Kay LW, Killey HC. The extraction of teeth: pre-operative assessment. Dent Update. 1973; 1:43-48
Riches S. Vertical-extraction forceps. BDA News. 2012; 4
Muska E, Walter C, Knight A Atraumatic vertical tooth extraction: a proof of principle clinical study of a novel system. Oral Surg Oral Med Oral Pathol Oral Radiol. 2012;
Minimally-invasive tooth extraction: doorknobs and strings revisited! Daniel Saund Thomas Dietrich Dental Update 2025 40:4, 325-330.
Authors
DanielSaund
BDS, MFGDP, MFDS RCPS, MJDF RCS, M.ORAL.SURG
Department of Oral Surgery, Birmingham Community Healthcare NHS Trust, The School of Dentistry, University of Birmingham, St Chad's Queensway, Birmingham B4 6NN, UK
Department of Oral Surgery, Birmingham Community Healthcare NHS Trust, The School of Dentistry, University of Birmingham, St Chad's Queensway, Birmingham B4 6NN, UK
References to ‘atraumatic’ tooth extraction pervade the recent dental literature. This has been largely driven by the increasing demand for bone preservation as osseo-integrated implants increasingly become a mainstay for dental prosthetic rehabilitation. This article introduces the reader to the concept of vertical tooth removal, which aims to avoid socket expansion and thereby minimize trauma to alveolar bone during tooth extraction. Several systems have recently become available and we present our experience with the Benex extractor in particular.
Clinical Relevance: Clinicians should be aware of minimally invasive extraction techniques, their indications and potential advantages.
Article
Legend has it that, in days gone by, the practice of having a tooth ‘pulled’ by one end of a string being tied to the tooth and the other to a doorknob, and then slamming the door closed, was not such an uncommon practice. We are pleased to say that, as a profession, we have long moved on from such crude and unrefined approaches to tooth extraction.
Since the publication of Kay and Killey's article in the inaugural issue of this journal,1 extraction techniques have evolved by revisiting the principle of tooth ‘pulling’ (as was the case with the aforementioned home remedy), albeit with slightly more finesse and technical ingenuity, thanks to several extraction systems that have become available over the past decade. The basic principle of this technique is to extract the tooth exclusively by pulling along its long axis (vertical extraction). We will discuss the rationale for this technique and provide a detailed description of our experience with one of the available systems.
Doorknobs and strings aside, the idea of vertically extracting a tooth is not new, and special forceps had been available in the latter half of the eighteenth century to achieve this.2 The forceps were advertised in the Mercure de France, a French magazine for elegant society discussing intellectual debates of the time. The advertisement claimed that the new instrument ‘causes less tearing and consequently less pain than ordinary instruments’ when tooth extraction was necessary. The advert went on to suggest that the instrument was not only useful for surgeon-dentists, but also ‘to those who have the courage to operate on themselves’!2 Apparently, these instruments fell out of favour mainly because they relied on the presence of neighbouring teeth to the one to be extracted and had complex construction, meaning that they were difficult and time consuming to use. In addition, multi-rooted teeth could not be removed vertically.2
Interestingly, some of these limitations still have to be considered with the currently available systems. The development of these novel systems has undoubtedly been driven by the desire to preserve as much bone as possible in the context of implant therapy, and references to ‘atraumatic’ extractions now pervade the literature. Although the term ‘atraumatic extraction’ has never been clearly defined, it is clear that, with the possible exception of orthodontic extrusion, no extraction technique can be completely atraumatic. We therefore feel that the term ‘minimally-invasive’, which is also used in other areas of surgery, would be more appropriate. The amount of trauma sustained by the periodontal tissues varies considerably in current practice, ranging from the reflection of a mucoperiosteal flap and surgical removal of bone to retrieve roots, to an uncomplicated extraction of a single-rooted tooth using forceps, luxators and/or periotomes.
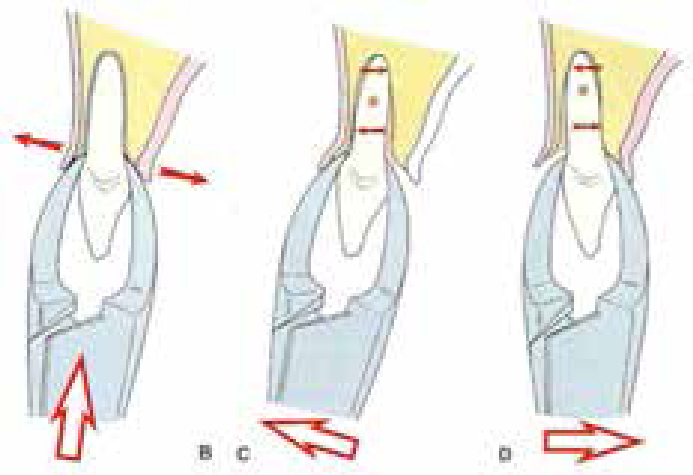
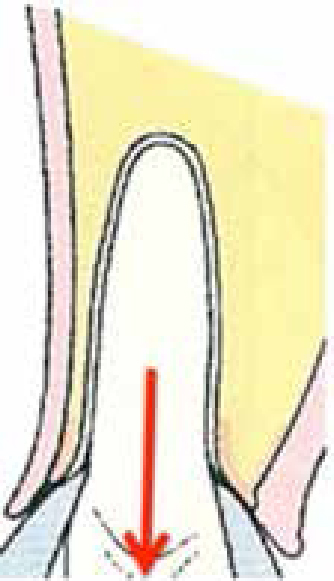
Bony trauma is difficult to avoid as the very principle of forceps extraction is socket expansion (Figure 1) and even a successful extraction using luxators or periotomes will traumatize alveolar bone to some extent, as any movement in a horizontal direction or a rotation, unless it is a perfectly circular root, will at a minimum result in some bone expansion. However, at least conceptually, there is no direct trauma to the socket walls when severance of the periodontal ligament is achieved by pulling a conical root in an axial direction from its socket in a controlled and measured manner (Figure 2).
Figure 1. Conventional extraction processes utilize horizontally directed forces for tooth removal (taken from Hupp JR. Principles of uncomplicated exodontia. In: Contemporary Oral and Maxillofacial Surgery 5th edn. Hupp JR, Ellis III E, Tucker MR (eds). St Louis: Mosby Elsevier, 2008: p117, used with permission).Figure 2. Vertical extraction generates force in a coronal direction only.
This is the central tenet of the vertical extraction systems available today, which are all inspired by a well-established kitchen tool (Figure 3).
Figure 3. Well established instrument that is used for vertical extraction of corks from bottles with predictably high success rates! The same principle is used with vertical tooth extraction.
Given the plethora of different corkscrew devices in people's kitchens, it will not surprise the reader that more than one system for vertical extraction has become available over the past decade. To our knowledge, these include the following three systems:
Benex;
Easy X-TRAC;
Apex Control.
The common feature of these systems is the use of a screw that is placed in the root of the tooth to be extracted and a mechanism is then applied that allows the extraction force to be transmitted to this screw. The currently available systems differ in the specifics of this latter mechanism. We describe here our extensive experience with one of the available systems (Benex extractor, Hager & Meisinger GmbH, Neuss, Germany and Helmut Zepf Medizintechnik, GmbH, Tuttlingen, Germany) which, in our opinion, has several distinct advantages in terms of its flexibility.
It should be made clear from the start that because of the extraction principle, the use of any vertical extraction system is limited to single-rooted teeth or multi-rooted teeth with non-divergent roots. However, divergent roots can of course be sectioned and approached separately in some cases.
The Benex extractor
Benex extraction – the basics of the procedure
The basic Benex system consists of the Benex extractor itself (Figure 4a), a set of diamond burs (1.6 and 1.8 mm), a set of self-tapping screws, a pullstring and a sectional impression tray (Figure 4b).
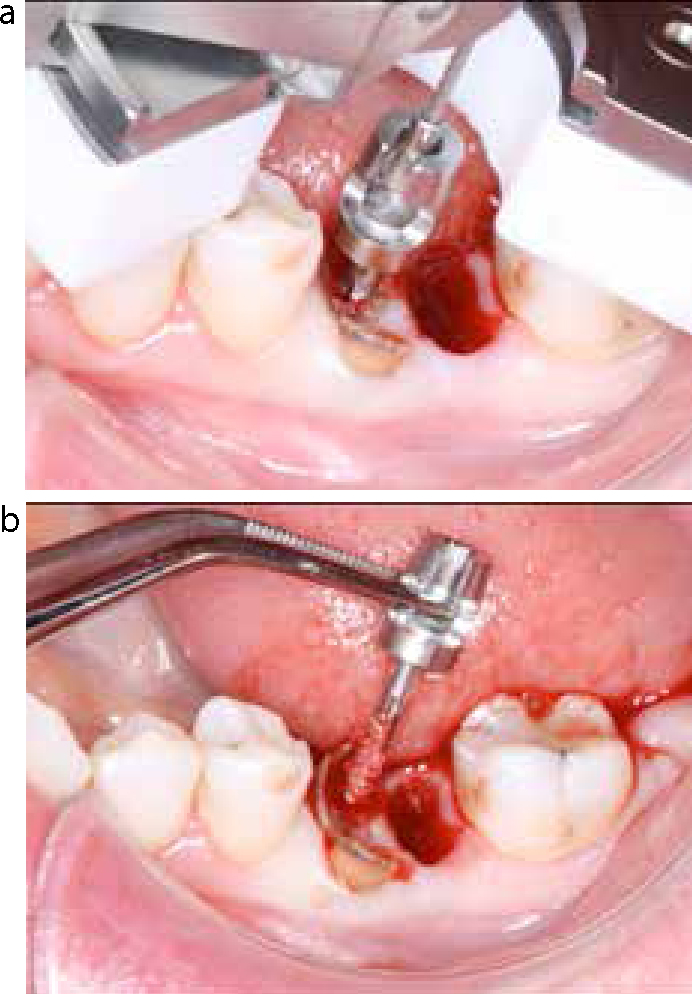
The following case demonstrates how the Benex extractor can be used to remove a carious upper second premolar. It can be seen from the radiograph (Figure 5a) that minimal coronal tissue remains which would necessitate extensive use of luxation, or a transalveolar surgical procedure. It is possible to remove this large retained root with the Benex system and this is demonstrated. The first step in the extraction procedure is the preparation of a screw-hole in the centre of the tooth using a diamond bur (1.6 mm or 1.8 mm diameter), commonly (but not necessarily) following the course of the centrally located pulp canal. Removal of carious tissue is optional, but may be indicated to provide better overview (Figure 5a –d). A self-tapping anchor screw is then inserted until firmly secured into the root (Figure 5e).
The force required to remove the root will be counterbalanced against the adjacent teeth or edentulous ridge, depending on the clinical scenario. In this case, the Benex extractor is stabilized directly by the adjacent teeth (Figure 5f). To achieve proper placement and support for the Benex extractor, it may be necessary to position the sectional impression tray using some silicone impression material to stabilize its location. The pullstring is then located within the head of the anchor screw. The T-bar at the other end of the pullstring is positioned into one of three notches on the Benex extractor (Figure 5f).
Gradual force is applied to the tooth root by turning the knob at the end of the extractor clockwise, which results in a controlled severance of the periodontal ligament and emergence of the retained root from its alveolus (Figure 5g, h, i).
Benex extraction – how well does it work?
At Birmingham Dental Hospital we have been using the Benex system for extractions of teeth deemed unsuitable for forceps extraction, and we have performed an observational study in order to document the success rate of this technique and its limitations. The results of the extraction of the first 111 roots in 72 patients have recently been published.3 Overall, 83% of teeth were successfully extracted, with the success rate being higher in single-rooted teeth (89%) when compared to multi-rooted teeth (43%). It is important to note that the study was limited to teeth not suitable for forceps extraction, did not include maxillary molars or mandibular third molars and did not include teeth with increased tooth mobility. Perhaps the most exciting finding was that, overall, only 7% of teeth required surgical removal (flap reflection and/or bone removal following failure to extract the tooth with the Benex system), although the surgeons estimated that 44% of teeth would have required a surgical approach had the Benex system not been used. This suggests that a significant proportion of teeth that would otherwise require a surgical approach can be successfully extracted with the Benex system.
Failure to complete an extraction with the Benex system in our experience can usually be attributed to one of two main reasons. Firstly, the root morphology may not be compatible with vertical extraction (Figure 6), which is often impossible to ascertain from a standard radiograph. Secondly, failure may occur as a result of insufficient retention of the screw and/or the root fractures. This can either be due to caries or failure to place the screw in an ideal position into the centre of the root. In our experience, this was a particular problem with slender roots, such as mesial roots of lower molars (Figure 7).
In order to achieve an optimal force vector for tooth extraction and to avoid complications such as screw bending, the pullstring should be perfectly aligned with the screw. This is easy to achieve with the Benex system as the transmission wheel offers some flexibility to move the extractor mesially or distally in order to achieve optimal alignment. If this is insufficient, the impression tray should be used in order to achieve alignment, even if neighbouring teeth are present (Figure 8a). Alternatively, an angled support disc has recently been developed to facilitate achieving the correct alignment of the pullstring with or without the aid of the impression tray (Figure 8b).
In our opinion this is a distinct advantage of the Benex system over the other two currently available systems, where vertical alignment of the force vector is not so easily achieved.
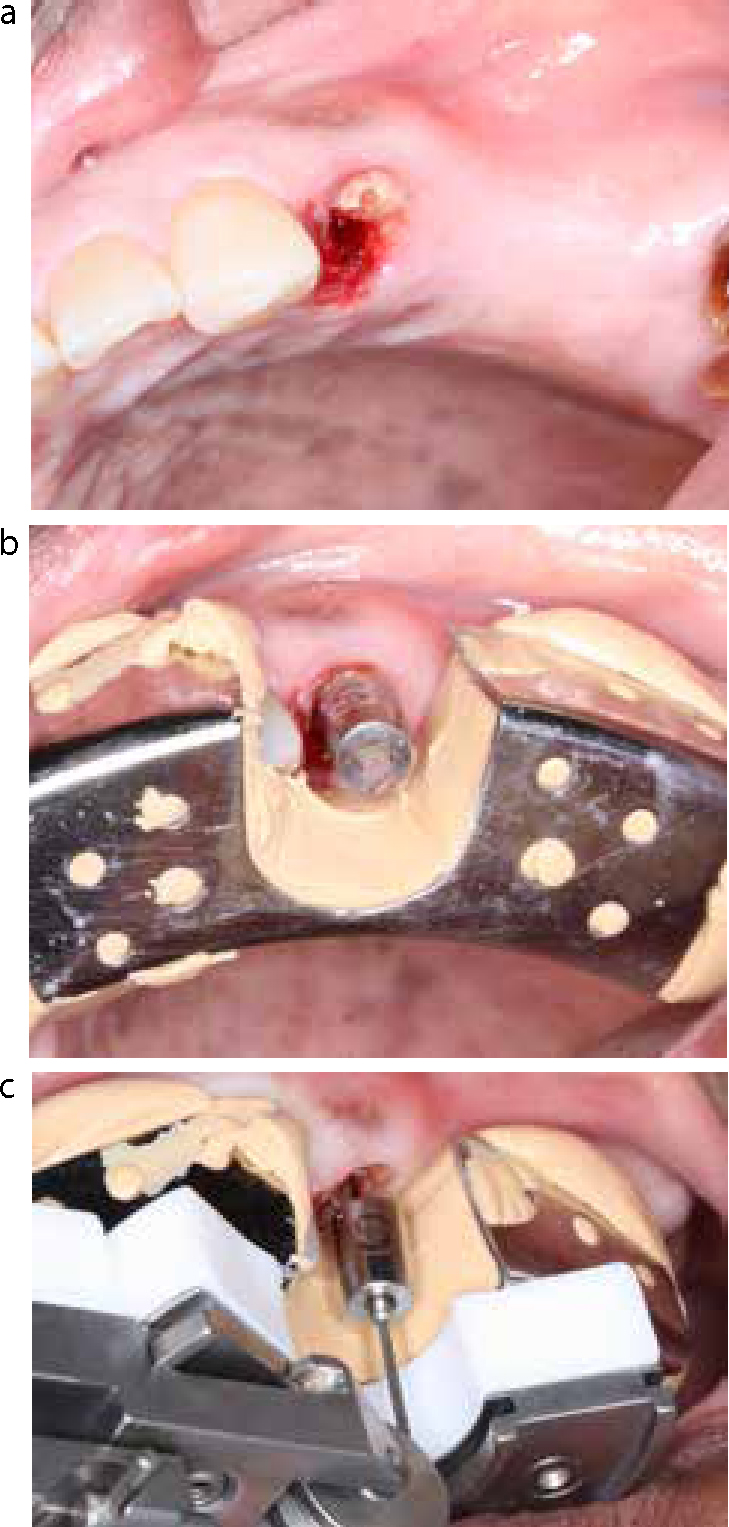
Use of the impression tray
The impression tray has several important functions. Firstly, the impression tray is necessary to provide stable support for the extractor in cases where adjacent teeth on either or both sides of the tooth to be extracted are missing (Figure 9a). However, it will often also provide more stable support when adjacent teeth are present, in particular with extractions in the anterior region. Secondly, the impression tray distributes the counterforce evenly across a larger area and it is therefore particularly suited for situations in which large forces are to be avoided (eg restorations, cantilevers). Thirdly, the impression tray may be necessary to achieve optimal vertical alignment of the pullstring (Figure 9b, c). For all these reasons, use of the impression tray is often necessary or advisable; in our study it was used in 3 out of 4 cases.3
Upper premolars constitute a particular challenge as they are often multi-rooted, and the exact root morphology, ie whether or not the roots are divergent, cannot be ascertained from standard radiographs pre-operatively. Based on our experience, we therefore recommend to place the screw initially in the centre of the root. If the tooth is single-rooted or multi-rooted with non-divergent roots, this will typically result in successful extraction of the tooth, even if some perforation of the furcation may have occurred (Figure 10). In cases of divergent roots, the tooth is unlikely to yield, and the roots can then be sectioned by extending the hole in a mesiodistal direction. The roots can then be approached separately.
In contrast to the manufacturer's instructions, we do not recommend any luxation of the tooth to be extracted as this would contradict the minimally invasive principle of the vertical extraction. However, if the tooth does not yield to a sustained input of a significant extraction force, luxation of the tooth can be attempted while the extraction force is being applied (Figure 11). In our study, luxation was performed in only 5% of successfully extracted teeth, some of which had been luxated as part of a previously failed routine forceps extraction. In conclusion, the vast majority of successful Benex extractions can be achieved without luxation.
In theory, minimally invasive vertical extraction methods may have several benefits compared to conventional extractions using luxators and/or forceps, which are listed in Table 1. However, it is important to note that, at present, none of these benefits has been scientifically validated in a robust manner.
While some of the advantages of the vertical extraction method, such as avoidance of flap surgery, are most obvious for root remnants not suitable for forceps extraction, the use of the system is by no means limited to such cases. Teeth do not necessarily have to be decoronated prior to removal, as it is possible to extract complete teeth by placing the screw into coronal enamel and dentine (Figure 12).
Contra-indications to use of the system are multi-rooted teeth with divergent roots that cannot be sectioned and clinical situations in which the extractor cannot be appropriately applied owing to limited access.
Reduced post-extraction bone resorption and preservation of residual alveolar height and width
Reduced trauma to alveolar bone and soft tissues in high-risk patients (eg patients on bisphosphonate medication, patients post-radiotherapy) to reduce incidence of complications
Reduction in flap surgery
Improved patient satisfaction, clinical procedure more acceptable to the anxious dental patient
Reduced post-operative morbidity
Less risk to anatomical structures – mental nerve, maxillary sinus
Improved post-operative soft tissue aesthetics
Improved success of intentional reimplantation/autotransplantation due to minimized trauma to periodontal tissues
Conclusion
Perhaps our forefathers with their doorknobs and strings were on to something after all. It just took us a hundred years to finally realize!
Based on our experience, we recommend the Benex system for extraction of incisors, canines and premolars. In selected cases, it may also be useful for extraction of molar roots, in particular the distal roots of mandibular molars and the palatal roots of maxillary molars. It may also be used for extraction of impacted teeth in selected cases, in the context of a surgical extraction to minimize bone removal.