Importance of quality in referral letters sent for potentially malignant oral, head and neck lesions Mital Patel Adeel Qutub Khan Janavikulam Thiruchelvam Dental Update 2025 38:3, 192-198.
Early diagnosis of oral, head and neck cancer is very important. Delay in diagnosis and referral to a specialist unit can result in an enlarged tumour with an increased chance of metastatic spread which will result in upstaging of the tumour, thus worsening the five year survival rate. There is a great need for early identification and referral of potentially malignant lesions by general dental and medical practitioners. Referral letters are the standard and, typically, the sole method of communicating confidential information between two professionals. It is vital that the referral letters sent for potential malignant lesions are of good quality, clearly marked as urgent and contain adequate administrative and clinical data. An audit was undertaken at the Oral and Maxillofacial Department at Barnet and Chase Farm NHS Trust, to examine the quality of referral letters sent for potentially malignant oral, head and neck lesions. The outcome is discussed and a standard referral letter is also proposed if not referring using the standard local cancer network referral proforma.
Clinical Relevance: A good quality referral letter should minimize delay in diagnoses and management of a patient with an oral, head and neck lesion.
Article
Oral, Head and Neck Cancer (OHNC) is a major health problem in many parts of the world. It is the third most common malignancy in the developing world after cancer of the stomach and cervix.1 Incidence of OHNC is low in western countries; however, in the Indian subcontinent and in other parts of Asia it may account for up to 50% of all new malignancies.2 In England and Wales, OHNC accounts for about 2–3% of all new malignancies each year and oral cancer alone makes up almost half of the reported cases.3 Over 90% of oral carcinomas are squamous cell carcinomas, which arise from the oral mucosal lining.2 The mortality and morbidity rate of OHNC is high and the quality of life of the survivors can be compromised with altered speech, chewing, swallowing and breathing. Disfigurement of the face, head and neck is also common, especially when diagnosed in late stages.4 It is therefore important that an early diagnosis is made. Regular screening of the oral tissues and an adequate and timely referral plays a major role in this.
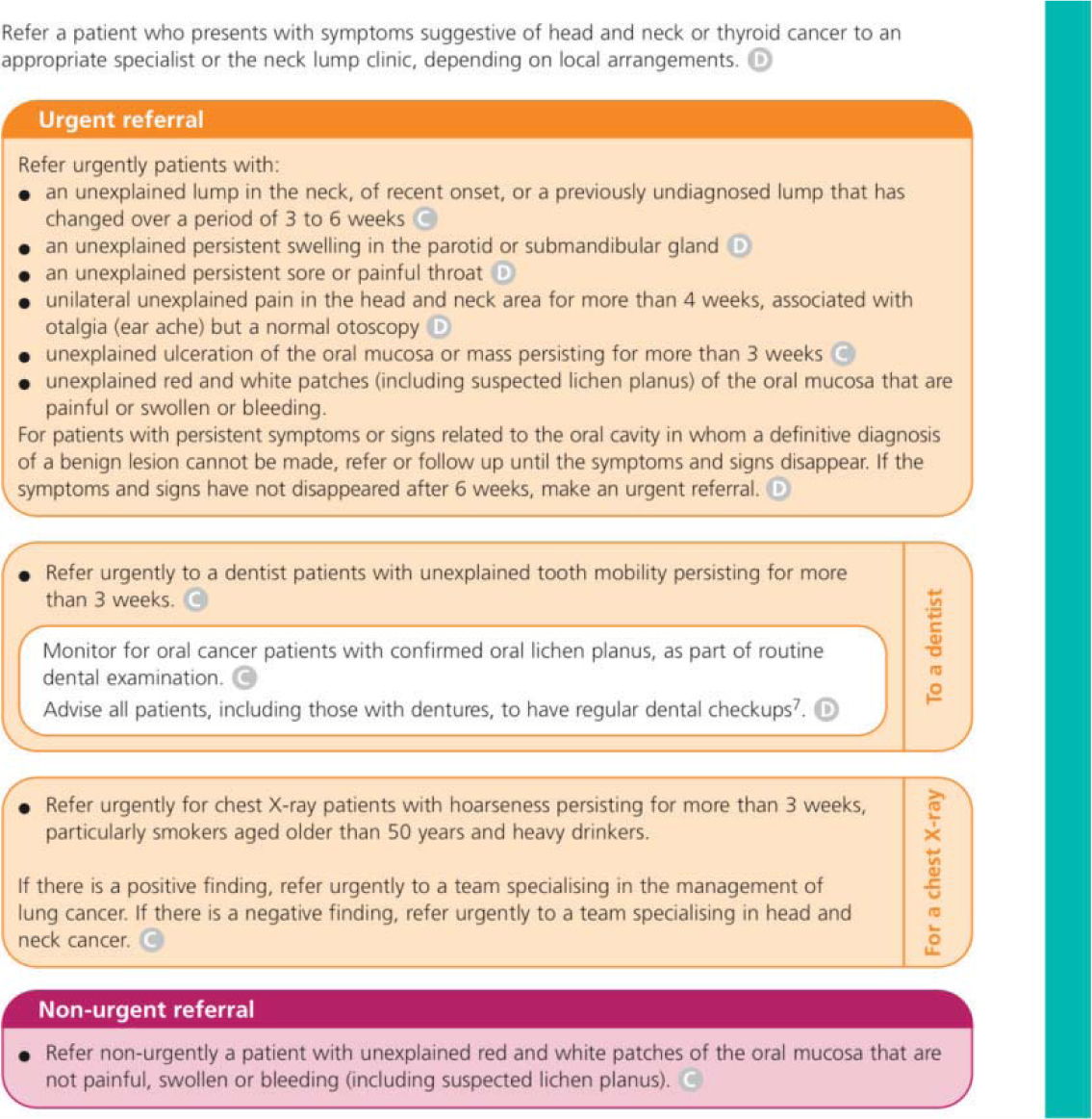
In November 1999, the NHS published a consultation document regarding referral guidelines for patients with suspected cancer.3 The document emphasized that all patients with potentially malignant disease should receive specialist examination within 14 days of referral to the relevant specialist unit. These guidelines became applicable for potentially malignant OHNCs from December 2000. Following review of the consultation document, a subsequent document entitled Referral Guidelines for Suspected Cancer was published by the Department of Health in 2000 which outlined the presenting complaints and the clinical signs and symptoms requiring urgent referral following consultation with their general practitioners (Table 1).3,5 In 2005, the National Institute of Clinical Excellence (NICE) published further clinical guidelines, CG27 (Figure 1), which was an update to the existing Department of Health guidelines based on new research and audits carried out (Figure 2).6 In order to meet the Department of Health two-week referral target successfully, an appropriate referral letter from General Dental Practitioners (GDPs) and General Medical Practitioners (GMPs) is required, clearly highlighting the nature and urgency of the referral.
Urgent Referral required for patients presenting with:
Hoarseness persisting for >6 weeks
Ulceration of oral mucosa persisting for >3 weeks
Oral swellings persisting for >3 weeks
Dysphagia persisting for 3 weeks
All red or red and white patches of the oral mucosa
Unilateral nasal obstruction particularly when associated with purulent discharge
Unexplained tooth mobility not associated with periodontal disease
Unresolving neck masses for >3 weeks
Cranial neuropathies
Orbital masses
The level of suspicion is further increased if the patient is a heavy smoker or heavy alcohol drinker and is aged over 45 years and male. Other forms of tobacco use (chewing Betel, Gutkha, Pan) should also arouse suspicion
Adapted for the Department of Health Referral Guidelines for Suspected Cancer, 2000.
Figure 1. NICE guidelines CG27, Referral guidelines for suspected cancer, 2005.Figure 2. NICE guidelines for referring and managing patients with suspected malignant oral, head and neck lesions. Taken from NICE CG27 document, Referral guidelines for suspected cancer, 2005.
The timely diagnosis and subsequent management of malignant lesions is well known to provide the best prognosis. Dental professionals are ideally situated to recognize potentially malignant lesions in the oral cavity.7 A systematic extra-oral and intra-oral examination of the oral, head and neck region should be an integral part of all routine dental examinations and is considered as the most suitable screening method for malignant and premalignant lesions by the UK screening group. There is evidence that some cases of oral cancer are missed by GDPs.8,9 A study by Cowan and co-workers 199510 found that most GDPs agreed that screening for OHNC should be part of their routine examination. However, only 50% routinely examined the oropharyngeal region. This will therefore delay the diagnosis and subsequent referral of the patient to the Oral and Maxillofacial Department.
Patient factors also play an important role in the early detection, as some patients do not attend regular dental assessments for social and financial reasons.11 The delay in identification, referral and diagnosis will increase the chance of metastatic spread and therefore upstage the disease.5 The five-year survival will therefore reduce from 90% for stage I disease to 30–40% for stage IV disease.12 If there is any concern about either an area of ulceration in the mouth or a white or red patch affecting the oral mucosa, an early opinion should be sought from a specialist to exclude malignancy.2
It is important that, once a suspicious lesion is identified, there is good communication with the specialist centre for early diagnosis and management. Referral letters are the standard and, typically, the sole method of communicating confidential information between two professionals.13,14 They are also an important medico-legal document.15 When used correctly, they can provide a valuable source of information about a patient.16 Referral letters can be either handwritten, typed or filled in on pre-constructed proformas. This should be done as soon as possible after the examination while all the details are fresh in the mind. If there is a suspicion of malignancy, the referral letter should be clearly marked as urgent, faxed to the specialist immediately and a hard copy should be sent by post.17 Good quality referral letters can avoid discontinuity in care, unnecessary repetition of diagnostic tests and poor patient outcomes such as anxiety, dissatisfaction and loss of confidence in healthcare professionals. They can also potentially reduce waiting times and minimize the workload for administrative staff.18
Aims and method
The aim of this retrospective audit was to assess the quality of referrals sent to our department for potentially malignant oral, head and neck lesions and to analyse how the quality of the referral letter affected the time taken from the point of referral to an outpatient appointment being made. The findings were correlated with the recommendations from the Department of Health that all cancer referrals should be seen within two weeks and treated within 62 days. From our database, names of all patients who were newly diagnosed with oral and oropharyngeal cancer during a two-year period (2007–2009) were obtained. Patients who were being regularly reviewed in our clinics for monitoring of a precancerous lesion, and were diagnosed with cancer during their regular follow-up visit, were excluded, and only patients with new referrals in this time frame were included. The referral letters were audited to analyse the information present, based on the key points listed in Table 2. Delay in diagnosis, owing to inadequate information, was calculated.
Administrative Data
Clinical Data
Marked as urgentPatient's namePatient's addressPatient's tel. no.Patient's date of birthPatient's genderPatient's NHS no.Language spoken/Interpreter required or notPrevious visited hospitalReferrer's nameReferrer's address Referrer's tel. no.Referrer's fax no.
Description of siteDiagram of lesion Size of lesion Shape of lesion Duration of lesion Symptoms Clinical appearanceRisk factorsMedical history
Results
In our unit a total of 75 patients were diagnosed with oral, head and neck carcinoma during the two-year period. Of these patients, 17 patients were diagnosed during their regular follow-up visit and were therefore excluded from the audit. A total of 58 referral letters were analysed. Of these, 30 patients were referred using the North London Cancer Network (NLCN) referral proforma. Most of these referrals were from GMPs. All the NLCN referrals were treated as urgent by the administrative staff and outpatient appointments were made for the patients without the need for prioritization of the referral by the consultant. The average time for outpatient appointment for patients referred through the NLCN pathway was 12 days, with a range of 10–16 days. The diagnosis, confirmed by a biopsy, was made within 22 days, with a range of 17–30 days.
Twenty-eight patients were referred using a typed or handwritten letter. These letters required prioritization by the consultant prior to an outpatient appointment being made. Amongst these letters, 12 had most of the details required to help the consultant to triage the letter as urgent and thus attempt to give an outpatient appointment within two weeks of the referral. In patients whose letter did not have the urgency highlighted or a suggestion of cancer, the letters were triaged as routine, and an outpatient appointment was given within 6–8 weeks. The average time taken for an outpatient appointment for patients referred using a typed or handwritten referral letter with the appropriate information was 21 days, with a range of 14–30 days. Confirmation of diagnosis for these patients was done within five weeks, with a range of 24–40 days.
A total of 16 patients, whose letter did not have the necessary information, had a delay in the first outpatient appointment of up to eight weeks, with a range of 6–10 weeks.
Once patients were seen in the clinic and suspected of having cancer there was very little variation, amongst the groups, in the time taken to diagnose and treat the patient.
Discussion
The results of our audit shows that patients referred through the NLCN pathway using the suspected oral, head and neck cancer referral proforma were seen and diagnosed the quickest. It is therefore considered to be the most appropriate method of referral, as most trusts are catered to give appointments within two weeks of referral when referred through this pathway. As these proforma letters are specifically for suspected malignant lesions, they do not need to be prioritized by the consultants, and the patients are directly booked into the outpatient clinics by the administrative staff. This reduces the delay in the time taken to triage the referral letters. However, these referral letters are usually over used or sometimes abused, as only 2–11% of these referrals turn out to be cancer.19,20 These referral forms are mostly used by GMPs and should be encouraged for use by GDPs.
The second most appropriate referral format was a handwritten or typed letter containing adequate administrative data and clinical data, as shown in Table 2. The literature shows that many referral letters are poorly written and do not communicate the necessary information, and in many referrals the urgency is not always obvious owing to inadequate information provided in the referral letter.17 Cowan and co-workers found that, when referring to a specialist, the most frequently used method involved a written description of the suspected lesion; only 16% of GDPs routinely provided information about the size of the lesion and only 8% overall routinely provided a diagram.10 When using this method of referral, it is essential that these letters are clearly marked as urgent or there is the mention of urgency or suspicion of cancer in the text. Letters with the appropriate information were seen and diagnosed quicker than letters that did not have the necessary details. It is, however, difficult to correlate the staging with the delay, as the rate of progression of the disease varies between patients and it is difficult to guess the size of the lesion when the patient presented to the GMP/GDP. Once the patients have been seen in the clinic there is very little variation on further management and any delay in treatment is often during the referral stage. In order to ensure our patients are efficiently managed, as part of the patient care pathway, both medical and dental professionals must take the referrals seriously and send the appropriate letter. Monitoring and auditing the quality of referral letters must form an important part of both primary and secondary health sectors' clinical governance policies.
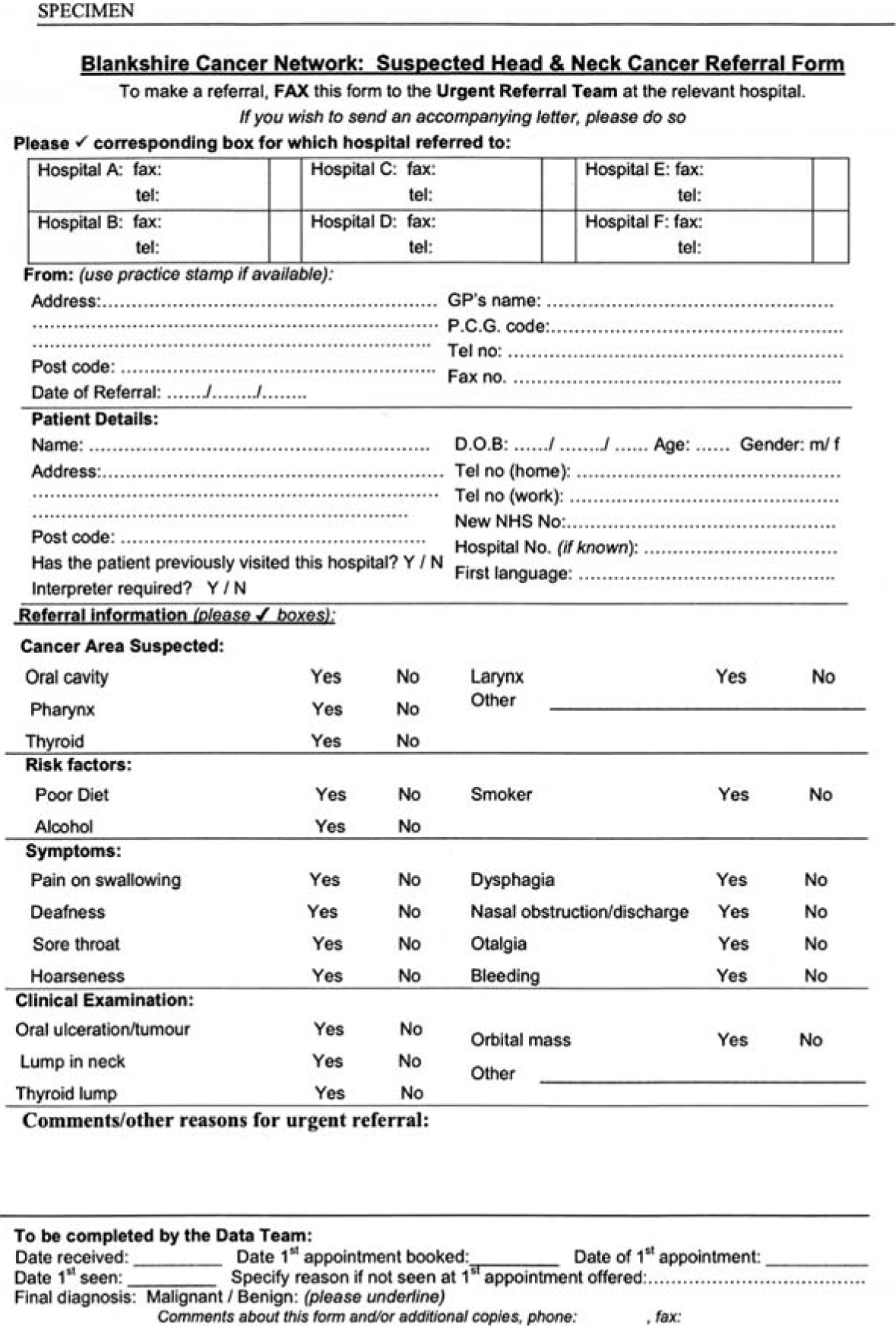
Evidence has shown that typed letters generally contain more information than handwritten ones. Typed letters, or proformas, also increase the referral's legibility and its chances of being read by the hospital consultant.16 A study by Couper and Henbest found that the quality of referral letters improved after the introduction of the proforma letter21 and, similarly, Navarro and colleagues showed statistically significant differences in the quality and quantity of the information found in proforma-based and non-proforma-based referrals.22 Proforma letters, as well as containing more relevant information, are quicker and simpler to complete than typed or written letters,23 making them practitioner friendly. Using a separate proforma specifically for the referral of potential malignant head and neck lesions, such as the Cancer Network Referral Proforma (Figure 3), can also make life easier for hospital-based administrative staff, who would be able to recognize the form and prioritize it accordingly. This may be difficult in a handwritten or typed letter as the administrative staff may not understand the importance of a referral which may state ‘long standing, non-healing ulcer, please see and treat’, especially if the letter is not marked as urgent. Proforma-based referral forms are being increasingly used by many specialist units and some are widely available on the internet or from the Department of Health website, with the intention that these can be customized for local use.3,5
Figure 3. Example of Local Cancer Network Proforma which can be used for referring patients urgently for suspected malignant lesions.
The errors within referral letters vary from minor (lack of basic administrative data) to serious (lack of clinical data or any suggestion of suspected malignancy). Most letters lack clinical detail and those which only consist of ’please see and provide treatment for this patient with a lump’ or worse, ‘please see and treat’ are hardly helpful.5 McConnell and co-workers showed less than half the referrals detailed clinical findings or included information on past medical history, social history, medications or allergies.24 Other studies highlighted that a patient's medical history is poorly covered in referral letters.25 Medical and dental practitioners should appreciate that their documentation of medical problems is not superfluous, since it helps by providing another line of defence against error.26 A good social, family and emotional history is also important, especially in patients with cancer or precancerous lesions.27
Referral letters also play an important role in good record-keeping. When a patient is referred, a copy of the referral letter, the date it was faxed or posted and copies of any replies should all be kept as a record in the patient's record/file. This is not only a legal requirement, but also provides proof against negligence that an appropriate referral for the patient was made. Once referred, the patient should be followed up to ensure that the patient has been sent an appointment or seen within the two-week period. The general practitioner should also expect a timely reply from the specialist centre or hospital following the patient's outpatient appointment.
Dental practitioners are now increasingly involved in the multidisciplinary care of the patient's oral health. It is clear that patients are being increasingly referred between dental practitioners, dental care professionals and specialists with the aim to provide the best treatment for the patient. For this type of team care to be successful, referral letters will play an important role in the exchange of confidential information between professionals regarding the patient. Practitioners should therefore be able to write good quality referral letters which will ensure that an efficient and professional team care approach to modern dentistry is maintained.
Conclusion
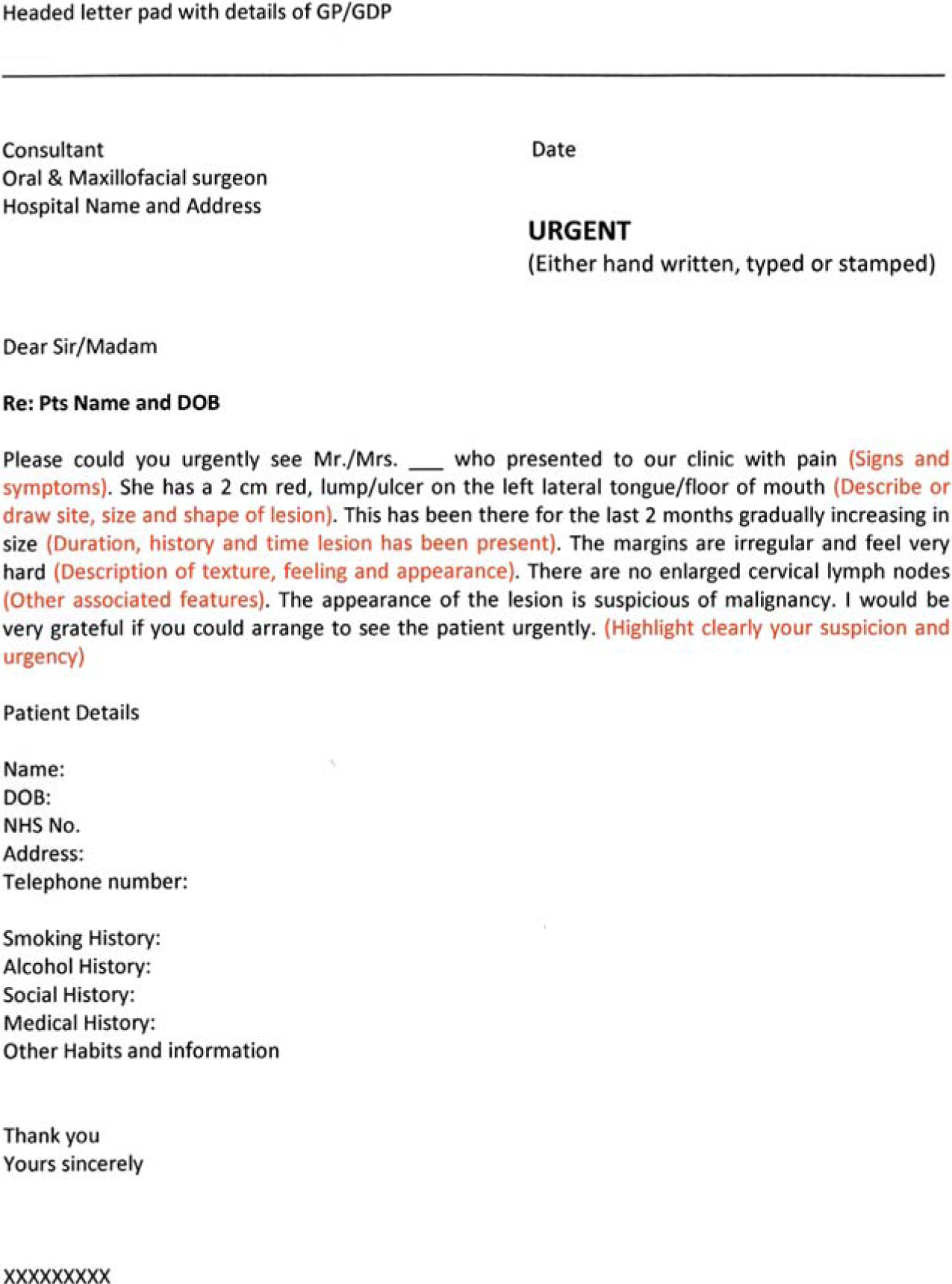
It can be concluded that a referral letter constitutes a major part in the initial pathway of patient care and a poorly written referral letter can result in the delay of treatment for the patient and poorer prognosis. It is vital that the referral letter contains essential administrative data and clinical data (Table 2) to help the consultant prioritize the referral accordingly. Our audit, and the literature, show that proforma-based referrals are the most accurate and result in the least delay between the patient being referred and assessed in the outpatient clinic. GDPs and GMPs should also be aware of their local OHNC network and, where possible, use the Cancer Network referral proforma (Figure 3) designed specifically for referring patients with suspected malignant oral, head and neck lesions. An alternative would be a standard written or typed referral letter with adequate details and the mention of urgency or suspicion of malignancy. An example of an acceptable referral letter is shown in Figure 4. This would enable the consultant to prioritize the referral as urgent and therefore the patient can be seen and treated as soon as possible to get the best possible outcome.
Figure 4. Sample of an adequate handwritten or typed referral letter.