surgeries.12 Trauma, as a result of facial lacerations, stab wounds and temporal bone fractures may cause a facial palsy. A temporal bone fracture can be diagnosed if peri-orbital bruising (racoon eyes), mastoid bruising (Battle's sign), or blood in the ear canal is present.27
Management of facial palsy for general dental practitioners
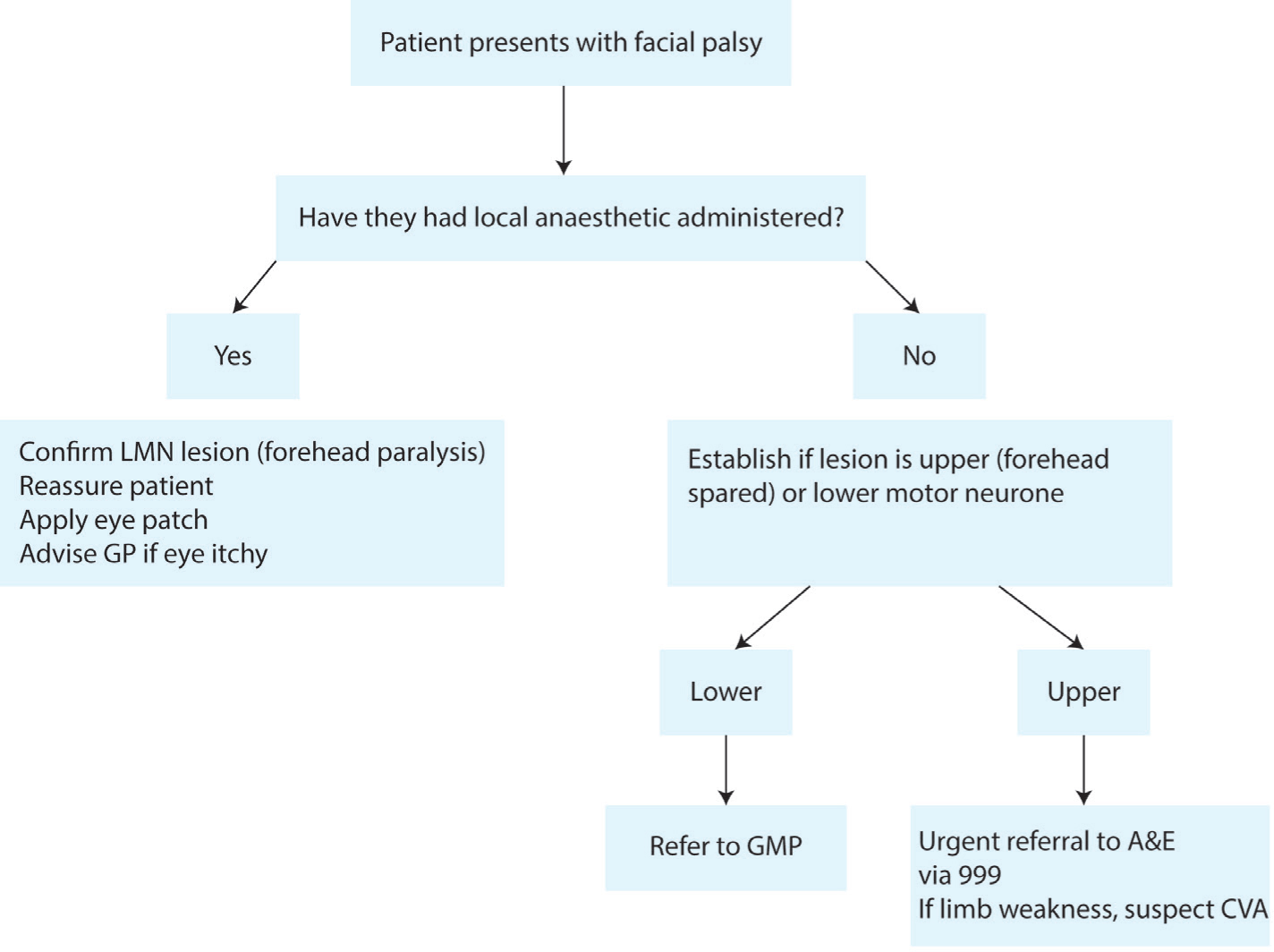
General dental practitioners (GDPs) play an important role in the early detection, prompt referral and management of facial palsy, as patients will often present to their dentist in the first instance. An algorithm is proposed to guide GDPs in the management of patients presenting with facial palsy (Figure 3).
Figure 3. Algorithm for management of facial palsy for general dental practitioners.
Conclusion
Patients may present to a GDP with facial palsy. Prompt treatment is required to maximize outcomes for patients, particularly with Bell's palsy. A thorough and complete examination is essential in aiding diagnosis and providing the most appropriate treatment.